
Abstract
OBJECTIVES:
Muscle energy technique (MET) is a voluntary contraction of a patient’s muscle in a predetermined direction, at varying levels of intensity. Its commonly used as a treatment option in musculoskeletal rehabilitation. This study aims to investigate the effectiveness of MET in the treatment of people with musculoskeletal injuries with particular emphasis on flexibility, range of motion (ROM), and function.
METHODS:
Scopus (via Science Direct), CINAHL via (EBSCO), Embase (via OvidSP), PubMed, and PEDro were searched using specified keywords to select randomized controlled trials that assessed the effect of MET on flexibility, ROM, or function in patients with musculoskeletal disorders. Two authors extracted all related information from the included trials and presented them in an excel spreadsheet. Two other authors independently conducted the quality assessment. Meta-analysis was performed where homogeneity (similirty regarding population and outcomes) was sufficient and required data were available.
RESULTS:
A total of 42 studies were included. Yet, twelve joined the meta-analysis where six comparisons were conducted. Of them, four comparisons were composed of two trials, one comparison consisted of six, and another one was composed of four. No statistically significant differences were observed between MET and other comparators regarding function and ROM, especially in patients with low back or neck pain. MET was statistically significantly better than control or sham interventions on the flexibility of patients with sacroiliac joint (SIJ) problems.
CONCLUSIONS:
MET can produce better flexibility than placebo and control interventions in patients with SIJ problems. MET is not better than other interventions regarding function and ROM. Although the existence of multiple trials testing the effectiveness of MET, there is obvious heterogeneity. There is no sufficient evidence to reliably determine the clinical effect of MET in practice.
Introduction
Muscle energy technique (MET) is a gentle technique used in clinical practice by a wide range of manual therapy practitioners, including physiotherapists and osteopath practitioners [1]. According to Burke and colleagues, more than 14% of Australian osteopathic practitioners use MET in their clinical practice [2].
It is characterized by the participation of the patients through active muscular effort (isometric or isotonic) [3]. The isometric version of the technique is most commonly employed and involves specific components: 1. Localization of joint/muscle barrier by the operator (controlled joint positioning); 2. Patient active muscle contraction in a specific direction for a specified time; 3. Operator-applied distinct counterforce against the patient contraction; 4. Patient relaxation; 5. Operator re-uptakes the ‘new’ barrier (passive stretch of the muscle, or increase in joint movement in a specific direction); 6. Repeat the procedure several times [1]. This technique aims to reduce pain, improve joint mobility, improve tissue flexibility, treat hypertonic muscles, and improve musculoskeletal integrity [3–6].
The physiological mechanisms that underpin MET are unclear. However, it is thought to act through a complex interplay of neurophysiological mechanisms which affect tissue extensibility and tolerance due to pain modulation [5, 7]. The contractions and positions used in the treatment of MET can also stimulate the fascial tissue and enhance the mobility of the region [8]. MET results in decreased muscle tone and sympathetic tone as well as localized vasodilatation by providing fascial stimulation [9].
Musculoskeletal injuries are the commonest type of injuries seen in the physiotherapy field [10–12]. The impact of musculoskeletal disorders is obvious, they account for 2% of the domestic product yearly in Europe [13]. In Sweden, neck and back pain patients represented approximately 7% of the national expenditure on health services due to sick leave. It has been estimated that around 49.9% of sick leave lasting more than three days in Europe is due to musculoskeletal pain. Around 77% of the reduction in work productivity was due to pain [14].
Previous literature showed that MET could be beneficial on a variety of occasions; the joint range of motion, as well as soft tissue flexibility, were better after MET [15–20]. Pain and function improved in several studies [20–23]. Additionally, muscular strength and endurance demonstrated significant improvement in other studies [3, 22].
Recently, several reviews were conducted to assess the efficacy of MET in a variety of medical conditions such as low back pain [24], neck pain [25, 26], and chronic obstructive lung diseases [1]. Another review did not consider specific pathology [27]. Of them, only one meta-analysis was conducted [24] while the others were systematic reviews [1, 25–27]. All these reviews used a single tool for assessing methodological quality which could limit the ability to fully cover the items that represent the study quality [28]. Additionally, many musculoskeletal conditions were not covered in these reviews.
This systematic review and meta-analysis aimed to investigate the effectiveness of MET in the treatment of a limited joint range of motion (ROM), flexibility, and functional disability in subjects with musculoskeletal disorders.
Methodology
The protocol of this systematic review was registered on the PROSPERO registry [CRD42022333502]. It was designed per the PRISMA guidelines for reporting systematic reviews and meta-analyses.
Inclusion criteria
Studies were included if they met the following criteria: 1) randomized controlled trials (RCTs); 2) no age restriction 3) the sample consists of subjects having musculoskeletal dysfunction 4) The intervention of interest is MET which could be used as a single treatment compared to none, sham, placebo, or other intervention protocol. 5) Outcomes of interest were joint ROM measured by a clinical tool (goniometer, inclinometer), muscles flexibility using flexibility testing, and function level using any functional scales or questionnaires; 6) articles published in English were included
Information sources
Scopus (via Science Direct), CINAHL via (EBSCO), Embase (via OvidSP), PubMed, and PEDro were searched between the 1st and 7th of August 2022. Searches were supplemented by hand searching and retrieval of any additional articles meeting eligibility criteria that were cited in reference lists.
Search strategy
Two authors searched the selected databases for the RCTs that meet the inclusion criteria mentioned before. The search keywords were MET (muscle energy technique, MET, post-isometric contraction and variants), and randomized controlled trials (randomized controlled trial, controlled clinical trial and variants), range of motion, flexibility, function, and disability.
Study records
Data collection and management
Found records were uploaded to www.Rayyan QCRI.org [29], an Internet-based software program that facilitates collaboration among reviewers during the assessment of studies against the inclusion and exclusion criteria. Before the formal screening process, a calibration exercise was performed to pilot and refine the screening procedures and to familiarize the screening team with the Rayyan software.
The team developed a table using Microsoft Excel 2016 spreadsheet to gather the characteristics of the eligible studies. These characteristics included the author’s name, year of publication, the setting, and country of the study, outcome measures, MET parameters, and sample size. Review manager software 5.4 were used to manage the data that could be used to conduct the meta-analysis.
Selection process
The Rayyan software was used to help in assessing the studies against the inclusion criteria, refining to remove duplicates. Two authors independently conducted this procedure. In case of uncertainty, the full article was downloaded and reviewed. An email was sent to the corresponding author to obtain any missing or incomplete data. Any disagreement between the reviewers was solved by the opinion of a third reviewer. The reasons for exclusion were recorded.
Methodological quality assessment
Seven common scales (Delphi List, PEDro, Maastricht, Maastricht-Amsterdam List, Bizzini, van Tulder, and Jadad) were incorporated to form one list of items that covers five areas: patient selection, blinding, intervention, outcomes, and statistics. This incorporated form was used to overcome the limitations of every single scale [30, 31]. This method of quality assessment was performed in previous systematic reviews [28, 32].
For each item listed on the critical appraisal sheet, a score of 1 was given to achieved items, and a score of 0 was given to neglected items. In cases where the study did not consider a particular item (According to its original design), the item was marked as not applicable (NA). Items that were not clearly stated in the study were labeled with the symbol?.
The scoring for each study was calculated by dividing the number of achieved items (1) by the total number after excluding the NA items (Table 2). Finally, each study was graded as having low, moderate, or high methodological quality based on how many items from the critical appraisal were met. The cutoff was determined as follows: 0– 0.40 for low methodological quality, 0.41– 0.70 for moderate methodological quality, and 0.71– 1.00 for high methodological quality [28].
Data synthesis and analysis
Studies investigating similar outcomes and interventions in addition to those providing clear quantitative data were grouped, evaluated for heterogeneity, and pooled, if possible. If a grouping of the outcome data was not applicable, descriptive, and qualitative summaries were used.
Results
A total of 1630 articles were retrieved from databases. There were 56 duplicates removed and 1574 were exposed to screening for eligibility through the revision of the title and abstract. Of these, 1518 articles were excluded, and 56 trials were considered eligible and furtherly subjected to detailed assessment where 14 studies failed to meet the inclusion criteria due to adopting different research designs [3, 21, 33–36], lack of randomization [37–39], using undesired study population [40–43], and lack of text written in English [44]. A single trial [45] was added after searching the reference list of the related trials. So, the final number of the included trials was 43[6, 16, 22, 23, 43, 45–82]. The final decision on the inclusion was taken by consensus between the three reviewers (Fig. 1).

Flow diagram.
The included 43 trials addressed a total of 2370 participants where low back dysfunction was investigated in twelve trials [45, 48, 49, 56, 57, 68, 70, 73, 74, 76, 77, 82], neck pain was investigated in nine trials [6, 23, 53, 60–62, 69, 78, 79], trigger points were investigated in five trials [46, 51, 54, 64, 75], shoulder dysfunctions were assessed in six trials [43, 50, 58, 65, 66, 80], and Sacroiliac joint (SIJ) was investigated in five trials [47, 52, 59, 72]. Additionally, elbow joint pain/dysfunction [16, 22] and cervicogenic headache [71, 81] were investigated in two trials each. Finally, piriformis [55] and upper crossed [67] syndromes were assessed in a single trial.
The effectiveness of MET was compared to other single interventions in 18 trials [6, 22, 58, 59, 62, 64, 65, 73, 75, 76, 33, 46, 48–51, 55, 57] representing 42% of the included trials where manual therapy [49, 50, 57, 59, 65], stretching techniques [6, 58], and trigger point therapies [46, 51, 55, 64] were the comparative treatments. Other studies compared MET against dry needling [75], corticosteroid injections [22], and exercises [48].
The effect of adding MET to standard treatment was compared to either the standard treatment [45, 68, 71, 74] or other interventions plus standard treatment [23, 43, 53, 56, 60, 61, 63, 66, 67, 69, 78–80, 82]. Additionally, three trials [6, 52, 54] incorporated a sham or placebo as a control condition.
On the other hand, two studies [70, 72] used MET in the standard treatment where it was delivered to both the study and control groups. Other characteristics of the included trials were summarized in Table 1.
Main characteristics of the included trials
Main characteristics of the included trials
TPT, Trigger Point Therapy; SIJ, Sacroiliac joint; ttt, treatment; MET, muscle energy technique; ROM; range of motion; LBP, low back pain; n, sample number; TMJ, tempromandibular joint; LE, lateral epicondylitis; SWD, shortwave diathermy; NPRS, numeric pain rating scale; US, ultrasound.
The determination of the methodological quality was conducted by two independent reviewers and whenever there is a contradiction, a discussion till reaching a consensus was conducted. Out of the 43trials, five trials [16, 57, 62, 69, 81] were of high quality (score ≥70%), 27 trials [6, 22, 23, 46, 47, 49, 52–56, 58, 60, 61, 63–68, 70–73, 75, 79, 82] were of moderate quality (score between 40– 69%), and eleven trials [36, 43, 45, 48, 50, 51, 59, 74, 77, 78, 80] were of low (score ≤39%) methodological quality.
There are a few points regarding quality that need to be clarified. First, the appropriate sample size was calculated in 26 out of the 42 trials representing 61.9%. Second, four trials only (9.5%) used the double-blinded design. Third, eleven trials were not described clearly as randomized. However, the randomization process was indirectly reported in the methodology section. Fourth, the majority of the trials (39 representing 92.8%) did not consider reporting the adverse effects of the interventions. Finally, the follow-up design was implemented in seven trials only where it was short in 85.7% of them (Table 2).
Results of the quality assessment of the included trials
Results of the quality assessment of the included trials
1, eligibility criteria mentioned; 2, the study described as randomized; 3, was the method of randomization mentioned?; 4- does randomization described appropriately; 5, randomization concealed; 6, baseline comparability (both groups are similar before treatment; 7, the study described as double blinding; 8, blinding described appropriately; 9, blinding of investigator/assessor; 10, blinding of subject/patient; 11, blinding of therapist; 12, blinding of the outcome / statistician; 13, treatment protocol adequately described for the treatment and control groups; 14, control and /or placebo treatment adequately described; 15, were cointerventions avoided? (other treatments than used in the study i.e. drugs); 16, cointervention reported for each group separately; 17, control for cointerventions in design; 18, testing of subject adherence; 19, adherence acceptable in all groups; 20, description of withdrawals and dropouts; 21, withdrawals/dropouts rate described and acceptable (up to 20% acceptable); 22, reasons for dropouts; 23, adverse effects described; 24, follow-up details reported; 25, follow-up period adequate; 26, short follow-up performed; 27, timing of outcomes comparable in all groups; 28, description of outcome measures; 29, relevant outcomes included; 30, validity reported for main outcome measure; 31, responsiveness reported for main outcome measure (reporting mean difference / effect size); 32, reliability reported for main outcome measure; 33, use of quantitative (objective) outcome measures; 34, Descriptive measures (point estimates, measures of variability) identified and reported for the primary outcome; 35, appropriate statistical analysis included; 36, sample size calculated periori; 37, adequate sample size - proper justification of the used sample; 38, sample size described for each group; 39, intention-to-treat analysis included; H, high quality; M, medium quality; L, low quality.
Due to the high percentage (76.1%) of the RCTs which had medium to high quality, the low-quality RCTs were excluded from the further meta-analysis. Additionally, trials that included the MET in the standard treatment [70, 72] where it was introduced to both study and control groups were also excluded. Other trials that lacks the necessary data [73] or were heterogeneous regarding the outcome measures [46, 64] were also excluded. Finally, 14 trials were grouped according to the investigated population then according to the nature of interventions to make homogenous groups then analyses were performed using REV MAN 5.4 software.
MET and low back dysfunctions
Comparison 1: Effect of MET on function in Low back pain conditions
In this subanalysis, two trials met the criteria and were included in the comparison. In these trials, Met was compared to manipulation [49] or spinal stabilization exercises [57]. As shown in Fig. 3, there was no statistically significant difference between MET and comparator intervention where the standardized mean difference (SMD) was – 0.33 with 95% CI between – 0.67 and 0.01. The SMD showed a trend favoring the MET (Fig. 2) yet, it was not high enough to reach a statistically significant effect (z = 1.89, p = 0.06). The 95% CI of both trials was relatively in the same range hence the homogeneity was evident (I2 = 0%).
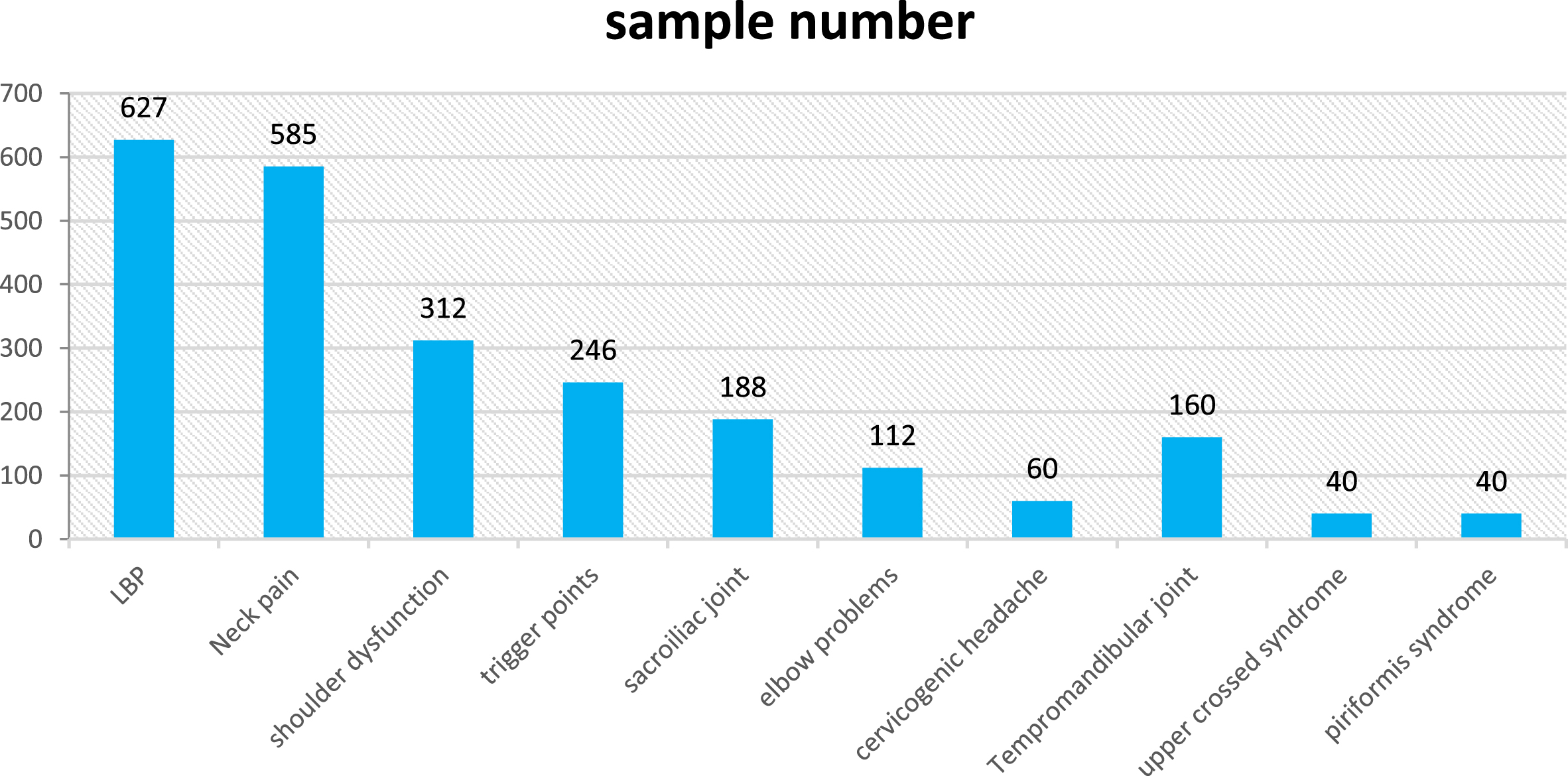
The population number in each diagnosis of the included studies.

Forest plot for the effect of MET versus other single treatments on the function of patients with LBP.
In this sub-analysis, two [56, 82] trials studied the effect of MET plus standard treatment versus other interventions plus standard treatment on ROM. The comparator interventions were kinesio-tape [56] and pilates exercises [82].
As shown in Fig. 4, there was no statistically significant difference between the two treatment conditions where SMD = 0.22 with 95% CI between – 0.14 and 0.58. Additionally, the 95% CI of both trials was relatively in the same range hence the homogeneity was evident (I2 = 0%).

Forest plot for the effect of MET + standard treatment versus other intervention + standard treatment on ROM in LBP.
Under this category, six trials met the inclusion criteria and were grouped for subanalysis. All trials compared MET plus standard treatment versus other interventions plus standard treatment. function and ROM were the outcomes of interest in all trials except two [60, 79] where function only was the outcome of interest.
Comparison 3: Effect of MET on function in patients with neck pain
This sub-analysis demonstrated a high degree of heterogeneity between the included trials (I2 = 93%, p = 0.000). The weight was distributed equally between all trials in this comparison. There was no statistically significant difference between MET and the comparator treatment where the SMD = – 0.38 and the 95% CI was between 1.40 and 0.64 (Fig. 5).
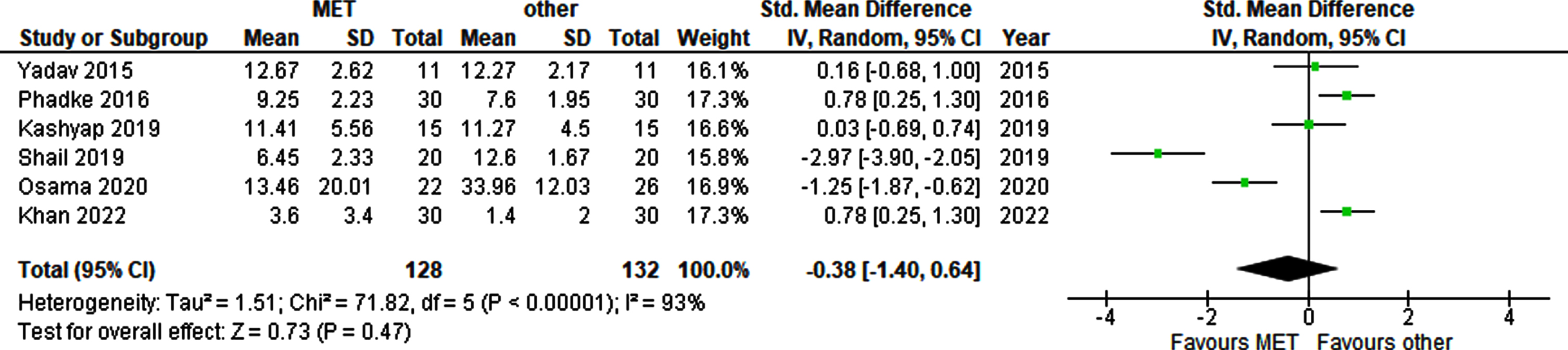
Forest plot for the effect of MET + standard treatment versus other intervention + standard treatment on the function in neck pain.
In this sub-analysis (Fig. 6), the weight of all trials was distributed in a balanced fashion. High variabilities in the 95% CI was reported hence the heterogeneity was statistically significantly high (I2 = 85%, p = 0.0002). The SMD shows a slightly better effect in favor of the comparator interventions on ROM (SMD = – 0.62) with 95% CI between – 1.14 and – 0.10. Yet the heterogeneity raises caution when dealing with this finding.

Forest plot for the effect of MET + standard treatment versus other intervention + standard treatment on ROM of patients with neck pain.
In this sub-analysis, two trials [6, 75] used a CROM device to assess the ROM of cervical lateral flexion. The comparator interventions were dry needling [75] and passive stretch [6]. The heterogeneity was significantly high I2 = 94%. There was no statistically significant difference between MET and other interventions. The SMD = – 0.19 and the 95% CI was between – 0.64 and 0.26 (Fig. 7).

Forest plot for the effect of MET versus other single treatments on cervical ROM of patients with trigger points.
In this comparison, two trials were conducted by Vaseghinia et al. [47, 52] where MET has compared to sham [52] or control [47] conditions. The outcome of interest in this comparison was the flexibility that demonstrated statistically significant improvement (z = 4.48, p < 0.000) in patients who received MET. It is worth mentioning that there was a high degree of heterogeneity (I2 = 97%) in this analysis which raises caution when considering the current results (Fig. 8).

Forest plot for Forest plot for the effect of MET versus other single treatments on the flexibility of patients with SIJ problems.
The current meta-analysis showed that MET was better than the control or placebo on the flexibility of patients having SIJ problems. Yet, MET was not better than other interventions (manipulation, spinal stabilization exercises, and McKenzie) on function and ROM in patients with low back or neck pain.
This finding could be limited by the low number of analyzed trials (n = 2), especially in LBP, the analyzed trials used different tools for functional assessment (Roland & Morris and Oswestry disability index). Additionally, two different devices were used to assess ROM where Elshinnawy trial [56] used an inclinometer, El Gendy trial [82] used a BROM II device.
Another reason for this result could be the variation of the MET technique used, in Ulger study [57] no clear information was provided regarding the treated muscles while in the Sturion study [49], quadratus lumborum and piriformis muscles were treated. Similarly, upper trapezius, scalenes, and levator scapulae muscles were treated by Osama [61] and Yadav [53] studies, while others treated single muscles as the trapezius [23] or scalene [79].
Additionally, a different number of muscles were treated with MET in different trials. Moreover, there were obvious variations in the nature and number of modalities used in the standard intervention, while heat and exercises were used by Phadke et al. [60]. The other trials used multiple modalities. The observed effects could be attributed to the variation between the analyzed trials regarding the duration of treatment (from 6 days to 30 days), and the details parameters of the MET technique which were evident in the contraction time, stretching time, and technique repetitions per session.
The previous literature contains a single meta-analysis [83] and three systematic reviews [25–27]. The meta-analysis was concerned with LBP, two reviews were concerned with neck pain [25, 26], and the last review was conducted on multiple symptomatic and a symptomatic populations [27].
The results of the current meta-analysis were consistent with those reported by Franke et al. where MET did not show any significant difference compared to other interventions on the function of patients with LBP [24]. Franke meta-analysis was conducted on twelve trials where seven comparisons were performed. Five of them included only a single study.
On contrary to the current review, the previous systematic reviews reported beneficial effects of MET on ROM [25–27] and function [25]. It is worth reporting that the above-mentioned reviews used different Quality assessment scales (PEDro and standard quality assessment criteria) than the one adopted by the current meta-analysis, the low number of included studies (n = 5) [25], the heterogeneity in MET parameters [27], and the low methodological quality [26] could be attributed to the results of these reviews.
Methodological elements affecting observed effects
Although high and medium-quality trials only were included in the meta-analysis, various methodological biases were observed that might affect the results. demonstrated various methodological biases such as randomization where five out of the twelve trials failed to report the randomization sequence and procedures clearly, while concealment was not considered in eight trials. Another source of bias could be blinding where three trials only were reported as double-blinded [52, 57, 82]. This lack of data regarding the randomization method, concealment, or blinding might affect the accuracy of the results reported by research trials.
The third source of potential bias could be the sample size that was not appropriately calculated in 50% of the analyzed trials (n = 6). Additional factors, such as reporting the validity and reliability of the main outcome measure were reported in six and seven trials respectively, lack of such information could influence the observed effects. All of the analyzed trials (100%) ignored the data regarding the adverse effects and intention-to-treat procedures.
As suggested previously [28], trials should report the clinical significance of their results to show the real rather than the statistical significance of the investigated intervention. Clinical significance reflects the presence or absence of a clinical impact of intervention because it can identify when a meaningful change is produced. However, its importance and reporting of clinical effect were considered in only two [57, 82] out of the twelve analyzed trials.
Summary of evidence
In low back pain, MET alone was not statistically better than other interventions such as manipulation and spinal stabilization exercises regarding function. Additionally, MET was not better than other interventions such as Pilate exercises and kinesio-taping when standard treatment was added to both interventions. Similarly, findings were evident in patients with neck pain where MET plus standard treatment was not better than other interventions (exercises, stretching, myofascial release, passive stretching, and mobilization). Yet, the authors observed a small trend suggesting more improvement in function in groups that received MET. On the other hand, the flexibility of tissues in patients with SIJ dysfunction demonstrated better improvement compared to placebo or control conditions.
Strengths
To the authors’ knowledge, this meta-analysis is one of the few that analyzed the effect of MET on different musculoskeletal problems. A systematic search was made to cover the recently published randomized trials (last 10 years) to reach conclusions based on the most recent evidence. Randomized trials of high and medium quality only were analyzed, the quality of these trials was determined based on integrated items extracted from seven popular scales to cover the majority of aspects that should be included in a good trial. In the current meta-analysis, five analyses were conducted to group the most homogenous trials together using well-defined criteria.
Limitations
The limited number of high-quality trials hinders the analysis of the effects of MET on certain populations (trigger points, cervicogenic headache, piriformis syndrome, upper crossed syndrome, and temporomandibular joint). The authors chose to compare the range of extension movement only if the trial measured more than one movement, this movement was particularly used because it was the common movement measured in the majority of the trials. Some trials were excluded from analysis due to differences in outcome measures and a lack of reporting important data that could not be determined using the REV MAN software calculator.
Conclusions
Implications for practice
MET as a single treatment could have a beneficial effect on flexibility in patients having SIJ problems when compared to control or placebo. The addition of MET to standard treatment might not add any additional benefits to function and pain, especially in LBP and neck pain. The small number of trials patients prevent conclusive statements regarding the effectiveness of MET, especially in LBP. There is no clear evidence about the long-term effect of MET on different musculoskeletal problems.
Implications for research
More trials are needed to investigate the effects of MET on different musculoskeletal problems. Items related to quality should be addressed in future studies. These items include consistent outcome measures, reporting validity and reliability of the outcome measures, reporting of the adverse effects, and investigating medium- and long-term effects of the MET.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
None.