
Abstract
BACKGROUND:
The trapeziometacarpal or first carpometacarpal (CMC) joint is the second most common joint affected in osteoarthritis (OA) of the hand. Surgical intervention may be required when conservative measures fail to alleviate symptoms.
OBJECTIVE:
To investigate operative and post-operative management of trapeziometacarpal osteoarthritis in Ireland.
METHODS:
An on-line Qualtrics survey was used to determine practice patterns of hand surgeons and therapists including surgical technique, patterns of referral to therapy, treatment protocol and perceived pain impact.
RESULTS:
Twenty surgeon’s responses were received. Trapeziectomy with Ligament Reconstruction and Tendon Interposition (LRTI) was the most common procedure for all stages of arthritis for sedentary and manual patients. Sixty seven percent (n = 18) stated they perform an additional procedure if stage IV arthritis is present. Eighty percent (n = 16) stated they would perform an additional procedure for MCP joint hyperextension.
There were 28 therapist responses. Almost all respondents indicated that patients are initially casted post-surgery with 88% (n = 24) indicating they remain casted for 1-2 weeks. A rigid long thumb spica and neoprene splint are most commonly used. The commencement of exercises differed between respondents and surgical procedures. All participants stated that pain is an issue in the rehabilitation of these patients.
CONCLUSIONS:
There was consistency in the surgical procedure choice. The stage of arthritis and functional level of the patient was not found to be an important factor for choosing this procedure. There is some consensus for post-operative casting and splinting but more variability in terms of exercise prescription. Pain is a factor to consider post-operatively.
Keywords
Introduction
The trapeziometacarpal or first carpometacarpal (CMC) joint is the second most common joint affected in osteoarthritis (OA) of the hand [1]. Surgical intervention may be required when conservative measures fail to alleviate symptoms [2]. The purpose of this study was to investigate the operative and post-operative management of trapeziometacarpal osteoarthritis in the Republic of Ireland by surveying hand surgeons and hand therapists on their practice.
The radiographic prevalence of CMC OA is reported to be as high as 91% in adults over 80 years of age [3]. Symptoms include pain, instability, weakness, and impaired function particularly with activities requiring pinch and power grip [4, 5]. CMC OA can be classified based on its radiographic appearance into four stages (Eaton-Littler classification), [6] see Table 1. Early stages and less symptomatic cases can be treated with conservative management when this is no longer sufficient to reduce pain and disability, surgical intervention may be indicated [2].
Eaton-Littler classification
Eaton-Littler classification
Abbreviations: CMC, carpometacarpal; STT, scaphotrapeziotrapezoidal.
The association between radiographic findings and clinical symptoms vary meaning that the stage of arthritis on x-ray does not always correspond with the severity of symptoms [7]. The decision to perform surgery is largely based on the individuals pain levels and loss of function [8, 9].
Several surgical procedures are reported and there is no consensus in the literature on which procedure is most effective in treating this condition [9, 10]. Surveys of practice have been carried out in Europe [2, 5] and the US [11–13] to determine which procedures are most commonly performed. The procedure of choice from all but one of the surveys [14] was trapeziectomy with Ligament Reconstruction Tendon Interposition (LRTI). This procedure involves removal of the trapezium and reconstruction of the ligament by harvesting a tendon from the forearm and passing it through the base of the first metacarpal [15]. The remaining tendon is interposed in the space left by the trapezium [15].
Post-operative recommendations on splinting and exercise are varied regarding immobilisation and in the prescribed exercises [16]. A systematic review in 2018 found that a shorter immobilisation time of 4–6 weeks or less and an earlier commencement of exercises at 4 weeks or less have positive effects on pain, grip, and activity [17]. A US practice survey of hand therapists on post-operative management published in 2020 determined that ‘multiple therapy programs’ exist which are guided by clinical experience [18]. To date there has been no European survey of practice.
This study sought to determine the operative and post-operative management practices in Ireland. A cross-sectional on-line survey using a descriptive design was used. This method has been used previously to examine practice patterns from surgeons and therapists on this topic [2, 5, 18]. Ethical approval was obtained from the School of Medicine Research Ethics committee, Trinity College, Dublin. Consent was gathered at the start of each survey.
Questionnaire
Development of surgeon and therapist questionnaires was informed by the literature, expert practice experience and piloting. The surgeons’ questionnaire was designed to identify the preferred surgical techniques based on stage of arthritis and functional level pre-surgery, any additional procedures performed during the surgery and patterns of referral to therapy. The therapist questionnaire sought to identify treatment protocols, preferred splinting, range of motion, strengthening programmes and perceived pain impact post-surgery. The on-line survey platform Qualtrics was used for data collection with the surveys remaining open for two months in 2021.
Recruitment
Consultant grade hand surgeons and hand therapists practicing in Ireland were invited to participate if they had treated this cohort in the last year. Recruitment was conducted via the Irish Hand Surgery Society (IHSS) and the Irish Association of Hand Therapists (IAHT). To ensure all potential therapists that treat this patient group were contacted, the survey was distributed via email through the Irish Society of Chartered Physiotherapists (ISCP) and Occupational Therapy and Physiotherapy hospital managers.
There were 20 responses to the surgeon’s survey which represents a 42% response rate based on membership of IHSS at the time. This was considered an accurate rate as not all members of IHSS would perform this surgery.
There was a total of 28 therapy responses, based on numbers of the IAHT in 2021 this represents a 39% response rate. Again it would be expected that not all members would treat this patient group and this number reflects the number of surgeon’s operating on this group.
An average response rate for on-line surveys is 44% [19].
The survey data was extracted from Qualtrics and descriptively analysed in Microsoft Excel.
Results
Surgeon’s survey
Demographic characteristics are provided in Table 2.
Surgeons Survey: Demographic characteristics of participants
Surgeons Survey: Demographic characteristics of participants
Figure 1 presents the number of each surgical procedure used for the treatment of trapeziometacarpal osteoarthritis performed within a six month period. The majority were performing five or less of each procedure within this time frame with three respondents stating that they performed up to 10 Trapeziectomies with LRTI. The only procedure that was performed 10 or more times in a six month period was a metacarpal osteotomy by one respondent. Trapeziectomy with LRTI was the most common procedure chosen and the majority of the respondents indicated that they never perform a denervation (n = 14) or metacarpal osteotomy (n = 13).
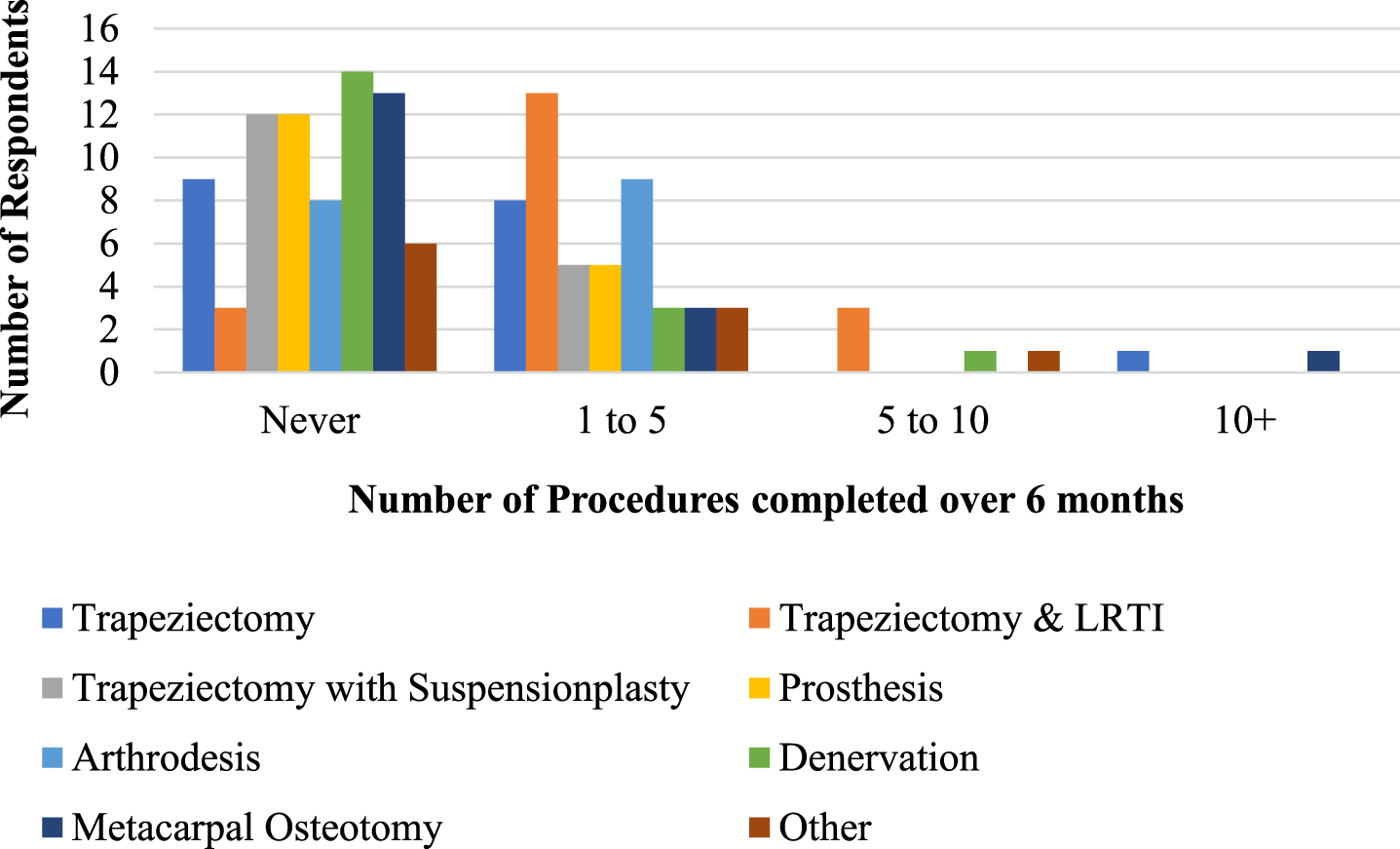
Surgical Procedures & Number completed over 6 months. Abbreviations: LRTI, ligament reconstruction with tendon interposition.
Figure 2 presents the procedure preferred by the surgeons for each stage of arthritis. Trapeziectomy with LRTI was the preferred procedure for all stages of arthritis for both sedentary and manual patients. Reasons were provided by 14 respondents for their preferred technique. See Table 3.
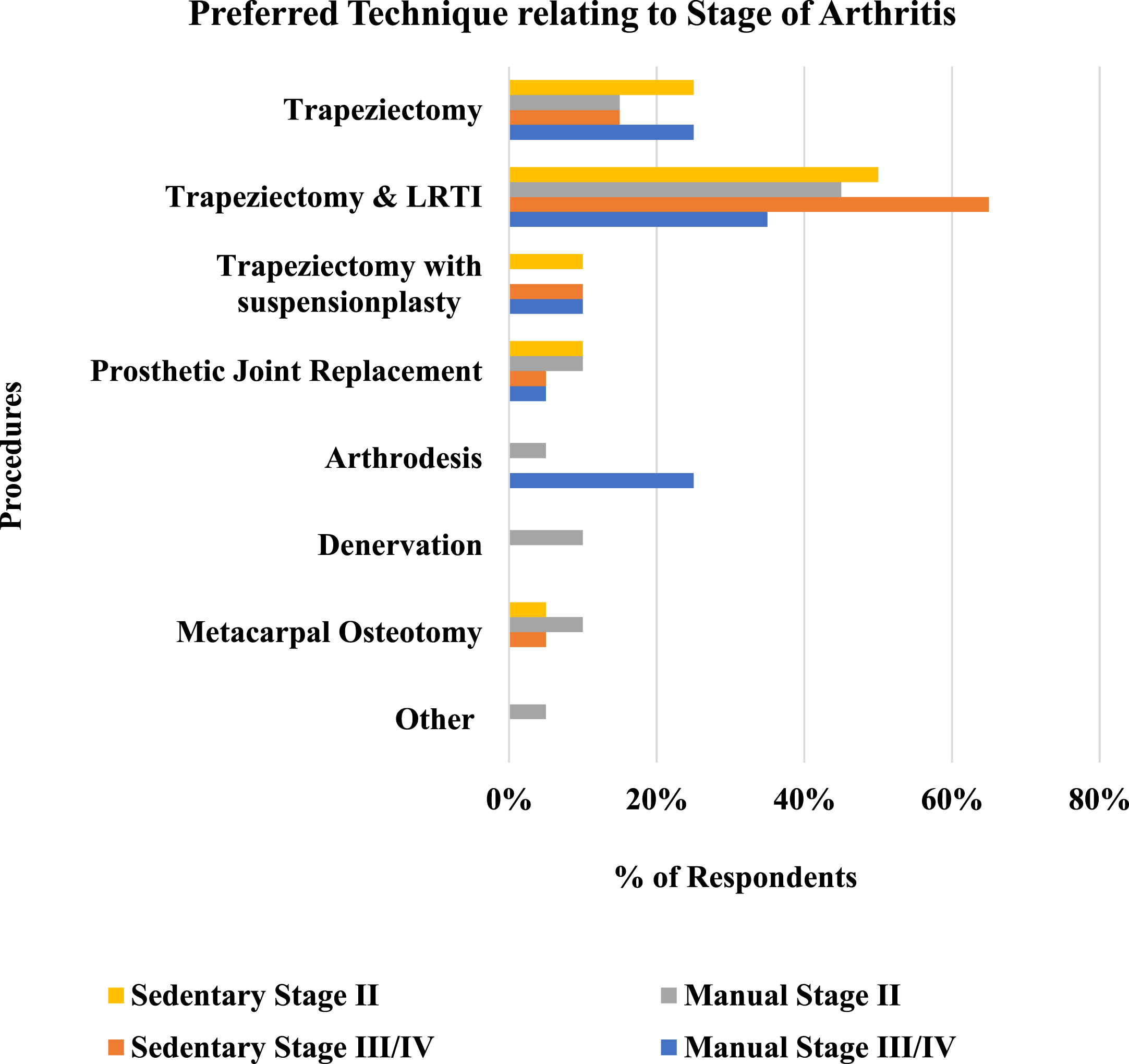
The preferred technique relating to stage of arthritis. Abbreviations: LRTI, ligament reconstruction with tendon interposition.
Reasons for choosing surgical procedure
Abbreviation: LRTI, ligament reconstruction with tendon interposition.
Sixty seven percent (n = 18) stated that they perform an additional procedure if stage IV arthritis is present. Four stated they would perform an arthroplasty of the STT joint while two surgeons specified that they would resect the proximal trapezoid.
Of the respondents the majority, 80% (n = 16), stated that they would perform an additional procedure if MCP joint hyperextension was present. Nineteen percent (n = 3) would perform a sesamoid fusion, 38% (n = 6) a capsulodesis/volar plate tightening and 44% (n = 7) an arthrodesis.
Referral rate to therapy was high. Seventy nine percent (n = 15) refer all patients, 16% (n = 3) refer over 50% of patients and 5% (n = 1) refer less than 50%. Respondents were asked what factors determine who is referred to therapy. More than one response could be chosen and there were 22 responses in total. Factors included the availability of therapy (n = 13), their own professional preference (n = 6), patient factors (n = 2) and other factors (n = 1). The comment in relation to other factors was that patients are referred for splinting.
Table 4 presents the characteristics of the participants.
Therapists survey: Demographic characteristics of participants
Therapists survey: Demographic characteristics of participants
Abbreviations: CMC, carpometacarpal joint.
Figure 3 presents the number of each surgical procedure treated within a 6 month period. Results show that the majority treat approximately 1 to 5 trapeziectomies (n = 15) and 1 to 5 trapeziectomies with LRTI (n = 15) over 6 months. Almost half of respondents indicated that they never treat patients following trapeziectomy with suspensionplasty with a foreign material (n = 14) or a prosthetic joint replacement (n = 13).

Procedures & Numbers seen in hand therapy practice over 6 months. Abbreviations: LRTI, ligament reconstruction with tendon interposition.
All respondents (n = 27) indicated that in their service patients are initially casted post-surgery with most (88%, n = 24) indicating that patients remain casted for 1-2 weeks. Figure 4 outlines post-splinting preferences and the week in which they commence.

Week each splint is commenced post-surgery.
Figure 5 presents the timeframes for discontinuing full time splinting. The majority 44% (n = 11) discontinue at Week 6, followed by 16% at Week 6–8 (n = 4) and 12% at Week 8 (n = 3).
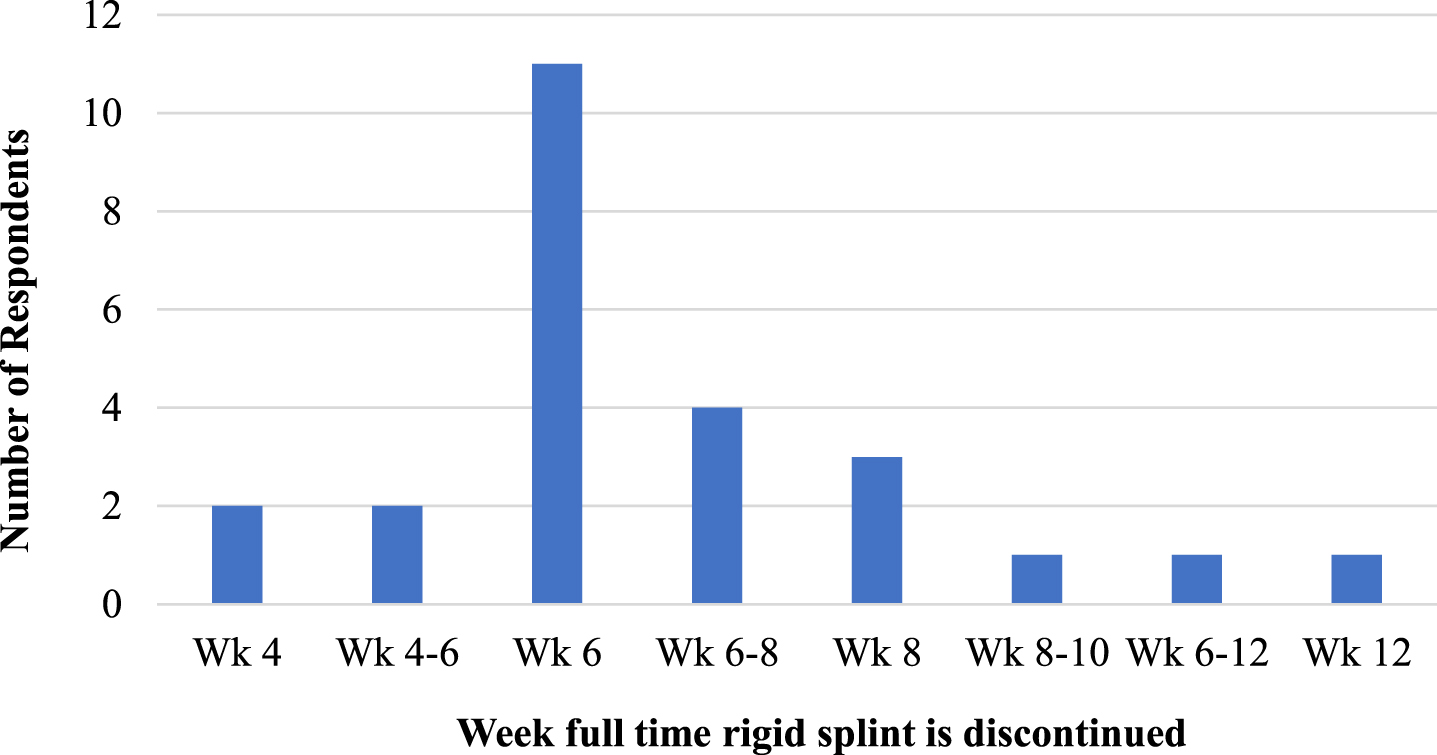
Week full time rigid splinting is discontinued.
Sixty four percent (n = 16) of respondents (n = 25) indicated that their splinting approach does not differ depending on the surgical procedure carried out. Of the respondents who do alter their splinting approach six people commented on factors that influence this decision (Table 5).
Reasons for changing splinting approach
Abbreviations: LRTI, ligament reconstruction with tendon interposition.
The commencement of MCP, CMC and wrist motion differed between respondents and surgical procedures (Fig. 6).
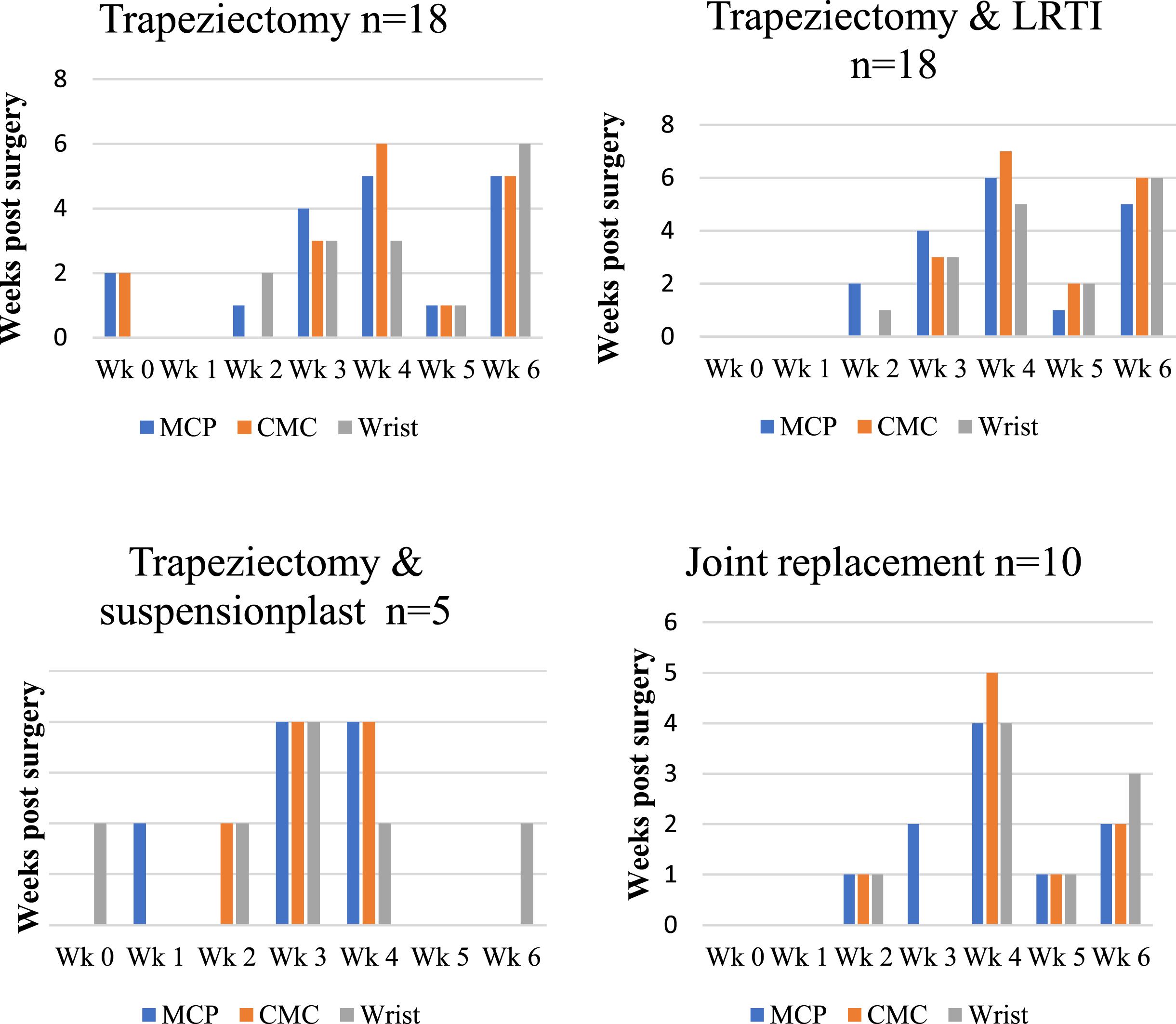
Commencement of MCP, CMC and wrist motion for each procedure. Abbreviations: LRTI, ligament reconstruction with tendon interposition.
All of the participants who responded to this question (n = 20) prescribe strengthening exercises with variation in the week of commencement. Nobody commenced strengthening before Week 6. See Fig. 7.

Timeframes for commencing strengthening Exercises.
Figure 8 presents the specific muscles targeted when strengthening. The three most common muscles strengthened are the 1st dorsal interosseous muscle (n = 18), opponens pollicis (n = 17) and abductor pollicis brevis (n = 16). Results were evenly divided on strengthening of the adductor pollicis muscle where 50% (n = 14) state they strengthen this muscle and 50% (n = 14) state they do not.

Specific muscles targeted when strengthening.
Protocols for post-operative management were developed by a therapist in conjunction with a surgeon by 72% (n = 13) of respondents (n = 18). Twenty-two percent (n = 4) used a protocol provided by the therapist only and 6% (n = 1) used a protocol provided by the referring surgeon only. The single main factor that influences the treatment protocol used was the therapists own clinical experience 50% (n = 9), the general practice where respondents work 22% (n = 4), evidence in a scientific journal 11% (n = 2) and surgeon’s preference 11% (n = 2).
All therapists (n = 19) indicated that pain is an issue in the rehabilitation of this patient group. The majority 63% (n = 12) advise patients that it can last up to 6 months following surgery. Thirty-seven percent (n = 7) advise that pain can last 6 to 12 months post-surgery.
Results of the surgeon’s survey identified that Trapeziectomy with LRTI was the most common procedure chosen. These results are similar to a practice survey of European surgeons [5] and American surgeons [11–13].
The stage of arthritis or functional level of the patient was not identified as a key factor when considering which procedure to perform. It had been anticipated that there would be a variation in procedure related to activity levels and radiographic staging. Limited respondents indicated the reasons for choosing this procedure. The main reasons cited were ‘reliability’ and ‘familiarity’. An American study in 2018 found that over 50% of respondents chose a particular procedure based on ‘personal clinical experience’ over ‘current evidence’ or ‘training’ [13].
Previous studies have recommended that hyperextension should be addressed surgically [20] to prevent abnormal load on the CMC arthroplasty which can lead to subsidence of the thumb ray [21] and reduced pinch strength and function [22]. A recent study found that more than 20 degrees of MCP hyperextension following trapeziectomy with ligament reconstruction had negative effects on functional outcomes [21]. The majority of respondents perform an additional procedure which reflects recommendations in the literature.
Most respondents (67%) perform an additional procedure if stage IV arthritis is present which is higher than the findings of a previous study [12]. The majority of the respondents did not outline what additional procedures they would complete. Of those who did, four would perform an arthroplasty of the STT joint while two surgeons specified that they would resect the proximal trapezoid. Excision of the proximal 2 mm of the trapezoid with excision of the trapezium has been advocated for in the literature for co-existing STT OA [23].
There was a high referral rate to hand therapy which reflects the results of a previous study [13].
There was some consensus in terms of the findings of the therapists’ survey in relation to splinting and casting. All patients are casted in the post-op period and most for just 1-2 weeks. A rigid long thumb spica and neoprene splint are most commonly used. There is some consensus in terms of time frames for commencing splints. Most commence a rigid long thumb spica at week 2 and a neoprene splint at, or after, week 6. A systematic review in 2014 found huge variability in the length and type of post-operative immobilisation and as a result could not make recommendations on best practice [16]. Another systematic review found that shorter immobilisation times of 4–6 weeks or less had positive effects on pain, grip strength and activity but that high quality studies are lacking [17]. The results of our study found that most cease full time rigid splinting later, at week 6. A recent randomized controlled trial found no difference in primary or secondary outcomes between a neoprene splint and early mobilisation at 3 weeks compared to a rigid splint and no exercises until weeks 6 [24]. The only difference was improved pain at rest at 12 months in the neoprene/early mobilization group. It appears that earlier commencement of a neoprene splint than what was found in our study is as safe and effective as more rigid immobilization [24].
There was a large variability in when movement is commenced for each procedure, and this is also reflected in the findings of other studies [18]. A systematic review in 2018 found that earlier mobilization at four weeks or less seems to have a positive effect on outcomes [17]. This was also found to be the case in a recent randomized controlled trial that found no adverse effects from commencing exercises and a neoprene splint from week 3 [24].
The earliest commencement of strengthening exercises is week 6 with most starting at week 6 and 8. These results are similar to a study by Siegel et al. [18].
The 3 most common muscles strengthened are the 1st dorsal intereosseous, the opponens pollicis and the abductor pollicis brevis. Strengthening these muscles has been advocated as part of a dynamic stability program [25, 26] for conservative management of CMC OA. A systematic review found that post-operative studies tend emphasise MCP flexion and CMC abduction/extension while CMC flexion, adduction and opposition are avoided [17]. Some studies mention thenar strengthening [24, 27] while others report pinch and grip strengthening without providing more detail [6, 15, 24, 28–31]. Respondents were evenly divided on whether adductor pollicis should be strengthened or not. There is evidence that adductor pollicis produces a deforming flexion/adduction force resulting in instability at the CMC joint and strengthening of this muscle has been advised against [26, 32, 33].
A strong collaboration is seen between therapists and surgeons regarding post-operative management. Therapists responded that post operative protocols are developed in consultation with the surgeon in most cases (72%). This is higher than reported in a survey of practice of American therapists where just 45.5% [18] develop protocols in conjunction with the surgeon. The single main factor that influences treatment protocol is the therapists own clinical experience. This may in part be because published studies provide little information on post-operative care and don’t adequately describe immobilisation and exercise protocols [17, 18].
There was consensus from therapists that pain is an issue following this surgery and can last anywhere from 6 to 12 months. In clinical practice this should be a factor to consider when selecting patients for surgical intervention. It is important to ensure that patients are educated about pain prior to surgery to set realistic patient expectations and help maximize post-operative recovery.
This study had a low response rate for both surveys. However, this is a small, specialised area of practice and the numbers are felt to be an accurate representation of surgeons and therapists treating this cohort in Ireland. Our research aim was to investigate surgical management only and therefore we did not include non-surgical interventions such as medication or injections that may be used in the earlier stages of the disease or with more sedentary patients.
In both surveys not all respondents completed every question. Open ended questions were used to capture clinical reasoning and rationale behind answers. As these were not completed by all respondents further research into why surgical and therapy practice decisions are made is warranted.
Conclusions
This is the first review of practice in Ireland investigating surgical and post operative management of trapeziometacarpal osteoarthritis. Trapeziectomy with LRTI is the procedure of choice and reflects current international practice. The stage of arthritis and functional level of the patient was not found to be an important factor for choosing this procedure.
A strong collaboration between surgeon and therapists is demonstrated by the high referral rate to therapy and the joint development of protocols. There is some consensus for post-operative casting and splinting but more variability in terms of exercise prescription. Pain is a factor to consider post-operatively and should be included in patient education prior to undertaking this procedure. The length of time that pain lasts following surgery also warrants further research.
Footnotes
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
Ethical approval was obtained from Trinity College Dublin Ethics Committee (project number # 20200214).