
Abstract
Introduction
Trapeziometacarpal osteoarthritis (TMC OA) is a common condition frequently related to instability and hypermobility. Many factors are involved in the development of this degenerative process. Recent research suggests that the position of the metacarpophalangeal (MCP) joint may influence TMC joint contact wear patterns and subsequent development of OA. The aim of this study is to explore the alignment of the MCP joint of the thumb during lateral pinch in order to describe the naturally occurring alignment in a group of healthy volunteers without symptoms.
Methods
One hundred and nine participants were asked to apply a lateral pinch manoeuvre to a pinchmeter, while their thumbs were assessed. Passive hypermobility of the thumb MCP (MCP) joint was assessed, key pinch strength was measured, key pinch position was photographed and the angle of the joints during the assessment was measured.
Results
Four different functional pinch patterns were identified. The most frequent pattern seems to be MCP hyperextension described by Moulton as harmful for the TMC joint. The level of strength obtained did not correspond to the pinch pattern used, and hypermobility of the thumb MCP joint did not determine the position of the thumb during key pinch.
Conclusion
Four different thumb postures were identified during lateral pinch; however, these postures were not associated with any difference in pinch strength. We conclude that the more unstable and mechanically inefficient postures are compensated by functional capacity.
Introduction
The thumb accounts for 70% of hand function. 1 Among pinch patterns performed by the thumb, lateral pinch is one of the most important movements: it starts from a flexion and adduction movement of trapeziometacarpal (TMC) joint, followed by flexion of the metacarpopha-langeal joint (MCP) and interphalangeal joint (IP) bringing the column of the thumb closer to index the finger.1,2 This position allows the thumb to exert pressure between the pulp of the thumb and the lateral side of the index finger, which can generate strength and stability, 2 as its Latin name Pollex suggests (strength, efficiency).
The strength used during functional tasks depends on the weight of the object to be held, and also on its size, shape and material. 3 The smaller and smoother the object, the more strength is required to stabilize it. In a study of the forces affecting the TMC joint, Cooney and Chao 1 concluded that for each kilogram of force exerted by the thumb against the fingertip, 12 kg of compressive force was applied to the TMC joint. If we take into account that normal pinch forces can reach 10 kg at the tip of the thumb, then it can be extrapolated that there would be 120 kg of compressive force at this joint. 1 To support this strength, great stability is needed.
Testing grip and pinch strength in hand rehabilitation provides important data in order to evaluate the effectiveness of therapy by comparing strength functional results over time and comparing these results with established normative data. The position for testing this force had been established by Mathiowetz in order to be able to compare the strength results for all patients pinching in the same way. However, we have observed clinically that not all patients are able to pinch in the same wrist and thumb position.
Ideally, the most biomechanically advantageous position to perform the pinch is the arched position,1,4,5 such that there is flexion, in the sagittal plane of both the IP and the MCP joint, while the first metacarpal is in extension on the trapezium. This position is when there is maximum articular contact, ligaments are relaxed and muscles have a central position and are therefore more efficient. 6 That TMC position is called the neutral position.7–16 In this position, muscles are able to follow the central excursion and are more efficient.
Hand osteoarthritis (OA) has been related to the intensity of the strength required for prehension and to the repetition of harmful gestures. For this reason, the development of pathology in the thumb is quite common. TMC joint OA is highly prevalent in the population.17–19 It generally affects more women than men over 45 years of age in a proportion of 3 to 1.17,18 Of the people affected by TMC OA, 33% 17 had symptomatology characterized by pain in the base of the thumb and loss of strength, which can be aggravated by manipulative activities such as unscrewing a jar, turning a key to open a door or holding a book. This pain imposes substantial restrictions on everyday functioning. One of the main research fields that have aimed to elucidate the aetiology of TMC OA is the study of wear patterns of the TMC joint.12, 20–23 By means of different methodologies, the sites with the highest level of articular wear patterns have been identified, as well as their links with the stabilizing elements of the TMC joint.22, 24–27 Wear and tear is present in the volar ulnar12, 20–25, 27 and dorsoradial12, 20, 21 aspects. While the anterior area of wear and tear is the area that carries the highest load due to excessive flexion–adduction, the dorsoradial area is subject to wear and tear due to shear movements associated with dorsoradial subluxation during prehension movements.12, 21
When conducting studies of articular wear patterns, some authors used lateral pinch as a study position, with the thumb in the arched position.5, 20, 23 Other authors suggest that if the TMC flexes too much while performing lateral pinch, a hyperextension of the MCP28–31 will be caused. Anatomically, this connection is logical, as the TMC and MCP joints may be conceived as a functional unity.28, 32
In 2001, Moulton et al. 29 demonstrated that, in the process of performing a key pinch, merely positioning the MCP joint in extension at 0° or in hyperextension at 30° changed the pressure pattern at the TMC joint. The more hyperextended the MCP, the greater the pressure on the anterior and ulnar area. So the pressure in relation to the position of the MCP increases in the areas with most erosion. Until then, hyperextension had been considered a secondary phenomenon to the closure of the first web space.1, 4, 28, 30, 33–38 Moulton et al. 29 raised the possibility that the position of hyperextension of the MCP could contribute not only as a secondary factor, but also as a primary factor in the pathological chain of degeneration of the TMC thumb joint.
Wajon (2003) also identified an association between the alignment of the interphalangeal (IP) and metacarpophalangeal (MCP) thumb joints of physical therapists performing posterior-anterior manipulation techniques, and the presence of pain. 39 She observed that young therapists had more pain in the MCP joint and that this pain progressively moves to the TMC joint in older physical therapists.
Hypermobility of the TMC joint has been associated with various predisposing factors, including joint incongruence,40, 41 geometry and bone shape,10, 13, 42, 43 ligament instability24, 25, 40, 41, 43–50 and the function of some muscles.40, 41, 51 However, all these concepts refer to mechanical stability, not functional stability. 15
Ligaments play an important role in stability, not only as a mechanism for restricting movement but also as a sensory system for the joint. 52 To better understand their function, it is important to point out that these ligaments tighten in extreme positions. When this tension appears, the ligaments inform the central nervous system (CNS), which reacts with a protection reflex, activating the muscles to stabilize the ligament through feedback. 53 These concepts have been clearly demonstrated in the wrist joint but not yet in the thumb. On the other hand, if these ligaments are kept in continuous tension, mechanoreceptors can adapt and stop their information being passed to the CNS. Without the protection of muscles they can be weakened and they will therefore lose their mechanical efficiency and also their capacity to activate a protection reflex. 54 If these ligaments are weak, this system can be functionally affected as a part of the reflex protection system of the joint, with a loss of natural protection capacity.52, 53, 55
Thumb muscular stability is not a new concept,21, 56 as numerous authors have already mentioned the importance of doing exercises for muscular strength and muscular stability.33, 57–60 However, some controversy exists around this concept.
Undoubtedly, the most mentioned muscle is the abductor pollicis longus (APL). It has been considered as a ‘harmful’ muscle for TMC OA mainly because of its capacity to subluxate the first metacarpal while working with the adductor pollicis (AP) muscle. Studies demonstrate that there are no relationships between APL anatomical variations and OA of the thumb. Other authors consider the APL as the only muscle capable of keeping TMC extension-abduction and it would be then the first to open the web space.14, 26, 32, 61–67 This muscle works together with the adductor muscle, which is the one that flexes the metacarpal and then closes the web space.28, 33, 51, 68 If this muscle shortens and closes the first intermetacarpal space, the APL will remain constantly stretched and will lose its strength and work capacity28, 51 or will remain inhibited, which means a loss of the arched position of the thumb. 32 In that case, there will be an automatic need to hyperextend the MCP in order to achieve gestural efficiency.28–31
On the other hand, the muscles with the capacity to reduce subluxation and joint compression are the first dorsal interosseous (1stDIO) and opponens muscle. The importance of first 1stDIO is not new, it had already been pointed out by Brand 32 who described it as the thumb's holding muscle. In 2000, Boutan 7 stated that when this muscle is working with the thumb opponents, it can reduce the base of the thumb through dorsoradial subluxation. This theory has been supported by Mobargha et al., 69 and also, more recently, by Albrecht. 70 The other muscles would have a more functional role involved with mobility.
In our professional practice as lecturers, we were able to observe hundreds of physical therapy students using their thumbs every year. We observed different positions for pinching, which did not always include the arched position. When researching this concept, we found that different thumb posture patterns are described for rheumatoid thumbs 71 but not for asymptomatic healthy people. If we take into account, firstly, that key pinch is a prehension mechanism that has been described as a trigger factor for TMC instability and OA, and, secondly, Moulton et al.'s 29 and Wajon and Ada's 39 observations, we hypothesized that the observation of key pinch in healthy volunteers can give us further information and help us understand the injury mechanisms leading to the instability and degeneration of the base of the thumb.
The aims of our study were:
To determine the functional patterns of key pinch in the population with no specific thumb pathology; To determine whether those patterns can have an effect on key pinch strength; To determine whether passive articular hypermobility of the MCP joint is a decisive factor in establishing key pinch patterns.
Methods
This observational study was conducted on physiotherapy students. The group consisted of 109 students, 29 males (26.6%) and 80 females (73.4%). Their average age was 20.89 years (ranging from 19 to 26). The majority (87.2%) were right-handed. Ethical approval was not required as it did not involve any intervention or any risk for the participants. All participants gave their informed consent and all data obtained remained anonymous, in accordance with the Helsinki Declaration.
Inclusion criteria were young physiotherapy students who had not suffered any kind of mechanical, functional or traumatic damage. Participants were excluded if they had spent more than 4 years in a specific job (in case this might have made changes to their natural pinch alignment), if they failed to provide adequate demographic data or if they had some history of hand pathology.
In order to assess the natural alignment of the thumb during key pinch photographs were taken of the participants while performing key pinch and in such a way that goniometric measurements of the angles of the first meta-carpal/wrist joint, MCP joint and IP joint in the sagittal plane could also be taken. Thumb strength was measured while the pictures were taken, and, finally, passive hyper-extension of the MCP joint was also measured.
During the key pinch test, all participants were asked to exert pressure three times, as strongly as they could, and their strength was recorded in all the attempts. In the first attempt, we made sure the participant understood our instructions. A sagittal image of the thumb was taken during the second attempt.
In order that each participant could use a natural, spontaneous posture when applying maximum pinch, we used the method described by Mathiowetz et al. 72 with three modifications. In Mathiowetz's method, subjects sit with their elbow at 90° – neutral prono-supination. Our modifications to this method were: firstly, their wrists were in contact with a piece of foam placed on the ulnar side of the hand, but at no time resting on it. Secondly, they had to have their wrists free instead of being extended between 0° and 30°; and, thirdly, they were asked to hold the pinch gauge while applying pinch force. The reason why we decided to add these three modifications was because we wanted subjects to find their most comfortable and efficient pinch position by themselves.
In order to get images that could be easily compared with each other, a wooden and plastic support was designed for the pictures. The IP and MCP joint angles were measured in the sagittal plane, taking into account the following marked lines (Figure 1):
Assessment posture Along the P2 line: the line drawn between the base of the fingernail and the IP joint; Along the P1 line: the dorsum of the first phalanx; Along the metacarpal: a line running dorsally over the metacarpal from the MCP joint to the dorsal wrist crease; Along the forearm: the dorsum of the radius.
Statistical analysis included univariate descriptive analyses and bivariate analyses, chi-squared for categorical variables and t-test for continuous variables. Data were entered in MS Excel® software (Redmond, USA) and analyzed with IBM SPSS® (IBM, Chicago, IL, USA). 15 A related t-test was used because data distributions were approximately normal.
Results
Pinch patterns
By analysing the images of the alignment of the MCP joint during key pinch in the sagittal plane, we detected four postural patterns:
Pattern 1: Intrinsic pattern which represents 6.35%. The MCP joint is flexed during the pinch but the IP joint extended at 0° or in hyperextension. The TMC joint is slightly extended with respect to the horizontal line defined by the radius (Figure 2). We called this the ‘intrinsic pattern’, because in this position the contribution of flexor pollicis longus (FPL) was apparently not as important as flexor pollicis brevis (FPB) or AP.
Intrinsic pattern
Pattern 2: Mixed or arched pattern which represents 31.2%. The MCP joint is flexed more than 5° during the pinch and the IP joint is flexed. The TMC joint is consequently extended (Figure 3). We called this the ‘mixed or arched pattern’, because the APL, FPL and FPB and AP were apparently all working at the same time. (In this case, we should take into account that many people do not have such great flexion of the MCP joint, so they cannot achieve this position).
Arched pattern
Pattern 3: Extrinsic pattern which represents 24.3%. The IP joint of the thumb is greater than 60°. The MCP joint is between −5° and +5° from flexo-extension (Figure 4). We called this the ‘extrinsic pattern’, because in this position the FPL is the predominant muscle applying the pinching force.
Extrinsic pattern
Pattern 4: Hyperextended pattern which represents 36.9%. The MCP joint is hyperextended more than 5° and the IP joint is flexed. The TMC joint is close to the horizontal line, and, in some cases, flexed (Figure 5). We called this the ‘hyperextended pattern’, because in this position there is no control of the MCP flexion position.
Hyperextended pattern
Distribution of thumbs according to pinch pattern and sex and hand dominance
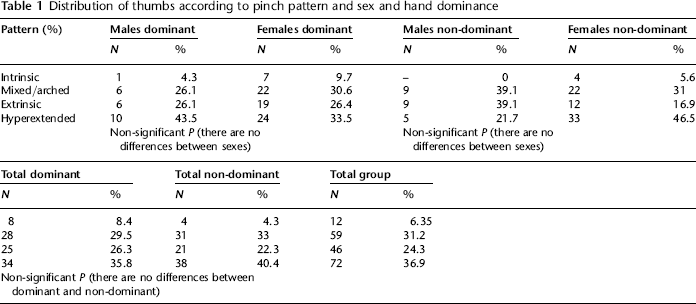
Of all subjects in the study, 46.8% had a symmetrical pinch pattern, whereas 53.2% had an asymmetrical pattern (Figures 6 and 7).
Asymmetrical patterns of the same subject Asymmetrical patterns of the same subject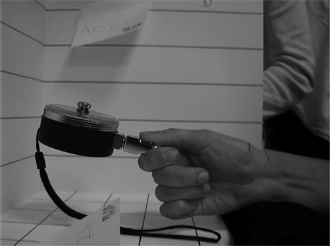

Strength
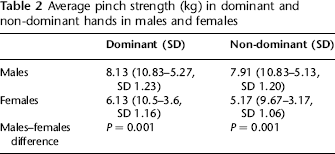
Average pinch strength (kg) in dominant and non-dominant hands in males and females
Pattern distribution of pinch strength in dominant and non-dominant hands in males and females (kg range and SD)
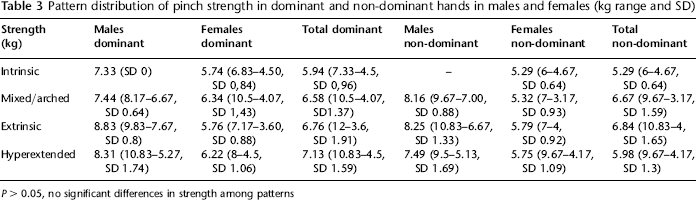
P > 0.05, no significant differences in strength among patterns
Hypermobility
Pattern distribution in those with hyperextension over 30° (43 thumbs, 22.75% of all thumbs evaluated), divided into those with unilateral hyperextension and those with bilateral hyperextension in the dominant and non-dominant hand
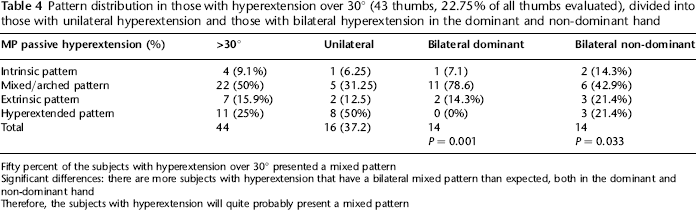
In order to know if there were any differences between the hypermobile group and the total group (hypermobile + non-hypermobile group), we compared the percentage of the different pinch patterns between the constitutional or acquired group and the total group.
Fifty percent of the subjects with hyperextension over 30° presented a mixed pattern
Significant differences: there are more subjects with hyperextension that have a bilateral mixed pattern than expected, both in the dominant and non-dominant hand
Therefore, the subjects with hyperextension will quite probably present a mixed pattern
We considered those subjects with a MCP joint with passive extension over 30° to be hypermobile. Those with bilateral hyperextension were considered to have a constitutional type of hyperextension, whereas those with unilateral hyperextension were considered to have an acquired type of hyperextension.
In the constitutional group, with passive bilateral hyperextension (Figure 8), we observed that, in key pinch, most of the subjects could obtain a stable arched pinch (Figure 9). The difference was significant (P = 0.001) in the dominant hand since, out of 14 subjects, none of them showed a hyperextended pattern and 11 showed a mixed pattern. For the non-dominant hand, a mixed pattern was present in six thumbs (42.9% versus 31.2% in the total group). The hyperextended pattern was present in three thumbs (21.4% versus 36.9% in the total group). These differences were not statistically significant but the results suggest that the constitutional hypermobile thumb (Figure 8) was able to compensate the passive hypermobility of the MCP joint with muscular control (Figure 9 and Table 4).
Thumb MP joint passive hyperextension Completely stable arched key pinch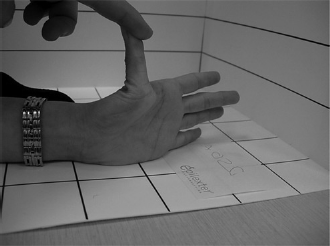

In the acquired group with unilateral hyperextension of the MCP joint greater than 30°, 8/16 subjects presented a hyperextended terminalateral pinch pattern (36.9% total group) in the hand with a greater MCP hyperextension. These data were again non-significant, although it seem to suggest that unilateral passive MCP hyperextension is associated with a hyperextended pinch pattern (Table 4).
Discussion
We expected to find different thumb patterns and suspected that the least favourable and the least aligned patterns would be the least efficient, causing ligament deformity to the MCP joint, especially towards hyperextension, as this was what we had previously observed clinically.
Regarding the first goal of our study, we were able to identify four different patterns of MP and IP joint alignment in the sagittal plane during lateral pinch which are different from those described by Nalebuff. 71
The intrinsic pattern shows a strategy to perform a different type of pinch. The excessive flexion of the first phalanx given the contraction of the intrinsic muscles prevents the TMC from increasing its flexion. However, this involves the pulp of the thumb remaining far from the side of the index, which requires IP hyperextension.
The arched pattern described in the literature1, 5, 25, 73 as an ideal pattern accounts for 31.2% of all cases, and is not the most common. The presence of both extrinsic and hyperextended patterns confirms Moulton's observation in the laboratory. Both patterns suggest a gradual loss of motor control of the thumb with a progressive collapse of the TMC towards the flexion and the MCP towards hyperextension (except in people who cannot flex the MCP and are consequently not capable of achieving the arched pattern mechanically).
Hyperextension of the MCP joint during key pinch involves increased flexion of the TMC joint. The demand on the TMC ligaments in this position may make them gradually weaker and reduce their capacity to restrict joint subluxation.1, 74–76 As a result, the joint progressively becomes more unstable, which facilitates dorsoradial subluxation and leaves the joint surface into a type of distribution that encourages wear and tear.
Regarding the second goal of our study, we did not observe any significant differences in the strength obtained during the different pinch patterns. It is therefore proposed that, when there is no established pathology, and regardless of the pattern used to form the key pinch, the efficacy in the strength of the gesture will be the same. According to Moulton et al., 29 the use of an unfavourable pattern will be associated with greater compression occurring on the wear-and-tear areas. Any person trying to pinch something during the performance of key pinch, gathers the anatomical elements available to obtain a strong and stable lateral grip. Harmful postures during key pinch are not avoided by the patient because the priority is functional efficacy. The imbalances that may arise during pinching do not generate any symptoms, the imbalances are not corrected and they can therefore end up generating deformities of anatomical elements.
The third goal of our study was to establish a connection between hypermobility and the patterns considered harmful. Participants who had an asymmetric hyperextension and who considered to have acquired hypermobility had a greater percentage of unstable pinch than the total group (50% versus 36.9%). However, an unforeseen but very interesting aspect was that hypermobility, represented by the participants in the study who had a constitutional hyperextension of the MCP joint (>30°), produced a stable arched key pinch more easily than those subjects who had an acquired hyperextension. Apparently, those patients had better motor control of their thumb during lateral pinch, and, consequently, hypermobility was not connected to an unstable pinch.
There are limitations to this study. The sampling of participants was due to ease of access to the study population but may not be representative. The exclusion of those who have worked in the same professional activity for more than four years was a subjective decision considering that the aim was to avoid external factors that could have deformed the thumb. We considered that work of seven hours a day could be one of the factors that might have the greatest effect on this aspect.
Taking into account that goniometric measurements can generate errors of ±5°, we considered this margin in all the measurements. All measurements were taken by the same assessor.
We think the ideal measurements would be made in three-dimension. For this reason, we also took pictures of the thumb in the frontal plane to evaluate possible modifications in this plane. However, when it came to making the measurements, we could not distinguish between degrees of rotation, abduction and adduction. This is why these data were excluded from the study.
Clinical implications
This study contributes towards an understanding of thumb muscle imbalance as one of the factors that could generate thumb instability and finally TMC OA. At present, splinting is the only hand therapy intervention showing evidence of its effectiveness to improve the symptomatology of pain,30, 36,77–81 and function33, 39, 58, 78, 82–84 for TMC OA. This effect is very plausible, as a splint stabilizes the base of the thumb. Although it is true that stabilization with a splint can reduce the symptoms, immobilization will also increase stiffness, 85 weaken voluntary contraction, reduce tone, contribute to muscle wasting86–89 and induce cortical reorganization 90 As a result, the possibility of regaining muscular stabilization may be reduced.86, 88, 89
Therefore, splints should be applied as temporary elements while appropriate muscular training is taken up once again. Exercises are often included in the conservative treatment for TMC OA.41, 57–60 The exercises specifically designed to treat this pathology are dynamically oriented, to regain motion, with counter-resistance and concentric work aimed at improving strength.4, 14, 33, 58, 91
For future research on treatment for thumb instability, and therefore TMC OA, an interesting approach would be to focus more on motor control and proprioception15, 16, 73, 92–95 of the thumb in a neutral or arched position rather than working only with thumb mobility or muscle strength.
As only 33% 17 of the people with radiological TMC OA report pain, exercise should be considered not only for patients who find themselves at an early stage of TMC OA, but also for patients with an advanced stage of OA, as it means it may be possible to discover a non-symptomatic point of balance, even if there is structural deformity.
In the same way, this kind of rehabilitation could be considered before and after surgery, because the improvement in mechanical stability does not guarantee functional stability and may make surgery fail.29, 31, 37, 38
More electromyography studies should be carried out in order to provide extra information about the role of each muscle in the different patterns and more clinical studies should be developed to find out the best way to improve the motor control of the thumb.
Footnotes
Acknowledgements
The authors wish to express their gratitude to Anne Wajon, who offered invaluable assistance and support in the writing of this paper.