
Abstract
BACKGROUND:
Understanding how dynamic arm supports affect the ability to perform activities of daily living (ADL) in daily life situations is essential for improved prescription.
OBJECTIVE:
To determine whether the newly developed MMAAS is a useful tool to assess the RoM at home. Secondly, to investigate differences in RoM and ADL performance with and without dynamic arm support.
METHODS:
Five dynamic arm support users performed nine activities with and without dynamic arm support at home. A reference group of five participants was included. Shoulder and elbow RoM were assessed for the three most difficult tasks.
RESULTS:
The measurement of the elbow joint RoM appeared unreliable. In most participants shoulder RoM increased with dynamic arm support, but the magnitude of change differed. Variation was also found regarding whether people could perform ADL with and without support.
CONCLUSIONS:
In its current state the MMAAS is not regarded a useful tool for assessing the RoM in the domestic setting. The ability to perform ADL and RoM seem influenced by the environment, users’ needs and abilities. Future studies investigating effects and benefits of dynamic arm supports should be conducted in a broader daily life context.
Keywords
rm
Abbreviations
Activities of Daily Living (ADL),
Range of Motion (RoM),
Inertial Measuring Units (IMU),
Motion and Muscle Ambulatory Activity System
(MMAAS),
Individually Prioritized Problem Assessment
(IPPA).
Introduction
Upper extremity impairments can result in a limited ability to perform activities of daily living (ADL) such as eating, or using a computer [1, 2], and can result in an increased need for assistance [3]. Boys diagnosed with Duchenne muscular dystrophy show a decreased ability to perform ADL as the disease progresses and upper extremity function declines [2]. Of all persons affected by a stroke about 48% has to cope with the consequences of upper extremity impairments [4]. These are just two examples of the many disorders that result in some degree of upper extremity impairment [5].
During the course of a disease or impairment people may receive physical therapy or training programs to restore upper extremity function or to prevent further deterioration of the arm’s function [2, 6]. Despite functional improvements, the arm function is often still not optimal and as a consequence people may still be unable to perform essential ADL [2, 7]. To compensate for this remaining loss of function, and to improve independence, assistive technology can be recommended. Dynamic arm supports are a class of assistive technology specifically designed to support the weak upper extremity. Several types of dynamic arm supports are commercially available, ranging from non-actuated, to passively-actuated, to actively-actuated devices [8, 9, 10, 11]. In The Netherlands a specific device is selected by an end-user in close cooperation with a supplier and/or an occupational therapist.
A literature review was conducted to gain insight into the effects and effectiveness of these devices [12]. Most studies reported positive effects at the level of body functions. Effects were for example found on tremor reduction, speed of movement [13], and joint Range of Motion (RoM) [8, 14]. These studies were conducted under controlled circumstances in laboratories, but the benefit of these devices in daily life situations were not in all cases evident and a relatively high level of non-use was found on the longer term [12]. Increased knowledge regarding the effects and benefits of dynamic arm support in daily life is essential to support the prescription of these devices. This knowledge could also support future developments. Therefore it is necessary to study how dynamic arm supports affect the ability to perform ADL in daily life situations. One way in which these devices seem to affect this ability is by altering the achieved RoM [14], because in order to allow users to perform ADL again, dynamic arm supports have to support those movements that are necessary for a specific task.
For different tasks, a different RoM of the shoulder and the elbow is required. Combing hair for example requires a smaller shoulder flexion RoM compared to placing a can on an overhead shelf [15]. Haumont and colleagues studied upper extremity RoM with and without a dynamic arm support (WREX ©, JAECO Orthopedic Hot Springs, USA). They found that the shoulder and elbow RoM increased while participants used the WREX [14]. Ideally, dynamic arm supports alter the RoM of the weakened upper extremity towards the RoM that people without impairments use to perform ADL.
Haumont and colleagues studied the RoM in a laboratory setting [14]. However, dynamic arm supports are designed to be used at home where people probably show more variation in task execution compared to a controlled setting, for example due to adaptations in houses of dynamic arm support users. In order to gain insight into whether ADL can be performed with a dynamic arm support and how upper extremity movements are supported, it is essential to assess this in the domestic setting. Additionally, in rehabilitation in general the focus has shifted from gains and effects in body functions to effects on an activity and participation level as defined in the International Classification of Functioning, Disability and Health [16]. This stresses the relevance of assessing effects of dynamic arm supports in daily life situations rather than measuring effects under controlled conditions in a laboratory, to which this study aims to contribute.
Systems comprising multiple inertial measuring units (IMU) provide a portable upper extremity motion capturing instrument that can be used for recording motion in the domestic setting [17]. A system specifically designed for people with muscle weakness and coordination problems is the MMAAS. MMAAS stands for Motion and Muscle Ambulatory Activity System. The system comprises a stretchable cardigan with a data acquisition system and sensors [18]. The system allows for real-time and wireless upper limb movements and EMG measurement. Reliability and validity of the MMAAS were confirmed in a laboratory setting [19, 20]. Applicability of the MMAAS in the domestic setting had not been assessed before.
Therefore the objectives of this pilot study are twofold: 1) to ascertain to what extent the RoM can be assessed during ADL in the domestic setting using the MMAAS; 2) to determine differences in the ability to perform ADL and RoM when people do or do not use their dynamic arm support.
Methods
In order to achieve the objectives the study involved three steps. First, the ability to perform activities of daily living was assessed. Secondly, for the tasks that appeared to be the most difficult the shoulder and elbow RoM was assessed. Finally, the extent to which the RoM could be assessed using the MMAAS in the domestic setting was evaluated. The study involved dynamic arm support users and a reference group of people without upper extremity limitations. The study was approved by the Medical Ethical Committee Atrium-Orbis-Zuyd (13-N-53).
Dynamic arm support users were recruited via a manufacturer and supplier of dynamic arm supports (Focal Meditech, Tilburg, The Netherlands). Participants were selected on the basis of convenience sampling. Inclusion criteria were: people did use their arm support in the past week, participants were eighteen years or older and were cognitively able to participate. People were excluded if they were not able to sit upright without support in a (wheel)chair, if they used supportive devices for the upper extremity other than an arm support; or if they had a health condition preventing movements of the arms other than the reason for using the arm support, and if they did not speak Dutch. Participants either used the Sling or the Top/Help electric [21, 22]. These dynamic arm supports are two devices commonly used in the Netherlands. Both devices are developed, manufactured and supplied by Focal Meditech (Tilburg, The Netherlands). The Sling is a suspension type, passive dynamic arm support in which counterweights negate the effects of gravity and the Top/Help electric is an active device that functions as an arm lift that actively supports vertical arm movements. In addition, five persons (who were 18 years or above) without upper extremity limitations were recruited for reference purposes.
Participant characteristics
Participant characteristics
Participants are referred to in the text as
Picture of the MMAAS. Numbers 0 to 4 denote the recommended position of the sensors. Sensor number 1 is positioned on the back.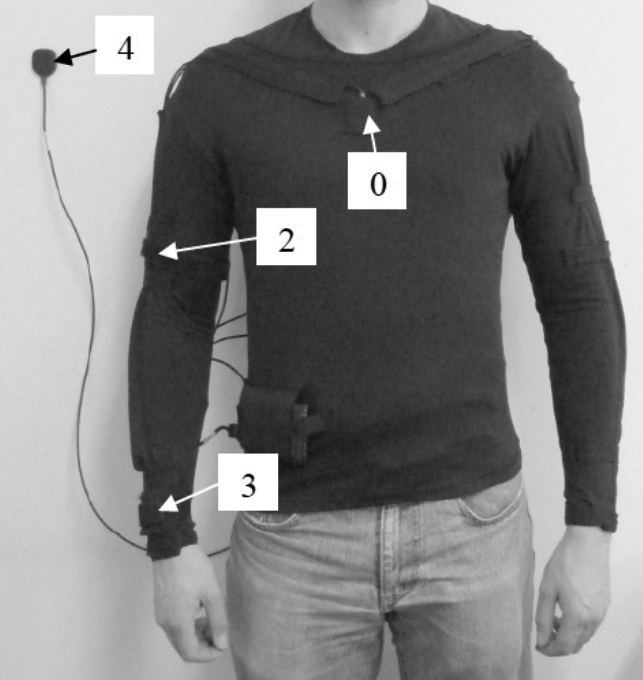
To capture upper extremity movements, the MMAAS
motion capturing instrument (Fig. 1) was used (Maastricht
The study was performed at the participants’ homes. The arm function of dynamic arm support users was assessed with the Brooke scale [24]. Nine ADL tasks were selected to perform. These tasks are crucial for independent living [25], are regarded as important by potential users [26, 27], and cover a wide RoM [28]. The ability to perform each task and representing arm movements were recorded for the following ADL:
Touching the ipsilateral ear; represents using a telephone Eating with a spoon Drinking from a glass Touching the opposite axilla; represents washing the armpit Touching the seat between the upper legs; represents retrieving a dropped object Combing hair Stroking a pet Grabbing a door handle Grabbing a book from the shelf
Participants were instructed (or helped) to put on the MMAAS cardigan and told to sit on the chair. To calibrate the MMAAS, participants had to keep their shoulder flexed (90
Range of motion with and without dynamic arm support in dynamic arm support users
Without
Range of Motion in degrees of people without upper extremity limitations (reference group)
M
Changes in RoM are expected to be most apparent in challenging tasks as it is expected that in difficult tasks support is needed the most. Therefore, the three tasks that could not be performed without dynamic arm support, and with dynamic arm support, by the highest number of participants were selected.
The RoM was determined for the 1) elbow flexion, 2) pronation/supination, 3) shoulder rotation, 4) shoulder forward flexion/extension, and 5) shoulder abduction. This was done for the performance with and without device and for the people without impairments. Joint angles were calculated within the MMAAS software. The RoM was obtained by calculating the difference between the minimal and the maximal joint angle achieved during the task.
Data of specific joint movements were excluded if the sensors shifted during the measurements, if the calculated RoM exceeded the anatomical RoM [29], and if plotted joint angles showed a movement pattern that was not fluent. In order to determine the latter, movements (based on joint angles) were plotted.
The RoM was individually compared between tasks performed with and without dynamic support. This was done for each task and each movement separately.
Results
From the eleven invited users six people wanted to participate. One of those could not participate because the dynamic arm support was broken at the time. Characteristics of the remaining five dynamic arm support users who participated are listed in Table 1. In the reference group two males and three females without upper extremity impairments were included (age range: 21–59, average age: 37.2).
Task performance. The numbers in the bars represent the tasks listed. Participants are referred to in the text as P.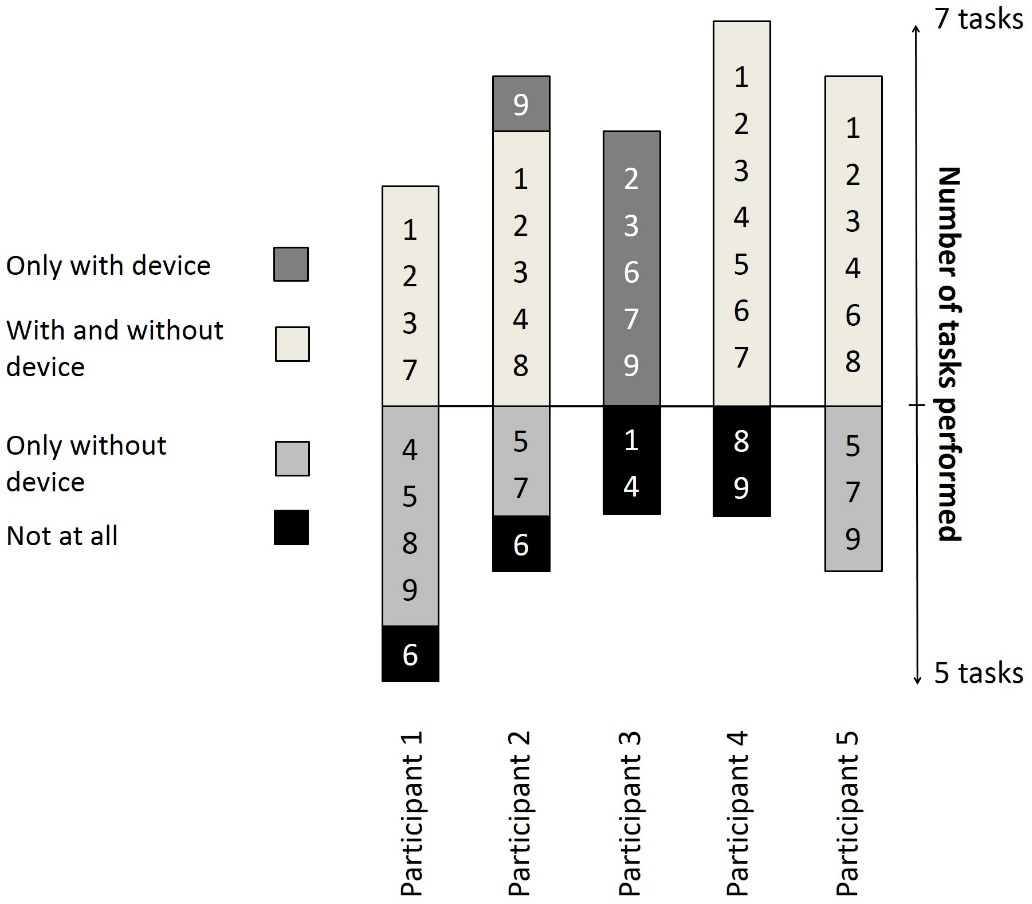
Dynamic arm support users were asked to perform activities with and without their dynamic arm support. Two participants (P 2 and 3) were able to perform activities with their dynamic arm support they otherwise (without device) could not perform (Fig. 2). The other participants could not perform more activities with dynamic arm support than without (P 1, 4 and 5); they could perform most activities also without dynamic arm support. Three participants were not able to perform tasks with dynamic arm support they could perform without.
The tasks ‘grabbing a book from the shelf’, ‘combing hair’, and ‘touching the seat between the upper leg’ could not be performed with arm support by the highest number of participants. Therefore, the RoM was determined for those three tasks.
Upper extremity range of motion
The MAASS did not fit two persons, the cardigan was too small. To correct for this, the MMAAS sensors were placed at the desired anatomical location [23] on the skin with tape. Participant 3 did not perform task 5 as this was impossible due to the wheelchair construction.
A total of 24 elbow and pronation/supination movements had to be excluded, due to shifting sensors (12 movements), movements exceeding the anatomical RoM (6 movements), and movements that were not fluent (6 movements). All shoulder movements recorded were included (Tables 2 and 3).
Shoulder RoM (forward flexion/extension and abduction) was higher in most participants when they used their dynamic arm support (compared to without device), for the task combing hair and grabbing a book from the shelf (Table 2). However, in general the RoM achieved with support seemed to be lower than the RoM achieved by persons without limitations. The magnitude of change (with versus without support) differed widely between individuals; for example in combing hair, an increase in RoM between minus 5
It remains unclear whether the ability to perform tasks is associated with the achieved shoulder RoM. There were three activities that could only be performed with dynamic arm support (Fig. 2, P3 task 6 and 9, P2 task 9). In cases, an increase in RoM (towards the RoM of persons without limitations) resulted in persons being able to perform the activity. In other cases, the RoM of persons without limitations was achieved while participants were still unable to perform the task.
Elbow flexion RoM seemed to decrease when the dynamic arm support was used. However, it is important to note that results for elbow flexion are based on only two arm support users.
Discussion
The objectives of this pilot study were to 1) ascertain to what extent the RoM could be assessed during ADL in the domestic setting using the MMAAS and 2) to determine differences in the ability to perform ADL and RoM when people use or not use their dynamic arm support.
Applicability of the MMAAS in the domestic setting
The study revealed some unexpected difficulties of the MMAAS for the measurement in real life settings. Beforehand it was expected that the MMAAS was ready to be used in a field trial as it was designed for this purpose and its reliability and validity were confirmed in a laboratory setting. However, the MMAAS did not fit two of the five participants and sensors sometimes shifted when the arm moved in and out of the arm support. This means that the MMAAS currently cannot be used by people with deviating anthropometric data. More important maybe is the fact that a cardigan that does not suit properly can result in sensors that do not remain on the correct anatomical location which will threat the reliability of the measurements. For this reason no conclusions can be drawn about the effect of arm supports on the RoM for elbow joint and pronation/supination. In its current state the MMAAS is not regarded a useful tool for evaluating effects, specifically the RoM, of dynamic arm supports in the domestic setting. Before larger studies in daily life situations can be conducted with the MMAAS, and data can for example be used to support the development of new dynamic arm supports, it is essential that these issues are solved. However, the measurement of shoulder RoM appeared to be sufficiently reliable to draw some conclusions about what these results mean to the field of dynamic arms supports.
Differences in the ability to perform ADL and RoM when people use or not use their dynamic arm support
In tasks that involve reaching an increase in shoulder RoM (shoulder abduction, rotation and forward flexion) was observed. These tasks require lifting of the arm against gravity; supporting these movements matches with the design principles of these arm supports [10]. The increase in shoulder RoM found is also in accordance with the findings reported by Haumont and colleagues [14]. However, the magnitude of change differs widely among participants. This variation could be due to differences in the technology; using a Sling or Top/Help dynamic arm support, kinematic constraints of the arm supports, wheelchair construction, and the way in which the arm support is adjusted for example. Additionally, differences in effects can be due to individual differences in needs and abilities; some participants had a more severely decreased arm function which is reflected in the achieved RoM. Possibly also muscle contractures have affected the RoM [30]. Also the fact that activities were performed in the domestic setting has created variation in how activities were performed which affects the RoM. These individual differences indicate that, next to the arm support, many other factors affect the achievable RoM in daily life situations.
The relationship between whether tasks can be performed and the change in RoM as well as the RoM of persons without limitations remains unclear. Many participants were able to perform tasks although their RoM was lower than the RoM of people without limitations. One explanation could be the fact that participants have adaptations in their houses (for example lower shelves) which make it easier for them to perform tasks (with a smaller RoM). Additionally, participants were allowed to use compensatory movements. For example bending the head or back while combing hair might result in satisfactory performance with a smaller RoM. On the other hand there were participants who achieved similar RoM’s, compared to people without limitations, who were not able to complete tasks. It is not surprising, but apparently the RoM is not the only factor affecting the ability to perform tasks. This is in line with daily occupational therapy practice and its body of knowledge that acknowledges that the ability to perform ADL (occupational performance) may vary depending on the environment, and the use of assistive technology [31]. Additionally, persons who use arm supports may, next to a limited muscle strength, have to cope with for instance tremors, hand function problems, or coordination problems which could have affected the ability to complete tasks.
Findings of this study indicate that it is not easy to objectively determine the effects of dynamic arm supports in daily life situations. This is partly due to individual differences between users including their environment. This variation would be less present in studies conducted under controlled circumstances, however, dynamic arm supports are used in daily life situations by different users, in different contexts. So, in order to understand the real effects of dynamic arm supports it is essential to assess these effects in daily life and to take this variability into account.
Also the effect of the arm support on whether people were able to perform ADL differed widely between individuals. Only two participants were able to perform tasks with device they could not without. One of those participants had a severely impaired arm function (Brooke score 5), and also had the smallest RoM without support compared to all the other participants. This suggests that a person with a severely impaired arm function might benefit more from a dynamic arm support than persons whose arm function is less severely impaired. It was remarkable that most tasks could be performed with as well as without dynamic arm support. It seems as if the dynamic arm support does not support the ability to perform ADL in these cases. However, this study did not take into account the effort required to perform tasks, and the related ease, pain, fatigue, etcetera. Fatigue for example has been reported as a reason for using the arm support in daily life [32]. Additionally, despite the fact that the set of activities was chosen deliberately, possibly some participants use their arm support to perform other activities in daily life situations. From other studies investigating use of dynamic arm supports in daily life it is already know that devices are used for a wide range of ADL; from brushing teeth to eating and writing [9, 14]. For this study it is assumed that all participants functionally benefit from their arm support to some extent in daily life, because all people did use their arm support in the week prior to the measurements. They used it at least for eating and drinking, but the frequency of use varied.
The variation in the ability to perform ADL (with and without device) indicates that probably use in daily life and the functional benefit will vary between individuals as well. Which means that it is impossible to assess benefits in real life by measuring the ability to perform a standardized set of tasks and RoM alone. Scherer and colleagues already identified that individual differences in needs, preferences, technology characteristics, the environment, and many other factors influence assistive technology use in general [33]. This study suggests that factors related to the environment, a user’s abilities and needs and activities for which support is desired affect use and benefits of dynamic arm supports in daily life situations.
To support patients and professionals in the selection of dynamic arm supports it is therefore essential to understand which factors contribute to whether there is a functional benefit of a device or not. This information is currently lacking. Careful consideration of the factors that affect this benefit in the light of the available solutions might result in a more optimal match between the user and the dynamic arm support, which could favor the functional benefit perceived. And finally, this could decrease the relatively high level of non-use of dynamic arm supports [12].
Study limitations
This study had some limitations. Participants were recruited through one supplier (Focal Meditech) which might have introduced selection bias if they have chosen arm support users who were expected to have a large benefit of the device. This might have led to an overestimation of the RoM achieved with dynamic arm support.
The activities performed by the participants were not randomized. This would have affected the results if fatigue affected the ability to perform ADL and the RoM. However, participants only performed each movement twice and had to rest between tasks. Therefore this effect is expected to be negligible. Absolute joint angles were, especially for elbow movements and shoulder rotation, often (in 55% of the movements) higher than the anatomically possible RoM. This could be due to calibration errors or drift in the data. Data were excluded if the joint angles at the start and the end of a task were not equal. This precludes the possibility that drift in the data or calibration errors had an effect on the calculated joint RoM. Magnetic materials around the MMAAS sensors could have resulted in incorrectly measured data. It is known from de Vries and colleagues that variations in the magnetic field in lab settings are a thread to the validity of the data [34]. The magnetic fields in the domestic setting might be even more heterogeneous due to the presence of iron in walls, floors, and furniture etc. Despite the fact that the MMAAS corrects for this to some extent, the variation in magnetic fields likely have affected the data. In this study data were excluded if joint movements showed an influent pattern, which minimized the risk of including data affected by magnetic fields.
The RoM was assessed for three activities which were difficult to perform with currently available dynamic arm supports. However, this does not necessarily have to mean that the tasks for which the RoM was calculated are meaningful in daily life situations for all participants. This unfortunately is unknown. Besides, the individual differences in the RoM and the ability to perform activities between users suggests that measuring effects based on a standardized set of tasks is insufficient. The study would have benefited from an in-depth activity analysis, which would have provided more qualitative information regarding the facilitating and limiting factors, about how the activity performance changed and whether activities were regarded important by participants. Additionally, for future studies it is recommended to consider the use of an instrument that takes into account personal preferences and needs such as the the Individually Prioritized Problem Assessment (IPPA) [35].
Conclusion
The study revealed some unexpected difficulties of the MMAAS for the measurement in real life settings. In its current state the MMAAS is not regarded a useful tool for evaluating effects, specifically the RoM, of dynamic arm supports in the domestic setting. Before larger studies in daily life situations are conducted with the MMAAS it is essential that the reliability of the MMAAS in the field is improved. Additionally the cardigan should accommodate persons with different anthropometric data. Reliability of the shoulder joint RoM was regarded sufficient. Shoulder Range of Motion (forward flexion, abduction and rotation) increased with dynamic arm support. However, the magnitude of change differs widely among participants. Users also differ markedly in whether ADL can be performed with and without dynamic arm support. Aspects related to the environment, the user’s preferences, abilities and needs seem to influence the effects dynamic arm supports have in real life situations to a great extent. For future studies, in order to understand the real effects of these devices it is recommended to take this individual variation into account. Due to the highly individual character it is expected that also the functional benefit in daily life will differ between individuals. It is recommended that benefits are also assessed in a broader daily life context. Insight into benefits of dynamic arm supports and influencing factors could support the provision and the selection process of dynamic arm supports.
Footnotes
Acknowledgments
The authors would like to thank our colleague Gert Jan Gelderblom