
Abstract
BACKGROUND:
Clients with intellectual disabilities benefit from a fixed daily structure due to difficulties in remembering appointments and in performing daily activities.
OBJECTIVE:
To develop a memory application to structure and support daily activities for clients with intellectual disabilities that contribute to independence and to provide a clear insight into the developmental process of the application.
METHODS:
A ‘participatory design’ (two development cycles) was used to understand users’ needs, wishes, and abilities regarding structure and support of daily activities. Using a pre- and post-test design, two pilots (
RESULTS:
The pilots showed that the application has the potential to contribute to the independence of clients, e.g. less control needed regarding daily structure offered by formal carers. This was most evident in the last pilot because of the improved ease of use, the added value perceived by clients and formal carers and the increased focus on the implementation of the application in the care process.
CONCLUSIONS:
For successful integration of the memory application in the care process, well-defined personal goals of clients in the care plan are needed and carers should act according to these goals. Further research is necessary to examine the generalisation of findings.
rm
Introduction
In the Netherlands, the number of people with severe intellectual disabilities (IQ
The objective of this research and development process was to help clients with intellectual disabilities to structure and support daily activities with the assistance of a memory application. It was also initiated due to the increasing need for reliable and suitable applications for this vulnerable target group.
Background
Clients with intellectual disabilities have difficulties in processing information, e.g.organizing and understanding new and complex information, which hinders them in learning activities of daily living and cognitive concepts, e.g. time perception and imagination [8]. They usually benefit from a fixed daily structure which is offered by the use of pictograms, planning boards and pictogram agendas [9]. Technology has the potential to support learning activities of daily living and cognitive concepts and can contribute to community participation of clients with intellectual disabilities [8, 10].
Nowadays, the development of technological applications that support independence in daily living for people with intellectual disabilities has increased. These applications can be displayed on handheld mobile devices and use several instructional methods to guide people to complete tasks, e.g. video (self) modelling; video feedback; visual and audio prompts and cues; picture cues and picture schedules [11, 12, 13, 14]. A review of Mechling (2011) showed that a variety of handheld personal data assistants (PDAs) are available to support clients with intellectual disabilities by using reminders and tools for time management, transition aids, prompts, and models for completing multi-step functional tools. Despite the positive results reported in these studies, it is a challenge to develop adjustable PDAs because ‘one size does not fit all’ [15]. The Picto Watch was developed for clients with intellectual disabilities. It contains a digital display on which activities are presented using pictograms or photographs and it provides an audible signal as a reminder of activities. The Picto Watch contributes to the independence of clients and it supports their daily structure [16].
The deployment of the above-mentioned applications offers support to clients with intellectual disabilities and they assess the use of touch screen technology as user-friendly and valuable. Unfortunately, the studies show that most technological applications are still under development and the products and services are not yet ready for general use. Furthermore, limited scientific research was found about the developmental process of applications and about applications that solely focus on the support of independence in structuring the day and in the performance of daily activities for clients with intellectual disabilities. Gillespie et al. reviewed the relationship between assistive technology for cognition (ATC) and cognitive function. Apart from the development of a dedicated classification system, they identified areas for future research and development in this application domain [17].
In 2010, a joint project was started by a small-scale group accommodation (SSGA) and Saxion University of Applied Sciences to develop a memory application that structures and supports daily activities for clients with dementia. Details of the development of this application, methods and findings are published elsewhere [18]. Based on the available technology at that time and in accordance with the activity scheme of the users, the daily structure was digitised and visualised using touch screens in the living room and in bedrooms which were interconnected via a wireless network. Due to positive findings [18], De Lichtenvoorde, a care organisation for people with intellectual disabilities, in the East of the Netherlands saw potential for the further development of this application to support their clients in their daily structure. Although the memory application was developed for people with dementia, the idea was to build on earlier work done for another target group with different functional limitations that also need support in structuring their daily activities.
Two development cycles were needed to develop a memory application that was tailored to the needs, wishes and abilities of clients with learning disabilities. In addition, the present study was aimed at providing a clear insight into the developmental process, e.g. lessons learned. This was illustrated by these two development cycles, whereby the following principles were taken into account:
Research design
To identify usability issues and needs for further development of the memory application, a mixed methods study, i.e. both qualitative and quantitative research methods, was used. During the development process, clients and carers were involved as active participants. Using a ‘participatory design’ [19, 20], an inventory of user’ needs, wishes, and abilities was made and integrated into the memory application.
Development cycles
On the basis of user-involvement methods [21, 22], the following phases were carried out. This represents a complete development cycle.
Phase 1: Gathering data with regard to the desired design. Phase 2: Converting these data into a programme of requirements. Phase 3: Testing to ensure the memory application meets its requirements. Phase 4: Piloting in a ‘real life setting’ to evaluate its usability and to gather directions for further development.
The progression from one phase to another was not a linear process and was conducted in an iterative process, i.e. return to an earlier phase of development based on feedback or new information collected in a later phase. This provided the opportunity to optimize the memory application constantly to the needs, wishes and abilities of users and this resulted in two development cycles in a two-year period (September 2010–May 2012). During the phases 1–3, users fulfilled roles as informants and advisors and in phase 4 users performed roles as objects of study and informants [23]. In the development cycles, technological experts of a software company worked together from the start with those experienced in the needs of persons with mild intellectual disabilities, e.g. informal and formal carers of De Lichtenvoorde, and with Saxion researchers. The result of development cycle II is a provisional end version of the memory application.
Several iterations took place in which the users were invited in several rounds to test whether the prototypes matched their expectations. Mock-ups were created and discussed and processed in the programme of requirements. Based on user experiences and discussions, prototypes were refined. Next, user tests were performed to ensure that requirements were met and to work on further refinement of the application with regard to usability issues.
Methods pilot, development cycle I (phase 4)
Setting and participants
The first pilot took place between January 2011 and April 2011. The touch screens were placed in the apartments of individual clients (
A purposive sampling strategy, consistent with the methodology and aim of this study, was utilised to recruit users [24]. Inclusion criteria for participation in the pilot were:
Clients need support in their daily structure related to (I)ADL performance. Clients are able to handle the memory application.
The individual clients were adults with moderate intellectual disabilities as well as auditory impairments. The group accommodation is home to clients between the ages of 13 and 17 years with mild intellectual disabilities as well as behavioural problems.
To investigate the effect of the memory application on independence ((I)ADL performance), a pre- and post-test design was used. An observation list was developed based on the Groningen Activity Restriction Scale (GARS) [25] and the assistive technology scale [26]. The list consisted of nine items related to waking up, personal hygiene, breakfast, departure and return to the daily activity centre, household activities, dinner, the evening programme, and other activities such as social activities and sports. These items were operationalized into sub-items consisting of statements that were related to the item. At the pre- and post-test, the current state of disability/independence in (I)ADL performance of clients was measured by two research assistants through observations of clients. Additional structured interviews with clients and formal carers were conducted to discuss remarkable observations in (I)ADL performance. At the post-test, the usability and needs for further development of the memory application were also mapped out using semi-structured interviews with clients together with formal carers.
Data analysis
Overall, three types of data were collected and used for the analysis: (1) participant characteristics, (2) completed observation lists and (3) notes and descriptions of the interviews at post-test. The observations and additional interviews related to (I)ADL performance of clients at the pre- and post-test were analysed and compared using tables. A deductive content analysis, based on the framework analysis [27], was performed as the researchers were particularly interested in themes regarding the usability and needs for further development of the memory application.
Methods pilot, development cycle II (phase 4)
Setting and participants
The second pilot took place between March 2012 and May 2012. Touch screens were placed in the bedrooms of clients (
Again, a purposive sampling strategy [24] took place and the same inclusion criteria for participation as for pilot 1 were applied. An inclusion criterion was added, namely that it was possible to formulate personal goals for functionalities related to (I)ADL for which the application could be used. All clients were adults between the ages of 18 and 45 years and seven clients had mild to moderate intellectual disabilities. Four clients had autism spectrum disorder, of which one client had autism without an intellectual disability.
Methods and study procedure
The effects of the memory application on independence ((I)ADL performance) were investigated using a pre- and post-test design with an updated version of the observation list developed in the first pilot. The items of the observation list were adjusted to the setting of the pilot and the level of independence were operationalized (e.g. without difficulty, with some difficulty, with great difficulty, with help and with complete help). In line with the previous pilot, observations of clients were performed by two research assistants and additional structured interviews were conducted with clients and/or formal carers to discuss remarkable observations in (I)ADL performance. Prior to the start of the pilot, personal goals of clients regarding the memory application were identified by formal carers and described in the care plans. During the semi-structured interviews at the post test, experiences of the usability and needs for further development of the memory application were explored. In addition, it was evaluated to what extent personal goals were achieved. These interviews were recorded with a digital voice recorder and transcribed verbatim.
Data analysis
Three types of data were collected and used for the analysis: (1) participant characteristics, (2) completed observation lists and (3) notes and transcriptions of the interviews at post-test. Differences in the ability to perform (I)ADL at the pre- and post-test were analysed using the Wilcoxon Signed Rank Test in IBM SPSS Statistics (version 22.0). The interviews at post-test were analysed using a deductive content analysis based on the framework analysis [27]. The analysis of the observations and the interviews was carried out by two researchers (YK and MdO).
The first version of the memory application as a result of the first three phases of development cycle I.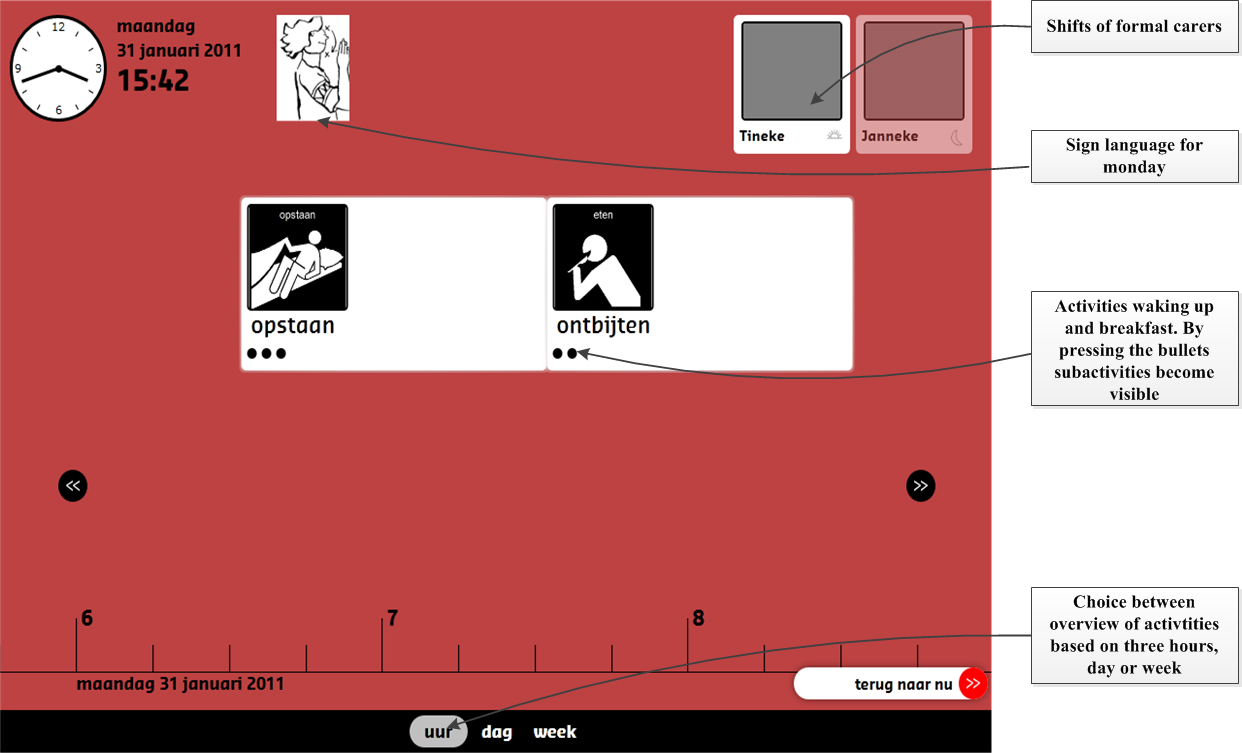
The Institutional Review Board was consulted and approval was granted prior to the start of the data collection. Based on the assessment of the protocol for the target group dementia [18], we received approval by a representative of the Medical Ethical Committee for this research proposal. Prior to participation in the pilots, the clients, informal carers of clients and formal carers signed an informed consent form. Other ethical principles – not harming participants, violation of privacy and deception [28] – were taken into account during recruitment, data collection, analysis and reporting.
Findings
Findings, development cycle I
Progress, memory application (phases 1–3)
For the implementation of the memory application for clients with intellectual disabilities, the planning board had to be revised to meet the requirements of this group, i.e. living conditions and the nature of the disability. With regard to the living conditions, the version of the memory application for people with dementia [18] was not suitable for use in geographically divided locations; the individual screens were connected to a local database through an unencrypted connection. The most important requirement for the care organisation was that multiple locations could be managed using the same web interface. This was implemented by connecting the screens to a central (cloud) web service through a secure connection. The screens themselves used Microsoft Silverlight. The back-end was written in Microsoft’s ASP.NET (a web application framework) and ran on Microsoft’s SQL Server (a database system). The graphical user interface (GUI) was also revised.
With regard to the nature of the disability, it was necessary to adapt the pictograms for people with intellectual difficulties and to have the possibility to introduce activities with the support of a variety of pictograms; to divide activities into sub-activities to enable the application to assist clients using a step-by-step method; to make use of sign language and different colours for communicating the different days of the week and to provide the client with shifts of formal carers. These were displayed with a picture of the employee, combined with a symbol of the shift (rising sun, sun, moon, bed). See Fig. 1.
The second version of the memory application as a result of the first three phases of development cycle II.
In development cycle I, data from informal and formal carers were collected with regard to the desired design, using mock-ups, and the software company converted these data into a programme of requirements. Formal carers trialled the application prior to its implementation to assess if it met the requirements. Additional wishes and needs were collected and sent to the software company. Based on these data, an update of the memory application was developed. Subsequently, this version was installed on touch screens and the first pilot was started.
Nine clients (two individual clients and seven clients of the group accommodation) participated in the pre-test. Two clients of the group accommodation withdrew from participation in the post-test. One client moved to another location and one client did not provide consent. Although clients used the application, conclusions regarding the limited contribution to the independence of clients should be interpreted with caution. This was the result of limited experienced ease of use, installation errors due to limited internet connection and lack of knowledge as to whether the functionalities of the application could support clients in (I)ADL activities. Working with the application was experienced by formal carers as an ‘extra workload’; it was not integrated in the care process and the care organisation did not support the implementation adequately. Clients and formal carers saw potential in a more user-friendly memory application and suggestions were given for future development, such as options for optimizing the back-end, e.g. to make the introductions of activities and shifts of formal carers less time-consuming. In addition, options were given for a more personalised use of the application, e.g. the use of pictograms or photos, analogue or digital display of time, the possibility of a total overview of activities during the day (to minimize the need for scrolling), etc. To ensure a personalised use, as well as an optimal integration in the care process, formal carers need to formulate personal goals in consultation with clients for the activities in which the application can support them, for example increasing independence in meeting appointments and planning. It is desirable that formal carers act according to these goals and that they are described in the care plan of clients. In conclusion, the memory application and the implementation strategy needed some major revisions, and therefore another development cycle was initiated.
Sub-activity screen from the last version of the memory application.
Progress, memory application (phases 1–3)
Based on the experiences and wishes encountered during the first pilot, the memory application was updated; see Figs 2 and 3. The user interface of the memory application was changed from a Microsoft Silverlight GUI to an HTML 5
Which period is shown (part of day/day/two days /week/unlimited) Analogue/digital display of time Pictograms or photos Extended or simple display of day screen Choose the ability to check off ‘done’ activities Choose the ability to ‘rate’ a done activity Choose the ability to add/edit/remove activities from the planning Choose the ability to log on/off
Overview of client characteristics and results of the intervention related to independence
*ID
Another design choice was to display all information on one screen, without needing to scroll left or right. Navigation changed from pushing navigation buttons to swiping left or right, or by clicking on activities. General technological developments also enabled some improvements. Working with a cloud database made it possible to access the application from any location. The disadvantage is that if there is no internet connection, the application, e.g. the display of pictograms, does not function optimally. This was solved by syncing local databases with a cloud database in the background, resulting in an offline availability of the memory application.
In development cycle II, the findings of the previous pilot were converted into a new programme of requirements and new mock-ups were created. User tests, by means of performing tasks, were performed by colleagues of the Saxion researchers and by formal carers on several locations of the care organisation to ensure that the memory application met its requirements. Informal carers and clients had the possibility to casually try and evaluate the application by means of a simple questionnaire concerning important user requirements, because it was presented in different lobbies of the care organisation. Results of the user tests and questionnaires were sent to the software company and were included in the update of the memory application. This process continued until the application met its predetermined requirements. A project organisation supported the implementation and integration of the memory application in the care process. Multidisciplinary co-operation translated into roles and tasks that were described in a protocol, e.g. ICT support (help desk) and the availability of memory application experts in various locations who could be consulted by formal carers. Several workshops took place with formal carers and clients to familiarize them with the operation of the application and to help formal carers formulate personal goals for functionalities related to (I)ADL which the application could assist clients with. After the first three phases of development cycle II, a second pilot was carried out.
3.2.2.1 Results from the observations
A total of seven clients participated in the pilot. In the post-test, one client withdrew from participation because of relocation. For six clients, the memory application contributed to a not statistically significant (
3.2.2.2 Findings from the interviews
At the post-test, six interviews took place with clients (
Realisation of personal goals
Formal carers confirmed that personal goals were reached by five clients. In four cases this was already visible at the post-test. Although not scored using the observation list (see Table 1), the interviews also showed that client 3 achieved his personal goal. The main goal of this client was to decrease the shuffling of daily activities during the day by using the memory application.
“We have noticed that client 3 is very strict in performing daily activities when they are submitted in the memory application. There is less discussion with client 3 about keeping appointments” FC client 3.
In three cases, formal carers indicated that the pilot was too short to evaluate more and long-term effects of the memory application on the personal goals of clients (as well as increasing independence). Overall, using personal goals in the application increased the integration of the memory application in the care process and contributed to a more personalised use of the application. Some personal goals of clients were less clearly defined and sub-goals were needed, for example increasing independence in meeting appointments and planning by using a sub-goal of being on time in the daily activity centre. In addition, personal goals were less transparent for other formal carers because they were not always described in the care plan.
Independence of clients
In four cases, formal carers perceived that the memory application had an added value to increase the independence of clients. In most cases, this was related to less control needed regarding the daily structure offered by formal carers. This contributed to the self-management of clients.
“We have to think less on her behalf. She sees what is going to happen; although she doesn’t have any notion of time, she knows the sequence of activities. When she hears a signal, she knows it is time for coffee. This is easier for her compared to constantly asking her formal carers. In the meantime, she can do things for herself and that gives peace of mind” FC client 1.
Advantages of the application
Clients and formal carers indicated that the application provided an overview of the activities, offered structure and clarity, and ensured peace of mind to the clients. Four clients appreciated the signal played at the start of an activity and formal carers mentioned that this contributed to the peace of mind of clients who had no notion of time.
“It is nice to hear a signal when something is important. Some activities are on the memory application, but you forget it when you walk away. It is nice to get reminded by the sound” client 7.
Formal carers indicated that especially when activities consisted of several sub-activities, the application provided structure, so that clients knew how to complete an activity.
“It was so nice for him to see exactly how he should clean the room. By checking the memory application in his room, he could see the steps we made together and the signal reminded him of it. But still we had to remind him to look at the memory application when it was time to clean the room” FC client 6.
In addition, there was less discussion with clients about performing activities or tasks when an activity was displayed on the screens.
Disadvantages of the application
The clients and formal carers were content with the perceived ease of use and usefulness of the memory application. However, there were some barriers, e.g. clients needed to get used to operating a touch screen; the flickering screen was annoying because one client suffered from epilepsy; one client perceived the screen as too big; the time of changing pages was in some cases too fast, so that clients did not have the opportunity to read things; stress perceived by clients due to installation errors and when no updated version of the planning of clients was available. Formal carers were limited in adding changes because not all carers were authorised.
Understanding the use of the application
Most clients understood the function and use of the memory application. One client only looked at the pictures and one client only selected the information that was most important to him. However, clients needed more instructions and constant reminders to ‘fully’ understand the function and use of the memory application. Formal carers acknowledged that it was their responsibility to make the memory application understandable for clients and to explain that other supportive means, such as pictogram agendas, were replaced by the application.
“In the beginning, he wanted to use the pictogram agenda as well as the memory application and we did not want to use two systems. So this was very clear for him and now he never speaks about the agenda” FC client 3.
In addition, it is important that formal carers remind clients to look at the application and take the time planning of clients into account.
“We have to pay attention to time, we have to get used to this. We cannot let her wait for half an hour” FC client 2.
Future challenges
All formal carers agreed that the memory application had an added value for clients and they would like to increase the use of the application among other clients within the care organisation. Most frequently mentioned was the wish for a mobile version of the application and for informal and formal carers to be able to enter appointments remotely.
“Maybe it is possible to make the application available on my mobile phone, so when I am on my way I can still see the things I have to do” client 7.
Remarkably, one client indicated that it would be nice to have more pictograms for one activity because the client associated the pictogram with activities for different kind of purposes.
“Normally I cycle to the daily activity centre, but in the weekends when I am free and I cycle with my parents, I also cycle to the daily activity centre” client 4.
These development cycles resulted in the following major revisions of the application:
Starting with a local database moving to a cloud database, and then moving to a combination of a local and cloud database. Adding sub-activities with the aim of assisting clients through a step-by-step method. The display of shifts of formal carers. Extension of functionalities that can be modified according to personal preferences, e.g. choosing pictograms or photos. The use of the application on mobile devices, such as smartphones and tablets. This also supports the use of the application by clients living in the community. Carers can enter and control appointments remotely. Accounts for informal carers through authorisation by clients or formal carers. The integration of Sclera pictograms (a selection of 11,000 pictograms) in the application.
Overall findings, development cycles integrated
The two development cycles provided broader insights into issues concerning the needs and design of a memory application for people with intellectual disabilities. Using participatory designs, a more tailor-made application was developed. The results of the final pilot showed that the memory application was generally perceived (by clients and formal carers) as easy to use and added quality to structure and supported daily activities, which resulted in clarity, peace of mind, independence, and stimulation of the self-management of clients with intellectual disabilities. In the final development cycle, the importance of a multidisciplinary co-operation was recognised and a project organisation was implemented. This confirms the results from previous research that important determinants for successful implementation of technology are, among other things, ease of use, relevance for patients and the importance of an adequate innovation strategy [29].
Lessons learned
Despite an increase in the perceived ease of use, the results showed that some clients needed more instructions to completely understand the function and use of the memory application. Previous studies showed that people with mild to moderate intellectual disabilities are capable of operating a touch screen, but most of them need coaching to learn new skills [14, 15], for example by errorless learning and trial and error learning [30]. Therefore, future research should also focus on which coaching interventions are most effective to support people with intellectual disabilities to use applications on mobile devices or computers. A structured and systematic training should be organised to avoid frustration and confusion both for persons with the disability and persons assisting that person [31].
The efficiency and effectivity of the application can be further improved by formulating well-defined personal goals and sub-goals in consultation with the clients and informal carers. Goal Attainment Scaling (GAS) can be a helpful method to involve users in the goal-setting procedure [32]. Second, both formal and informal carers need to act according to these goals and these goals should be part of the care plan. This requires a ‘shift’ in carers’ approach from supply-driven care to client-centred care aimed at improving the personal strength of clients with disabilities. Working with the memory application can help to adapt the activities more accurately to the needs, wishes and abilities of clients. Third, formal and informal carers should update their knowledge and replace other supportive means, such as calendars, planning boards, pictogram agendas, and medication alarms with the memory application. That way, they can improve the self-management of clients and efficiency of care by stimulating independence of clients.
In the present study, the software developer performed the data collection and carried out analyses of the wishes and needs of the clients in the first three phases of the development cycles. Although the data were systematically collected, the methods used in these phases could have benefitted from a closer co-operation between developers and researchers.
For reasons of comparability and to be comprehensive, the usability of the memory application should be evaluated according to the three quality levels of the design: (1) system quality (user-friendly and safe); (2) content quality (understandable and meaningful) and (3) service quality (adequacy) [33, 34, 35]. Furthermore, it is necessary to facilitate a process evaluation simultaneously. According to Alwin et al. (2013), outcome and process evaluations have different objectives and complement each other, resulting in an adequate innovation strategy [36]. Ideally, technological development and implementation strategies are organised ‘hand in hand’, since they influence each other.
Strengths and limitations
The strength of this study was the multidisciplinary collaboration, during the development cycles, between experts on the needs of persons with mild intellectual disabilities (informal and formal carers), ICT developers and researchers. This approach contributed to a tailor-made version of the application. Furthermore, using pilots in real life settings, insight was gained in the challenges associated with introducing new technologies. For example, carers should adapt their way of working more accurately to the wishes, needs and abilities of clients.
A number of methodological characteristics of the study are relevant for interpretation of the outcomes. First, informal carers were less involved in the pilots. However, the role of informal carers is becoming increasingly relevant and they are also able to stimulate the acceptance of technology by people with disabilities [36]. Scherer et al. (2005) stress it is also important to consider the user’s environment and support system as key elements for the successful integration of assistive technologies [37]. Second, the pilots were aimed at supporting the development of a tailor-made memory application. However, further research with a larger sample and study period is necessary to generalise the results of the final pilot in terms of effectivity of the application. Last, the chosen innovation strategy was not evaluated, as the focus of the present study was on the outcome of the technology development instead of an implementation strategy.
Practical implications and conclusion
In conclusion, the final memory application was valued as useful and easy to use. This qualitative study suggests that the application has the potential to contribute to the independence and self-management of clients with intellectual disabilities. For successful integration of the memory application in the care process, well-defined personal goals should be laid down in the care plan of the client and formal and informal carers should act according to these goals. The presence of a project organisation had a positive effect on the integration of the memory application in the care process. After tailor-made changes as a result of new development cycles within other vulnerable targets groups, the memory application was implemented in five care organisations and made available for different vulnerable target groups, such as people with intellectual disabilities, autism with and without intellectual disabilities, early-onset dementia and acquired brain injuries. Most clients use the memory application on the tablet. This may be an important contribution to the field. The application was not developed for one target group with a specific functional limitation, but for people with different functional limitations and a similar need for support. The development of new applications will be more efficient if we build on earlier work done for other target groups that need self-management support due to similar problems.
Footnotes
Acknowledgments
We are grateful to the clients and the formal and informal carers of De Lichtenvoorde for sharing their experiences and their co-operation. We also thank the students of the Faculty of Health, the Faculty of Social Work and the Faculty of Creative Technology of Saxion University of Applied Sciences for their participation in this study.
Conflict of interest
We thank the Dutch province of Gelderland, which partly funded this study. The province played no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; or the preparation, review, or approval of the manuscript.