
Abstract
BACKGROUND:
Amyotrophic lateral sclerosis (ALS) is a severe neurologic disease. Affected patients suffer from a gradual loss of functional capacities. The use of assistive technology and devices (ATD) can help them sustain their autonomy and ability of social participation.
OBJECTIVE:
The objective of this study was to analyze the experiences with ATD and to identify issues related to the use of ATD among ALS patients and their caregivers.
METHODS:
Semi-structured interviews were conducted with five ALS patients, five caregiving relatives, and five professional caregivers within a group discussion. Questions related to the living and support situation, expectations to and experiences with ATD, related problems and usage barriers.
RESULTS:
Three main areas that affected the experiences with ATD of ALS patients and their caregivers could be identified: usability of ATD, stigmatization due to ATD and the ATD supply process. Inadequate ATD and ATD supply negatively affected the patients’ quality of life and constituted a burden for caregivers.
CONCLUSIONS:
The presented study results give an important overview about the experiences of ALS patients and their caregivers with ATD. Strategies to approach identified issues could involve the implementation of a case management, patient empowerment, and an adaptation of ATD to meet user requirements.
Keywords
Background
Amyotrophic lateral sclerosis (ALS) is a neurologic disease impairing the upper and lower motoric neurons with a subsequent deterioration and death of these motoneurons. Consequently, affected patients suffer from a gradual loss of functional capacities up to the point where no voluntary movements can be initiated. ALS is a rare disease with an estimated prevalence between 1.44 and 6.25 / 100.000 inhabitants [1]. Early symptoms include a decreased muscle functionality of the extremities, falls, breathing problems, or impaired tongue movements [2]. In later stages, patients gradually lose their ability to move, inevitably caused by a total loss of motor control. Consequently, their need for care involves every aspect of life with the help of a multidisciplinary team [3]. At the same time, in the absolute majority of cases, cognitive abilities remain intact [4]. Therefore, ALS patients not only need an intensive and multidisciplinary care program, they also have a high demand for social participation and autonomy while not being able to fulfil their demands without help [3].
Due to the inevitable loss of functional capabilities, ALS patients become more and more dependent on the use of assistive technology and devices (ATD) to help them sustain their autonomy and ability of social participation. According to the World Health Organization (WHO) ATD are those whose “primary purpose is to maintain or improve an individual’s functioning and independence to facilitate participation and to enhance overall well-being” [5]. The American Assistive Technology Act of 2004 describes ATD as “any item, piece of equipment, or product system, whether acquired commercially, modified, or customized, that is used to increase, maintain, or improve functional capabilities of individuals with disabilities” [6]. A broad variety of ATD is available for ALS patients. They comprise but are not limited to life-supporting measures such as ventilation machines and feeding tubes, communication systems such as computers with eye-gaze control systems and writing tableaus, as well as mobile aids such as powered wheelchairs and lifter systems. Most of them incorporate complex technologies like computer interfaces, voice or even eye movement recognition to account for the level of functional decline the patients with ALS suffer from. Persons suffering from ALS therefore show a high need of ATD [7].
A qualitative study identified several factors with the potential to increase the quality of life of severely impaired persons of different age groups [8]. These especially comprised the capacity of ATD to help overcome a person’s impairments, barriers and environmental obstacles as well as reduce social isolation and increase life quality. A review about ALS patients and augmentative and alternative communication (AAC) technology revealed its immediate acceptance by 90% of the persons and a final rejection rate of only 4% [9]. Nevertheless, various studies raised the issue of problems using ATD. A study with stroke patients demonstrated issues with the use of ATD for the support of mobility in nearly every second patient [10]. A telephone survey with ALS patients showed high frequency rates for mobility and communication ATD, but also revealed discrepancies between received usefulness and satisfaction of for portable electronic devices. However, the reasons were not investigated [11]. A research about eye tracking technologies in persons with ALS demonstrated usability issues and iterative processes linked to demotivation in use, but a higher acceptance in patients with more severe conditions [12].
Studies about ATD in patients with ALS are mainly looking at specific types of ATD and very little of them provide the reasons for low satisfaction rates. Moreover, formal and informal caregivers are not included, who, however, play a crucial role in patient care and ATD supply processes. Thus, neither the experiences with nor the effects of ATD were examined in their full range and depth. We therefore performed interviews as part of a mixed-methods study with ALS patients and informal and formal caregivers. The aim was to (i) assess their experiences with ATD and ATD supply processes, to investigate (ii) the perceived usability and (iii) barriers of ATD usage in the daily routine, as well as (vi) their requirements to ATD in order to provide a clearer understanding for the relevance of ATD for patients with ALS and their caregivers.
In order to understand the findings in this publication, it is important to take a closer look at their supply situation within the German healthcare system. The German healthcare system consists of the statutory health insurance with 89.27% of all insured persons, and the private health insurance with 10.73% of all insured persons [7]. ATDs are financed differently according to the insurance type. Statutory healthcare companies mostly have contracts with ATD suppliers or pay them directly. Private health insurance companies have individual contracts comprising individual scope of health services with their members and reimburse the patients’ payments, therefore most privately insured persons have to pay ATD suppliers in advance [8]. One major factor forcing up the statutory healthcare expenses for the provision and financing of ATD from Euro 5.25 billion in 2005 to 7.82 billion in 2016 is the central role of ATD provision within the German healthcare system [9]. The need for a specific ATD is identified by a medical doctor, often through requests by patients or health professionals such as nurses or therapists. The need for the ATD is then verified by the insurances and is either accepted or rejected, leaving the patients and relatives with different options to object to the decision, organize private funding or refuse the acquirement. In an analysis of a German-based care-network for patients with ALS, ATD provision for ALS patients as well as rejection rates of proposed ATD provision by the patient or the insurer was evaluated [10]. In this study, rejection rates by the insurance companies were between 29% and 49%, those by the patients were nearly 10%. Reasons for rejection were not provided.
Methodology
The interviews were performed as part of a requirementss analysis for the research and development project “ROBINA – robot-supported services for an individual and resource-oriented care of patients with ALS”.
Participants
The interviews were conducted with ALS patients as well as caregiving relatives of ALS patients and professional caregivers specialized in the treatment of patients with severe disabilities within a group discussion. ALS patients were included with at least 18 years of age, a clinical diagnosis of ALS (according to the revised Al-Escorial criteria) and the ability to speak without major effort. They were excluded when showing cognitive impairments, psychological issues such as depression and when given no written consent (either by patient or legal representative). Caregiving relatives were included with at least 18 years of age and related to an ALS patient as well as taking part in his/her caregiving. They were excluded when showing cognitive impairments, psychological issues such as depression and when given no written consent. Professional caregivers were included who were a certified nurse and had experience with nursing ALS patients for at least one year. They were excluded when given no written consent.
Data collection and procedure
For these interviews, a group of researchers with experience in qualitative research as well as a medical doctor specialized in the treatment of patients with ALS including ADT provision, developed the interview guideline. This guideline consisted of questions related to past and current situations in the interviewees’ lives (living and caregiver/support situation, expectations to and experiences with technology, and related problems and usage barriers). Interviews with patients were held at an outpatient clinic for ALS patients at the Charité Universitätsmedizin Berlin. Interviews with relatives of ALS patients took place in the ALS outpatient department or at their homes, two of them were conducted via telephone. The group discussion with the professional caregivers was performed in a nursing home for patients with severe disabilities. The same two researchers were present during all interviews. Both researchers are trained in performing interviews with different patient groups as well as health professionals and have several years of experience in qualitative research. All interviews were recorded with an audio device; additionally, relevant information was noted during the interviews in a standardized protocol form. The interview guideline was pretested with at least one representative of each target group (patients, caregiving relatives, professional caregivers) in order to test consistency and comprehensibility. All patients, relatives and professional caregivers received information material about the aim of the study, study process, data protection and gave their written consent prior to the study. The Ethics Committee of the Charité Universitätsmedizin Berlin approved this study (no. of approval: EA1/121/17).
Data analysis
All interviews were recorded and fully transcribed using F4 software and analyzed by two scientists trained in qualitative research analysis, according to the principles of a systematic content analysis [13]. The analysis comprised the repetitive listening to the records, structuring, paraphrasing and finally coding the interview content into main categories and sub categories, independently by the researchers who performed the interviews. Subsequently, the researchers compared the emerged categories, discussed any discrepancies in the coding process to reach consent and developed a joint category system. This process consequently required several revision iterations, changing existing and adding newly identified categories that had not been included in the interview guideline. The ‘four-eyes’ principle was used in order to avoid errors and ensure the validity of the collected data. The data from the interviews contained overall 15 main categories and 128 subcategories. Relevant categories for answering the research question related to everyday and social life, ATD assessment, assessment of ATD supply, and requirements to ATD and ATD supply. In a further step, the interview content grouped in those categories was aggregated to one generalized statement per corresponding subcategory. The indicated categories can be seen in Table 1. The results were then structured in a logical order for this publication and will be presented and discussed in the following paragraphs.
Main categories and corresponding subcategories processed for this publication
Main categories and corresponding subcategories processed for this publication
Based on the qualitative analysis of the interviews, the following categories were identified: 1), experiences with ATD: usability, stigmatization, supply situation, 2), consequences of inadequate ATD and ATD supply: workaround, fear of technology failure, undersupply and oversupply, time expenditure, and 3) requirements for ATD and ATD use.
Study sample
The five ALS patients interviewed in our study were between 50 and 79 years old, four of them were male. The interviewed relatives were between 50 and 83 years old, two of them were male, all of them were their partners and had experience in caregiving them. The professional caregivers were between 38 and 48 years old, all of them were female and had experience in nursing ALS patients. For more information about socio-demographic data, please refer to Table 2.
Socio-demographic data of study sample
Socio-demographic data of study sample
The study sample of ALS patients showed mainly functional limitations for mobility, movement of arms and hands, fundamental needs in personal hygiene, food intake and social participation, apart from severe limitations in leisure activities. Restrictions in mobility manifested mainly in the form of inability to walk. However, most patients perceived the loss of arm functionality as the main concern and linked it to a reduction in activities of daily living and personal hygiene, resulting in an increased dependency of caregivers and ATD.
Most frequently, the ALS disease adversely affected eating and drinking. Being not only a basic human need but also playing an important role in the patients’ and relatives’ social lives, a restriction in eating and drinking may have severe consequences for the quality of life of affected persons and may even affect the relationship with their social environment. “We used to eat out a lot, but not anymore” (Relative, A01).1
All quotations were translated from German into English.
Other restrictions the study sample related to the loss of body functionality were all kinds of leisure activities such as operating a TV or radio, driving a car, going for a walk and maintaining personal relationships. “The one thing I really regret is that I cannot stroke my own dog anymore” (Patient, P03). Many of the patients were forced to give up leisure activities during the course of ALS due to a loss of functional abilities. Again, the effect of the disease on the quality of life and on social participation was the focus and clearly showed the powerlessness of the affected persons and their relatives. “That was last year, I could hold it [a camera] and get on my knees and so I could take photos, this year, it is not possible anymore. Therefore, I gave up my hobby” (Patient, P01).
In general, ALS patients were dealing with their health condition and were aware of its consequences. This could be seen as an important precondition to adequately assess the need for support in the form of formal and informal caregivers, as well as ATD or supporting measures.
When asked about the general satisfaction with ATD, the interviewed patients, informal and formal caregivers mostly expressed their appreciation for the possibility to use ATD in their daily lives. One professional caregiver summarized her gratitude, “it is great, that such assistive devices were actually created for ALS patients. Of course, sometimes it is time-intensive. But just think about communication systems, it is very nice for ALS patients, they have the possibility to communicate with us and to continue social contacts” (Professional caregiver, Pf01). However, more detailed questions about the usage of and experiences with ATD revealed several issues and concerns.
Usability of ATD
Over the course of the interviews, the construction of ATD and the lack of crucial features were often criticized, directly affecting the usability. “With this software I can write very quickly, but it has no voice output. So anybody I communicate with has to read the words while I write them, and they often finish the sentences for me; this is annoying.” (Patient, B10). So even a benefit in comparison to other systems can quickly diminish when other parts of ATD are insufficient for the users and leave them frustrated. Apart from insufficiently designed or programmed systems, deficient devices may also lead to frustration among the user groups. “The control smiley2
The eye control system uses colored smileys to display the correct head position for an optimal control. A green smiley stands for the optimal position, a yellow smiley for a reasonably good position and a red smiley for a poor position. Please refer to Fig. 1 for an illustration.
Screenshot of a Grid3 eye-control showing the control smiley.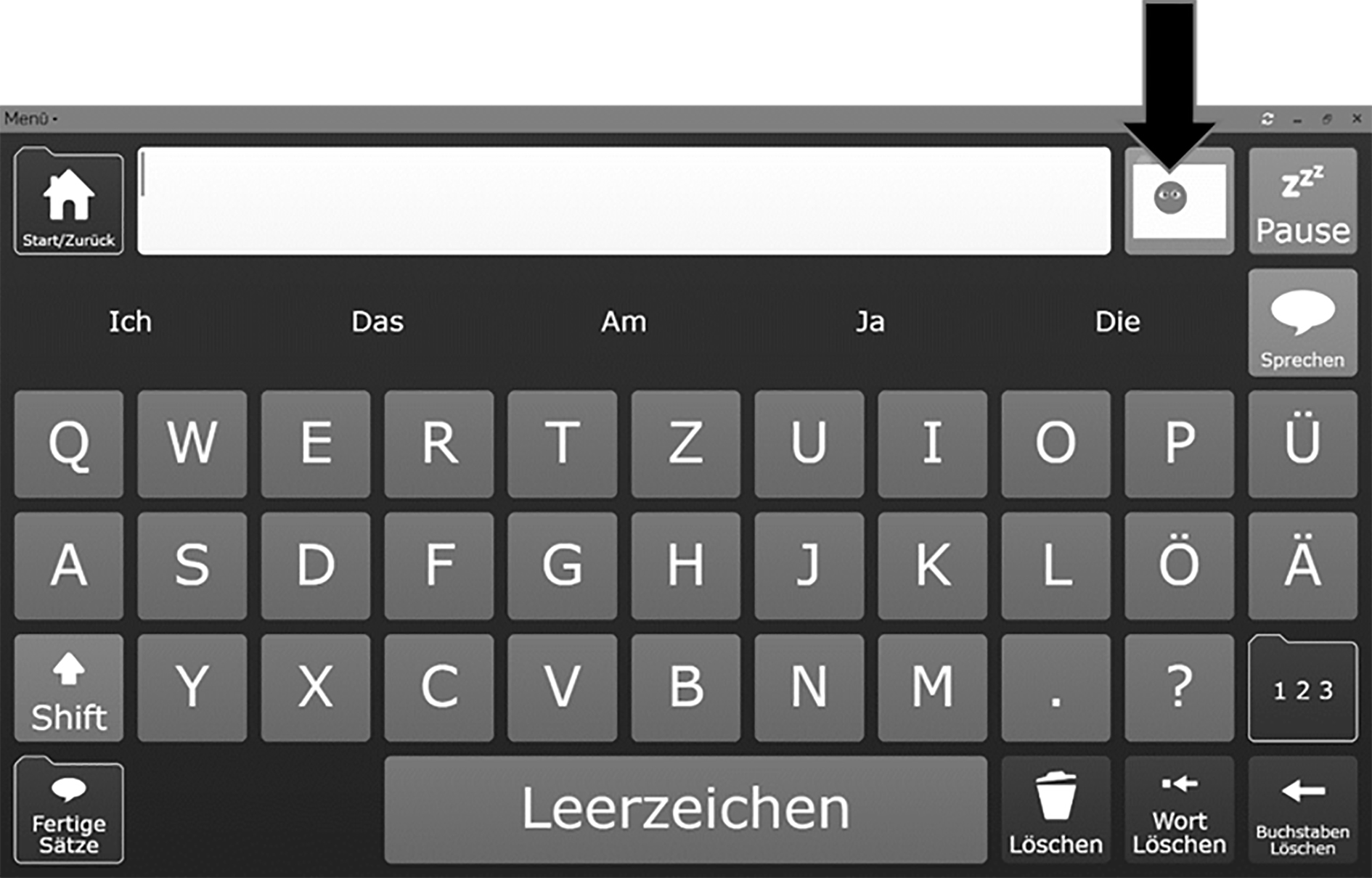
The interviews demonstrated the limited adaptability of ATD to the individual needs of ALS patients and a related uselessness of this ATD. “I don’t think this [ATD operation by joystick] would constitute a problem at the onset of the disease. As soon as the disease proceeds, however, it is questionable if they can operate it with their eyes. That is my concern. Because we have seen patients with ALS that was proceeding very quickly and thus, in a very short time, those patients could not use their communication systems or other ATD anymore” (Professional caregiver, Pf03). This quoted experience is representative for the vast majority of interviewed participants. They owned a range of well-working ATD that became useless due to the lack of operation alternatives during the progress of ALS and the related loss of body functionalities. On the other side, ATD with a high range of functionalities were described as being very complex, effecting a work overload especially in professional caregivers who generally took care of a number of patients and handled a great variety of technologies in a limited timeframe. “Yes, the variety could be a problem. […] We are 15 to 20 professional caregivers, and all of us have to be trained and have to manage all this ATD” (Professional caregiver, Pf04). “Especially ventilated patients, they need an extraction unit, a ventilation system, a carriage system, a lifter system, a multifunctional wheelchair, maybe a communication system. […] And this is time intensive” (Professional caregiver, Pf02). A poor usability and the lack of an intuitive handling amplified the problem, and led to operating errors or a restricted use by patients as well as formal and informal caregivers. “And our caregiver thought she had turned it [the alarm] off […] But it was awful, this alarm the whole night. I was sleeping and she was sitting next to it. The next morning, I don’t know what happened, but suddenly the alarm was off” (Patient, P03). This quotation describes impressively how a low usability could negatively affect the quality of life for both, patients and caregivers.
The size, weight and bulkiness of ATD were deemed very important particularly for handling and transportation purposes. Caregivers reported about the need of a third person or a strong person, especially for the handling of transfer aids, wheelchairs, and corresponding component parts. While this directly affected informal and professional caregivers, ALS patients also phrased concerns regarding the bulkiness of assistive devices. “They sent a female caregiver who weighed 50 kg, and had a normal height, and then she had to push me with that wheelchair. That was fairly unbearable” (Patient, P03). Another interviewee stressed the dependence on other people: “The walker has to be transported [to a leisure group], some people are not capable to do that, and some people don’t want to do that” (Patient, P02). The dependence on task-appropriate formal caregivers constituted a concern among patients and informal caregivers: “Last week, they sent us a strong and tall male caregiver, he took me down in that thing [wheelchair], and we went for a walk for an hour, almost one and a half hours. […] It was very nice to be outside and check out my old bike route, but that was only possible with this caregiver” (Patient, P03). This statement suggests that the patient cannot go for a walk with a different caregiver, who may physically not be capable of lifting the wheelchair; accordingly, the construction of the ATD created limitations in its determined use. Moreover, several interviewees disapproved of the maneuverability of ATD and the degrees of freedom. According to them, this concern was related mainly, but was not limited to, wheelchairs, and often resulted in a limited usage and scope of application. “I have a wheelchair at home, it is a bit, let’s say clumsy, not really maneuverable, I manage to sit in it but I cannot move around in my flat” (Patient, P08).
In this context, it was not uncommon among the study sample of ALS patients to possess two devices for the same field of application. This was especially the case when ATD turned out to be constructed for only one environment, i.e. home and non-home environment, not considering the mobility of the users and the related needs. “We own two ventilating machines, one with external rechargeable batteries for when we are travelling. The other one runs on corded electricity. It also runs without being plugged in, for about one hour, which is not long enough” (Relative, A03). Wheelchairs were often described either to be too bulky for the home environment, or not powerful enough for the outdoor environment. This emphasizes both the patients’ need for mobility and social participation as well as the consequences of a restricted ATD use, which had to be compensated by acquiring additional ATD. The option to test and compare ATD before ordering it provided by ATD suppliers, was evaluated positively but criticized to be too short. A short evaluation time does hardly reveal any issues relevant for the daily use of ADT, e.g. power issues. As a result, users may be unsatisfied after ATD implementation when they discover issues and limitations. “Half an hour or an hour, they show it to you. However, sitting in it [a wheelchair] for 12 hours, this is completely different. […] You should be able to test it for a week in order to assess it profoundly” (Patient, P08).
Another issue raised by some patients was the topic of stigmatization. Stigmatization is still an issue among people who use visible assistive technologies, whether those are small like hearing aids or more present ones such as wheelchairs. In our study sample, stigmatization due to ATD led to a complete refusal of the same in a few cases. “I didn’t want to have an emergency button, it makes me look sick” (Patient, P08). In this case, the patient who refused to use an emergency button described a situation in which she fell on the floor and could not get up anymore. Only by the help of her assistant dog, her son could be informed. Even after this experience, she still refused to use an emergency button, suggesting that stigma was even worse. ATD may have a negative psychological effect and make the user feel different or even inferior to others, and therefore socially excluded. “[…] when people look down at you, when you sit in a wheelchair, you develop inferiority complexes and you think ‘I want exist no longer’. It makes such a different in the interaction with others” (Patient, P08). However, some interviewees suggested this feeling may be overcome and that social contacts play an important supporting role. “[ATD use in public] We still do it [going out for dinner]. Even if people look at us strangely” (Relative, A01). The social environment as a source of support may therefore play an important role for the compensation stigmatization issues. I fact, even with discrimination. “And then it was December and the streets were slippery and full of snow and the bus driver was not very amused, a wheelchair user during rush-hour traffic, it delays everything. And then I drove him” (Relative, A09). All of those quotations underpin the consequences and fear of stigmatization of, but not limited to ATD.
Supply situation
In our study, experiences with the supply processes of ALS patients were very diverse. Overall, the processes were evaluated either completely positive or negative. Mostly, patients, their relatives and caregivers positively assessed the general ATD supply opportunity and cost coverage by the German health care system. “The whole supervision let me tell you, from [ATD supply] approval to delivery, everything happened really fast. I was pleased with that” (Patient, P02). Expressing their gratefulness for the support they received, many of the interviewees approved of the availability of professional caregivers. It became very clear during the interviews, that the at home provision of patients of a certain disease level would not be manageable without professional nurses, especially a 24 hours care. “You need to consider that one [ALS] patient occupies one caregiver. That is, taking into account the lack of professional caregivers here in Germany, we are grateful that it is possible at all” (Relative, A05).
Repeatedly, consolidated knowledge about corresponding laws and persistence was quoted to be a prerequisite for a smooth supply process, making it clear that patients and in the process-involved relatives need to be very well informed. That included specific knowledge regarding the application and objection processes, such as law texts and deadlines, in order to confront health insurances and build up pressure. “I got it [a specific ATD]. My health insurance is great, you only need to justify the claims, you need to assert yourself, you need to know the law and you simply need to hold on, call them and keep asking. […] My Berlin dialect is helpful” (Patient, P08). A high level of health literacy may be beneficial, which is not necessarily always given. Other patients and relatives criticized the rejection of ATD by health insurances. In most cases, refusals due to insurance contract conditions were reported, mainly concerning privately insured patients. Rejections within the presented sample usually led to either private funding or donation-based provision with ATD, or in the worst case to a supply shortcut. “So, after it [transfer lifter] was rejected [by the health insurance company], […] his former colleagues collected money and then they gave us those € 7,000” (Relative, A09). This illustrates the financial dependence on third parties when a funding by oneself is not possible and underlines the interference of health insurances on the patients’ lives. The following statement clearly emphasizes this. A patient described a situation when she wanted the insurance company to take over the costs for an assistant dog. In the end, it was declined as the insurance company would only take over the costs for an assistant dog for persons with severe vision impairments. Especially the way the insurance employee talked to her left her frustrated: “I also experienced this situation where she [an insurance employee] told me ‘you have ALS, what do you want with an assistant dog?’ Those are situations, well. I am still alive […], and I will not pass away tomorrow […] and I am outdoors every day. Some [insurance] people, oh I don’t know.” (Patient, P08). The refusal of ATD especially interfered with the lives of ALS patients and their social environment when it was the subject of mobility and, in particular, communication, one of the central requirements of human beings. “We wanted to have a communication system. […] We don’t have it, we don’t get it funded. They [the health insurance] rejected it, telling us, ‘it is not listed in our service catalogue’” (Relative, A01). According to the interviewees, the supply with ATD sometimes took a long time, but was initiated not until the need emerged. Therefore, ALS patients repeatedly experienced long intervals of limited social participation or even communicability, which was described to be very stressful and burdensome for both patients and relatives. “This is the worst thing, you need these things and you need them now. Immediately. Within the following two days and not the next two, four, eight weeks or even later” (Patient, P08). Patients stated that they felt left behind and not taken seriously.
Consequences of inadequate ATD and ATD supply
The consequences of an inadequate ATD and ATD supply as described above were very diverse, but ultimately led to a reduced quality of life in ALS patients. In accordance with the identified challenges, the corresponding consequences will be discussed in the following paragraphs.
Workaround
In order to overcome an inadequate supply with ATD, or to maintain the patients’ feeling of autonomy and independence, patients and relatives created several workaround strategies. The strategies in the present study sample involved three different approaches: 1) misuse of objects and 2) behavioral changes, and 3) a combination of both. The most common applied strategies described in the interviews involved solutions to overcome height by the use of little chairs. Due to limitations in arm functionality, patients cannot reach certain heights, e.g. a kitchen worktop. Therefore, they needed to climb on an elevation. Often, in-advance preparations by relatives or caregivers were necessary, for example the provision and appropriate positioning of objects. “You did this a lot, you climbed on that little chair, when I was not home, and I had prepared everything [put food in the microwave] and he just pushed the button” (Relative, A01). The reason for these kinds of workarounds was due to not only the limited functionality and lack of appropriate ATD, but also the wish for autonomy and self-sufficiency, even if it means more effort. “I have to add that he really tries to do everything he can himself. Some things last long, longer, and it is painstaking, but he makes the effort. If I do these things, it is much faster. But he still does them” (Relative, A01). “Generally speaking, it is very important for the patients to do specific things they are still capable of doing” (Professional caregiver, Pf04). Many workaround strategies concerned the patients’ communication, often compensating insufficient or immobile communication systems, or situations that interfered with the use of those systems such as sunlight making an eye-controlled operation difficult or impossible. “He writes [the text] in his voice output program and then copies the text into the email, so he doesn’t have to use the small letters of the email program” (Relative, A09). The users implemented those kinds of workarounds as a compensation of poor usability or insufficient systems. Apart from the fact that not everybody might be able to develop workaround strategies, they can be cumbersome, effortful and time-consuming; some might even be dangerous for the patients, e.g. climbing on a chair. The interviewees frequently reported the need for individual adaptation of ATD, often realized by caregivers or relatives. Adaptations included the simple attachment of a computer mouse to the hands of a patient with a tape, up to self-constructed boards for resting a patient’s arm in a certain height. Inspiration to create or adapt aids often emerged from the patients’ specific knowledge about their needs and requirements, or from word-of-mouth within self-aid groups.
Fear of technology failure
Technical failure of and negatively related experiences with assistive technologies or devices frequently resulted in the fear of such failure situations. “This is an extreme concern, because we experienced this situation a lot where we would be stuck on the street due to power issues [of the wheelchair]. This is not controllable. […] Tonight we will attend a school meeting, I am really worried, can we charge the battery again, please” (Relative, A06). As a result, negative experiences of such kind caused stress in both affected persons and informal caregivers and in some cases even adversely affected social participation. Especially life-supporting ATD is the focus of concerns in the context of technology failure, making patients and caregivers likewise aware of their technical dependency and equally causing stress. “So there you are, in that awful situation that the ventilation system is not working, and when you are travelling on your own, well, you don’t want to even think about that” (Relative, A09). Furthermore, safety-related concerns played an important role, in order to avoid dangerous situations and harming a patient. “He did not want the lifter system to be fixed on the ceiling directly above him. He is afraid it might fall down and hit him, while he is not able to move away” (Relative, A09). Safety-related concerns often adversely affected the appropriate implementation, use and handling of ATD. Consequently, technical devices could often not unfold their full potential with regard to work facilitation or support due to the deviation from the required application criteria. Instead, additional operations to compensate the lack of support functionality had to be introduced. Another patient linked the daily health status to ATD operation concerns: “Yes, that it [ATD] does not get out of control in, I don’t know, when I am having a bad day or time. It is important that it stops or disables its functions then” (Patient, P07). To a certain degree, the interview statements reflected the users’ powerlessness with regard to malfunctioning and a mistrust in technology after negative experiences.
Undersupply and oversupply
Long delivery times had a huge impact on the interviewed patients and their social surrounding by averting communication, mobility, and social participation. Frequently, the interviewees described situations in which acquired assistive devices were useless at the point of implementation, as the disease had progressed during waiting time and the patient was not able to handle the device anymore. “We saw ALS patients, the disease progressed really quickly, and they could not use communication computers or other devices anymore” (Professional caregiver, Pf03). Consequently, latent times in supply may lead to an undersupply and oversupply of ADT at the same time. An undersupply occurred during the waiting time, in this case identified as an insufficient supply with ATD, determined as being essential for the patient. Patients experienced a lack of autonomy – lost functionalities could not be compensated by ATD in time. As a result, specific areas of their lives were directly affected, e.g. communication or mobility, which rose frustration among both patients and caregivers and ultimately but quickly leads to a decrease of life quality. In turn, an oversupply with ATD persisted after having become useless, characterized by wasted time and opportunity costs such as costs for delivery, material and work force. Again, this is frustrating for patients and their social surroundings to receive the requested ATD finally but not being able to use it (anymore) and seeing it abandoned in the corner of their home. “I can’t use those orthoses any more, I cannot walk anymore. Unfortunately, you wait a long time for those things, too long, and then when you want to use it, it’s not possible anymore. This is bad” (Patient, P07).
Time expenditure
The variety of functions and features per ATD required a high amount of time for the correct settings. Additionally, the situations and needs of ALS patients can change within a short time frame. Due to the decline of body functionalities for example, iterative setting adaptions were necessary. A poor usability also effected a time-intensive handling. “It took me hours to program 16 names into the communication system until I realized that the eye control interferes with the process of programming. […] And like I said, I don’t have the nerve to do that and to adjust all those things, and these are barriers” (Relative, A09). Frustration among patients and caregivers especially arose when ATD was used to communicate needs or sorrows, as well as for social engagement, demonstrating the dependence from technology and making aware of personal limits. “[Alphabet board] When it’s not fast enough, when he wants to say the word before he even manages to show it completely. Often this ends in tears. And then you start again. Of course, this is time-intensive” (Professional caregiver, Pf04). The interviews showed quite clearly the patients’ will of social participation and maintenance of social relationships. Therefore, ATD facilitating mobility and communication plays a very important role in their lives. Nevertheless, there is a huge discrepancy between the patients’ functional status and the unaltered functional status of their social environment, which makes a social participation difficult even with the most sophisticated available ATD. Therefore, device malfunctions or a slow operation especially interfered with the patients’ and relatives’ social lives “It takes very long, so I leave the room and tell him: write it down, I’ll come back in a moment” (Relative, A05). Professional caregivers of the group discussion stressed the fact that the wasted time due to iterative processes and complex settings would be needed urgently for important nursing measures.
It becomes evident that an inadequate supply with ATD can have a negative impact on the quality of life of ALS patients and their social and in care involved environment. Therefore, it is necessary to focus on the needs of the users and to consequently clarify their requirements.
Requirements for ATD and ATD use
To overcome technology-related barriers, the presented sample was asked to express their requirements to ATD for ALS patients. One of the main approaches to counteract an insufficient or incorrect operation according to the participants constituted a training workshop. The instruction workshops offered by the suppliers were mainly evaluated positive. “If I have the training license, I train my colleagues, […] and if not, we get it from somewhere. […] If that doesn’t work, then the construction company visits us and trains us” (Professional caregiver, Pf04). Instruction workshops were criticized for not always involving informal caregivers or for being held too late, leaving the caregivers responsible but short of crucial information. “There was an emergency situation with the coughing assistant system and she [the patient] said ‘do something’ and I said ‘of course, do something’ and I think the instruction workshop was held half a year after that” (Professional caregiver, Pf03). Additionally, relatives and professional caregivers described language barriers among professional caregivers as issues. “The language barrier is also a problem, when a colleague does not speak the language and can therefore not operate the system and edit the settings in order to use it correctly” (Professional caregiver, Pf02). This is a major issue as professional caregivers are often the person in charge, especially in 24 hours or inpatient care, and patients have to rely on their expertise even with handling ATD. ATD suppliers should therefore offer comprehensive but easily comprehensible ATD training workshops, immediately after implementation with regular repetitions. Additionally, ATD should offer specific attributes for a correct and easy handling. The most frequently mentioned attribute ATD should provide is a quick and easy operation and launch of features, besides a quick and simple acquisition of operation skills, with the aim to reduce time expenditure. “It [ATD] should not be that complicated and time intensive. […] It should not take an hour to start that device” (Patient, P01). Few patients had requirements to the appearance of ATD to make it look nicer. Stigmatization could be an issue here or the association of healthcare ATD with the severe conditions of the disease, as remarked in the following statement: “they should make them more colorful those wheelchairs, when I look at the armrests, this wheelchair is three weeks old. It is worn off just because your arms lie on it and then everything is in black. We are not grieving” (Patient, P08). Another central requirement of ALS patients and their relatives concerned the mobile use of ATD. “That the device or machine is where I am. So that it can be used mobile, somewhere, fixable on the table” (Patient, P03). To stay mobile is a big issue in patients with ALS. In our sample, both patients and relatives emphasized the patients’ social activities and therefore stressed the need for mobile ATD. “My friends collect me from home, we play cards and then they give me a lift back home, including my walker” (Patient, P02).
Discussion
This paper presented the experiences with the use of ATD among ALS patients and informal and formal caregivers, and, in relation to that, assessed the consequences of inadequate ATD and ATD.
Usability
Based on the results of our research, usability has a huge impact on the quality of life of ALS patients, leading to frustration and a burden on both the patients’ and caregivers’ side. While many studies suggest a reduction of caregiver burden by the implementation of ATD, there is also evidence in the literature, that ATD might increase caregiver burden to a certain extent e.g. due to complicated handling, physical strain and an increased time investment [14, 15, 16]. Therefore, it is essential to evaluate the benefits of ATD individually. Nevertheless, generalizable improvement approaches for ATD could be derived from the interviews. A smooth mobile use of ATD was demanded by the installation of long-lasting and rechargeable batteries, as well as easy transportation by compact and lightweight ATD to enhance mobility and social inclusion. Apart from that, communication systems should receive a special attention due to their important role for social engagement and impact on quality of life [17]. A poor usability can quickly lead to frustration among patients and potentially reduce an information exchange with their social environment. Therefore, a quick operation of communication technologies, i.e. typing texts, also by different control options and with an equally fast voice output can enhance a normal communication between patients and their social environment, which is very important for their quality of life. An inclusion of patients’ and caregivers’ requirements in ATD development, also with regard to living circumstances and living environments, is a central objective to increase usability and avoid ATD refusal. On the other side, a large number of ATD models due to customization purposes seems unreasonable. It would require a certain level of technology expertise and the ability to quickly adapt to new systems and result in a chaotic market situation. As a solution, ATD should be constructed modular-based, e.g. by offering different operation possibilities or expandable parts. This could facilitate the use of ATD according to the patients’ altering needs, reduce the model variety and associated adaptation periods on the users’ side, as well as have a positive effect on the supply situation, as an undersupply would be counteracted.
A further limiting factor that was frequently mentioned during the interviews was the need for one or more persons additionally to a caregiving person for the appropriate use of ATD. Especially with an increasing number of persons in need of care and at the same time a decreasing number of professional caregivers due to the demographic change in OECD countries [18], this may result in the immobility of ALS patients, social exclusion and frustration. This issue should be addressed by improving usability rates. ATD should be constructed for the use by one person regardless of his or her physical characteristics, e.g. by the option to disassemble heavy parts or by installing lightweight constructions. However, the alteration and adaption of ATD might technically or financially not be feasible [19, 20], therefore the key approach should focus on a comprehensive assessment of needs prior to an ATD supply process, involving patients, caregivers and relatives.
Several studies with different vulnerable patient groups using ATD analyzed factors influencing technology acceptance [21, 22, 23]. They revealed that apart from usability and perceived benefits, a person’s social environment consisting of family and friends, formal and informal caregivers, or teachers and peers, can have a huge impact on ATD acceptance and enhance ATD use. However, the interviews revealed that formal and informal caregivers were not systematically involved in ATD instruction workshops or that workshops were held too late. These results were also proved in several studies evaluating ATD supply processes [24, 25]. As specific trainings can significantly improve ATD handling [26, 27], it is essential to instruct and familiarize informal and formal caregivers with new technologies and to provide easily accessible information about ATD. Moreover, language barriers should not constitute a problem for the adequate use of ATD. ATD, training workshops and instruction manuals should offer simple language and make use of symbols or pictograms. Both might also overcome usability issues.
Stigmatization
Experiences with stigmatization in the context of ATD use within a health context has been researched extensively and has been suggested to be one of the main reasons for ATD abandonment [28, 29, 30]. ATD design aspects may play a relevant role as described in the interviews and suggested in the literature [31], but other determinants such as social acceptance, age appropriateness and self-esteem must be considered [28]. Strategies to counteract stigmatization should exceed ATD adaptations and educate people about the necessity of ATD in order to empower people with impairments and disabilities. Relatives and caregivers play an important role with ATD acceptance in patients as stated above. Therefore, educational strategies about the benefits of ATD use should target this specific gatekeeper group.
Supply and supply process
Issues with ATD supply were verified in a study from 2018 analyzing ATD supply among patients with ALS in Germany between 2011 and 2014 [32]. Only two thirds of indicated ATD reached the patients, 26.3% of ATD were rejected by health insurances and 9.8% by the patients themselves. Latent times in the supply process were also analyzed and showed that they were high among electronic devices such as augmented and alternative communication (AAC) systems (96.11
Limitations
Even though the sample size was small with 15 study participants, the interviews gave an important insight into the lives and experiences of ALS patients and their formal and informal caregivers using ATD. Since the nature of the study was qualitative and only persons affected by ALS were included, the results are less generalizable. Additionally, other persons involved in ATD supply, e.g. health care supply companies or medical doctors, were not included in this study. However, relevant information concerning usability and acceptance of ATD among ALS patients and in care involved persons could be derived from the interviews, additionally to information about ATD supply and resulting consequences for the user groups. A follow-up study is planned, using quantitative research methods in a bigger sample size with different patient groups, to verify the results of the present publication.
Conclusion
The presented study results give an important overview about the experiences of ALS patients and their formal and informal caregivers with assistive technologies and devices. A poor usability constituted the main cause for handling issues, negatively affecting the quality of life of patients and leading to a burden among caregiving relatives and professionals. Apart from that, the study showed that stigmatization issues could have a negative impact on the patients’ quality of life and even result in the refusal of ATD. Another outcome of the study was the ATD supply situation. The interviews demonstrated major differences according to the insurance type. Strategies to approach these issues could be the implementation of a comprehensive case management to improve the ADT situation, the empowerment of patients to avoid stigmatization, and an adaptation of ATD to meet user requirements by user-centered design approaches and modular-based ATD development.
Footnotes
Acknowledgments
The authors thank all affiliated partners of ROBINA (Roboter-unterstützte Dienste für eine individuelle und ressourcenorientierte Intensiv und Palliativpflege von Menschen Patienten mit ALS) who supported the research as part of the R&D project.
Conflict of interest
None to report.