
Abstract
BACKGROUND:
Lack of parental knowledge about augmentative and alternative communication (AAC) systems and how to incorporate them into daily life can be a barrier to AAC use. To support children who are learning an AAC system, parents must understand how to model communication during naturally occurring activities.
OBJECTIVE:
The objective of the study was to examine the effects of parent instruction on modeling AAC use in naturally occurring activities.
METHODS:
An eight-step instruction model was used to teach four parents of children who use AAC to provide partner-augmented input (PAI) using the core vocabularies on their children’s speech-generating devices (SGDs) during core family leisure activities. Communication Sampling and Analysis (CSA) was used to compare parent and child language at pretest and post-test.
RESULTS:
All parents demonstrated the ability to perform all of the components of successful PAI (slow rate, model, respect and reflect, repeat, expand, stop) as determined by review of an observation checklist completed during coaching sessions. Parents significantly increased percentage of utterances modeled on their children’s SGDs between pretest and post-test measures. The percentage of unique words modeled (i.e., type-token ratios) by each parent suggests variety in models at post-test. Three of four child participants demonstrated increases in unique words used following parent instruction.
CONCLUSIONS:
Parent instruction can increase parent modeling and child SGD use.
Keywords
Introduction
Augmentative and alternative communication (AAC), the supplementation or replacement of natural speech and/or writing using aided and/or unaided symbols [1], can be invaluable in helping children with complex communication needs express themselves at home. However, providing the appropriate piece of technology alone does not ensure successful communication [2]. Rather, the success of a communication interaction between a person using AAC and a communication partner will depend heavily on the skills of the communication partner [3]. “Being an effective communication partner or AAC facilitator is not intuitive. It often requires one to change long-established, unconscious ways of communicating” [4, p. 12]. Interaction patterns of communication observed in parents of children using AAC often include controlling the topic, dominating conversational turns, and being more directive by requiring specific responses [5, 6]. These behaviors may affect communication development in children with complex communication needs [7].
Educating significant communication partners (e.g., parents, teachers) can be of great benefit in increasing participation in daily interactions by individuals using speech-generating devices (SGD) [8, 9]. Recent analyses of communication partner training programs suggest that there is consistent evidence that communication partner instruction improves both the skills of partners and of people who use AAC [10, 11]. Furthermore, research suggests that communication partner training can be used effectively as an intervention strategy for individuals using AAC [10].
Young children spend most of their waking hours at home, making family members key communication partners. Well-informed, well-educated parents can be valuable to a child who is learning an AAC system [12, 13, 14]. Parents are not only frequently acting as interventionists, but they are also important communication partners of a child using AAC. Furthermore, families are critical to evaluating the effects of AAC intervention [15]. Family involvement is also often the only constant in public school systems facing critical shortages of speech-language pathologists (SLPs) and frequent staff changes [16, 17].
Family-centered care has become preferred practice for a variety of medical and educational programs, including those serving individuals with developmental disabilities [18] and the importance of family-centered practice has also been acknowledged in the provision of AAC services [19, 20, 21]. Family-centered practice is characterized by recognizing family diversity, respecting families, treating them with dignity, sharing information, and engaging in professional/parent collaborations [18, 22]. In studies designed to assess family perspectives on AAC, parents rated the need for increasing knowledge of assistive devices as a priority [19, 20] and reported lack of knowledge about AAC systems and how to incorporate them into daily life as a barrier to AAC use [23]. Family satisfaction has been found to increase when clinicians recognize parent needs and provide guidance regarding AAC [20, 21, 23] and failing to recognize issues important to families can lead to dissatisfaction and device abandonment [24].
Parent education is one method used to increase family knowledge regarding children’s SGDs. “Parent education (or parent training) broadly refers to programs or trainings designed to provide parents with information or teach them skills” [25, p. 96]. Parents of children with autism spectrum disorder and developmental disabilities have successfully demonstrated the ability to implement a variety of language teaching strategies following participation in parent education programs [26, 27]. Furthermore, a recent meta-analysis of parent-implemented language interventions demonstrated significant positive outcomes on receptive and expressive language skills, receptive and expressive vocabulary, expressive morphosyntax, and rate of communication in their children when compared to a control group [28].
Live and online parent training in AAC has been linked to positive changes in children’s communication [29, 30, 31]. Parent-implemented naturalistic behavioral interventions such as Joint Attention Symbolic Play Engagement and Regulation (JASPER) combined with use of a speech-generating device (SGD) resulted in improvements in spontaneous communicative utterances, novel words, and comments [32]. Parent training in AAC has also been shown to increase parent provided communication opportunities, child communication, and parent responses to child communication [30]. In addition, increases in family comfort level with operating an SGD, supporting communication [21, 29] and feelings of successfully interacting with their children [33] have been reported. Parent support has been identified as a contributor to positive outcomes for individuals who use AAC [34, 35]. When families are not given adequate support regarding integrating an AAC system into a child’s daily activities, problems can arise and the AAC system may be viewed as a burden. Negative family attitudes and perceptions can become barriers to AAC implementation and lead to device abandonment [23, 36, 37]. Kaiser and Wright [38] suggest that to adequately support children who are learning language using an AAC system, adults must have specific skills in three different areas: 1) communication mode; 2); strategies for responding to children’s communication; and 3) strategies for modeling.
Partner-augmented input (PAI), also referred to as natural aided language, aided language modeling, or aided language stimulation, is a modeling strategy whereby communication partners use the child’s AAC system themselves by pointing to the symbols on the child’s SGD while simultaneously talking. “Augmented input can be broadly defined as an umbrella term for systematic modeling input from two or more modalities, one of which must include the learner’s AAC system” [39, p.157].
PAI use (a) increases vocabulary comprehen-sion [40]; (b) increases symbol comprehension and produc- tion [41, 42, 43]; (c) increases production of multi-symbol messages [44], (d) increases use of morphemes such as past tense –ed and plural –s [45]; and (e) increases utterance length and complexity [46]. Overall, use of this strategy is associated with gains in pragmatics, semantics, syntax, and morphology, and is effective in individuals of varying ages, disabilities, and language skills [47, 48, 49]. A recent review suggests that PAI meets the criteria to be considered evidence-based [50]. Little is known about the effects of parent education in using PAI during routine daily activities in the home.
Five training procedures have been commonly used and associated with successful parent training programs. These include (a) verbal instruction and/or instruction manuals, (b) in vivo practice, (c) role playing, (d) modeling by the trainer, and (e) reviewing videos of intervention being implemented [51]. The use of parent coaching, a collaborative effort between an SLP and parent, is particularly important in interventions with children with complex communication needs [33]. The literature on adult learning suggests that the use of a combination of training elements results in optimal learner outcomes [52]. Parent education programs were also found to be of greater benefit when parents practiced the skills they learned on their own children [53]. Finally, training was most effective when implemented in everyday, meaningful routines and activities [28, 55]. Family leisure activities, in particular, “offer a rich, naturally occurring context for AAC intervention” [54].
In 2005, Kent-Walsh and McNaughton proposed an eight-step instruction model for use with communication partners of people who use AAC [3]. They sought to increase attention paid to the instructional methods that have been associated with instructional success. They stressed the need to identify evidence-based procedures for communication partner instruction in AAC. This model includes multiple training elements seen in successful parent training programs including:
Pretest and Commitment to Instructional Program; Strategy Description; Strategy Demonstration; Verbal Practice of Strategy Steps; Controlled Practice and Feedback; Advanced Practice and Feedback; Posttest and Commitment of Long-Term Strategy Use; Generalization of Targeted Strategy Use.
This instruction model has been used successfully to train instructional assistants in school environments [56, 57] and parents [58, 59]. Increases in child AAC use following partner training were reported. However, the previous studies using this model (a) Focused on a single activity, storybook reading, an activity that may not occur frequently in all homes; and (b) The studies incorporated activity-based communication displays (ABCDs) created specifically for the reading activities rather than the child’s existing SGDs, thus limiting the likelihood of generalization. Furthermore, the studies reported limited data regarding parent modeling behaviors. In 2017, Senner and Baud successfully used this instruction model to teach school staff to provide PAI throughout the school day on a child’s existing SGD [60]. However, there is a paucity of research on using the model to teach parents to incorporate PAI into naturally occurring activities at home.
The objective of the study was to examine the effects of parent instruction on modeling AAC use in naturally occurring activities.
Child demographic information
LAMP WFL
Child language skills
Parent demographic information
This project was approved by the Institutional Review Board of Midwestern University.
Participants
Four parent-child dyads participated in this study. All child participants met the following candidacy criteria: (a) Utilized a dynamic display SGD to communicate; (b) Used commercially available core vocabulary (i.e., one with commonly-used, frequently-occurring words) on the SGD; (c) Used direct selection with a finger (i.e., physically pointed to or pressed a button) to access the SGD; (d) Produced fewer than 10 intelligible words using natural speech; (e) Lived with the parent participating in the study 100% of the time; and (f) Were between 5–10 years of age. The four child participants ranged in age from 5;0 (years, months) to 9;6 (
Diagnoses, length of device use and language skills varied. For additional information regarding the child participants including specific diagnoses, devices, and vocabularies used, see Table 1. For information about child language skills, see Table 2.
All parents participating in the study were mothers and all were married. None indicated any history of hearing or learning difficulties. Parents self-selected to participate in the study and were made aware of the project via posted announcements, letters to local therapists providing services to children with disabilities, and social media. All parents had at least one other child also living in the home. Two parents were employed outside the home and two were stay-at-home moms. All had completed at least some college. Parent income and previous training in AAC varied. See Table 3 for specific parent demographic information.
SMoRRES mnemonic
SMoRRES mnemonic
Informed consent was obtained for all participants, including consent to videotape and collect data logs from each speech-generating device. Prior to participation in the study, parents were asked to complete an online questionnaire regarding child and parent demographic characteristics such as ethnicity, family income, marital status, highest level of education, employment, and other children in the home. Parents were also asked to rank a variety of core leisure activities, “common, low-cost, relatively accessible, and often home-based activities that families engage in frequently,” [54, p. 314], on a scale ranging from 1 (never or almost never) to 4 (always or almost always). In addition, detailed daily schedules were obtained for each parent-child dyad. Evaluating Acquired Skills in Communication (3rd ed.: EASIC-3), an inventory of communication skills for children [61], was administered to each child participant to document the child’s communication skills. Student clinicians determined the appropriate starting level with guidance from a principal investigator and administered the Pre-Language, Receptive I and/or Receptive II skill assessments of the EASIC-3 to each child participant as appropriate to obtain an approximate understanding of the child’s functional level of language and to aid in determining appropriate modeling targets. During testing, student clinicians received 100% supervision from one of the principal investigators.
SGD data logging is the automatic recording of the content and time of language events generated using AAC systems. Data logging was activated on the participants’ SGD at either the time of language testing or at the time of the first pretest videotape, whichever occurred first. In addition, the time was set on the SGD so that data collected have the correct time stamp for later analysis. SGD data were downloaded by the evaluators and used to aid in language sample analysis. Between one and three weeks prior to the initiation of training, the principal investigators videotaped pretest sessions in the home. Parents and children participated in three of their core family leisure activities as indicated on the questionnaire. Two separate pretests were collected within a two-week period. Pretest activities lasted between 5:03 mins and 16:55 mins and had a mean length of 10:08 mins.
Training began with parents participating in a 3-hour group instruction session. During this session, parents completed Step 1, Pretest and Commitment to Instructional Program. Each of the parents was asked to individually watch a pretest videotape of her interaction with her child and to reflect on her own use of the child’s SGD. Parents discussed their strengths and weaknesses in providing PAI on the device with one of the principal investigators. Parents also signed a written commitment to training acknowledging that they were committed to learning to provide PAI. On the written commitment form they also set personal goals (e.g., “Implement the respect and reflect strategy in my modeling and give more/longer pauses as opposed to prompting”). Step 2, Strategy Description, was also conducted during the group training session via a PowerPoint presentation which outlined what PAI is, why it can be useful, and how to model on children’s devices. Step 3, Strategy Demonstration, was conducted via presentation of videotaped samples of PAI being used by families at home.
Step 4, Verbal Practice of the Strategy Steps, was completed using the SMoRRES (slow rate, model, respect and reflect, repeat, expand, stop) mnemonic [60]. See Table 4. The parents labeled and described each step aloud during the training with guidance from the instructors to confirm that they understood the strategies. The principal investigators also led parents through rehearsal (i.e., vocal repetition of the strategy steps) to aid caregivers in memorizing steps involved.
Each family member had a communication device or app with the child’s page set to participate in Controlled Practice and Feedback (Step 5). During controlled practice, parents were asked to generate a variety of practice phrases on the devices as well as to generate phrases to model based on scenarios presented. The scenarios related to activities at home and required parents to think about what types of models they might provide in the situations described (e.g., “Your child pushes away a game you are playing. What could you model on your child’s device to reflect his or her intent?”)
Following the initial training session, families attended eight to nine, once weekly 55-min coaching sessions at the University Clinic with the student clinician. During these sessions, student clinicians modeled device use during each of the three core family leisure activities (Step 4) and parents had an opportunity to participate in Controlled Practice (Step 5) and Advanced Practice (Step 6) with a student clinician providing coaching (i.e., collaborative live observation and feedback). Coaching was gradually faded by the student clinician between Controlled and Advanced Practice. Core family leisure activities were unique to each dyad but remained consistent throughout each week of the training program. Activities included playing a game, eating a snack, watching a video, playing with bubbles, doing a puzzle, and reading a book. However, specific foods, videos, etc., varied weekly, depending on child interest. A principal investigator supervised all sessions.
Parents received access to one of their post-test videos to watch on their own, and a review of their AAC use was completed with a principal investigator following the posttest videotaping (Step 7). During the last two coaching sessions, the student clinician introduced a fourth activity which had not previously been practiced during sessions (Step 8). The generalization family leisure activity was one that had been rated as 3 (often) on the parent questionnaire. Generalization activities included food preparation (i.e., cooking), listening to music, reading a book, and playing with blocks. The participants also discussed strategies for long-term PAI use at home with the student clinicians during their final coaching sessions.
Within 4 weeks after the completion of the final coaching session, two post-test video recording sessions of the same activities occurring in the initial recording sessions were completed. Both post-test videos were recorded within a 2-week period of each other. Post-test activities lasted between 5:00 mins and 28:21 mins and had a mean length of 12:23 mins.
During all videotaping sessions, the mothers were instructed to play/interact with child as they typically would [27]. The researcher did not attempt to influence caregiver behavior in any way. The researcher remained behind the camera and avoided interaction with caregiver and child other than to encourage them to continue engaging in the routine for at least 5 mins.
Data collection and analysis
A pre/post-test research design was used. An implementation fidelity checklist was used to ensure that parents completed each step of the training. Each item was dated and initialed by one of the researchers when it was completed. A student clinician also completed an observation checklist to measure intervention fidelity during each coaching session. Each item on the checklist pertained to a component of the SMoRRES mnemonic (e.g., slow rate, model, respect and reflect, repeat, expand, stop) and student clinicians tallied each time they observed the parent’s use of each behavior. Parent’s proficiency was defined as use of all of the strategies within an activity.
Child and parent utterances from the videotapes and SGD data logging were transcribed (i.e., written down verbatim) into Communication Sampling and Analysis (CSA), an online assessment tool for sampling and analyzing communication behavior in children with complex communication needs [62]. Utterances were defined as sentences or units of language that were separated from other utterances by a pause. Researchers noted whether or not parent utterances also included a model on the child’s SGD. A model was defined as one or more key words from a parent’s utterance being activated on a child’s speech-generating device immediately before, during, or immediately after a spoken message. Percentage of parent utterances modeled were calculated by dividing the number of utterances accompanied by a model by the total number of utterances produced by the parent. Pretest and post-test utterances were compared using a one-way repeated measures Analysis of Variance (ANOVA).
If a model was produced by the parent, researchers noted the specific word(s) modeled in brackets for analyses of the percentage of unique words modeled (i.e., type-token ratio). The total number of unique words modeled on the SGD by each parent was calculated for each post-test activity. The total number of unique words modeled was divided by the total number of words modeled and multiplied by 100 to determine the percentage of unique words modeled for each activity.
Total number of unique words each child independently communicated with the SGD was calculated by counting the total number of distinct words across samples at pretest and post-test. Utterances were considered independent if they were not preceded by a parent prompt. Prompts were defined as a cue or hint provided to the child by the parent to produce an utterance on the SGD. Prompt types included verbal prompts (e.g., a “tell me” or “show me” cue followed by the target word), gesture prompts (e.g., pointing to the target word), or physical cues (e.g., hand-over-hand assistance). If a single button on the SGD contained a phrase or sentence (e.g., “I love you”), that message was listed as a single word for the purposes of calculation.
After the study, parents completed a questionnaire to determine social validity containing seven questions answered using a 5-point Likert-type Scale ranging from 1 (strongly disagree) to 5 (strongly agree) and four open-ended sentence starters. The open-ended phrases included, (a) Things I liked about this process; (b) It would have been better if; (c) Changes I noticed in myself included; and (d) Changes I noticed in my child included. The Likert-type questions were as follows:
Overall, I believe that PAI has been effective in supporting my child’s communication; I better understand how to provide PAI during regularly occurring activities at home; I am more familiar with the language on my child’s device; I found this training useful; I will continue using PAI at home; I think it would be helpful for other family members to attend this training; and I used my child’s SGD more frequently at home.
Number of Unique Words Used by Child Participants
Mean percentage of utterances modeled by each parent on each child’s SGD. Note the significant increase in modeling between pretest and post-test recordings as well as a drop in modeling between the two post-tests.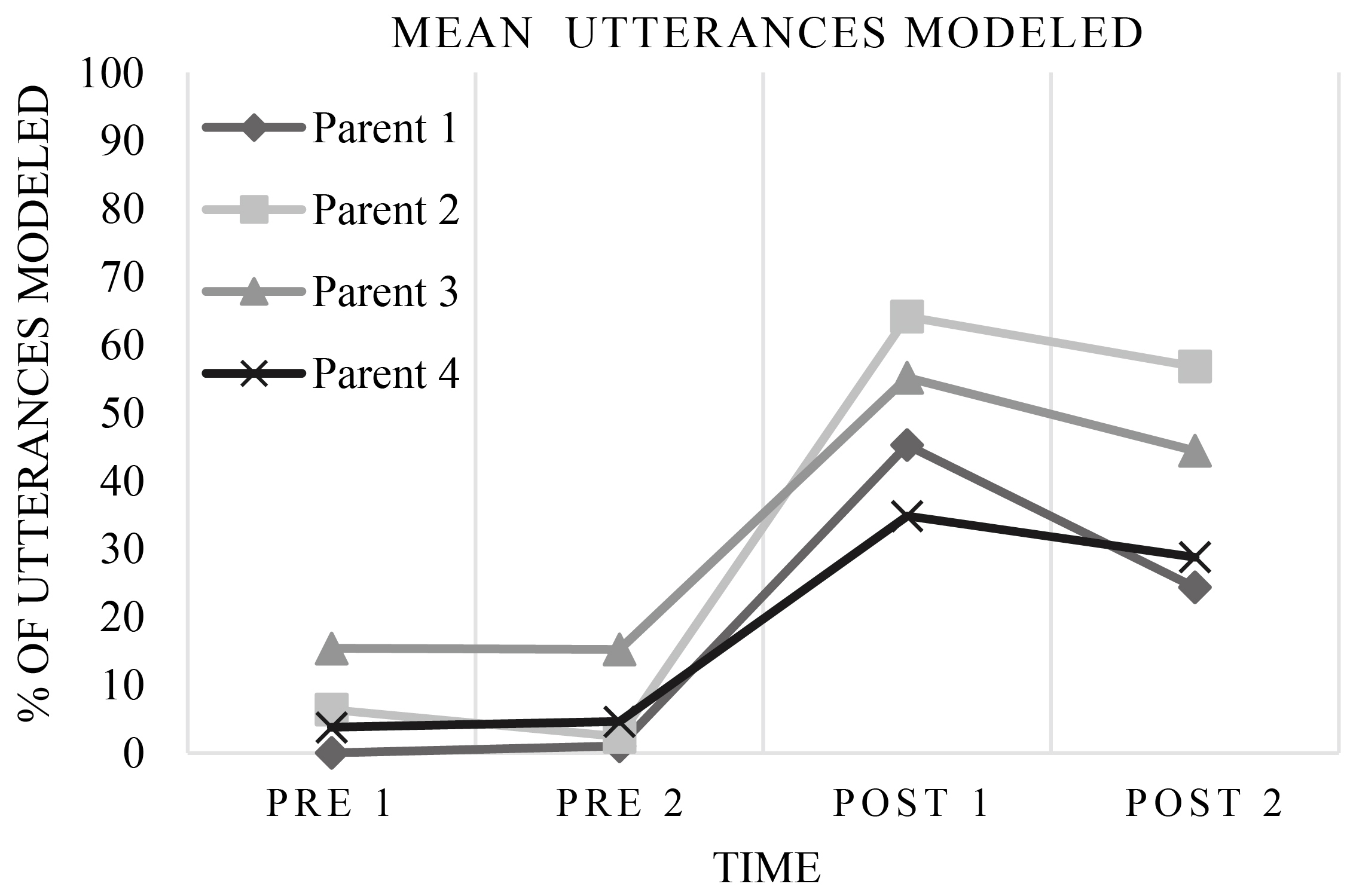
All parents successfully completed all steps of the training program as recorded on the implementation fidelity checklist and also demonstrated the ability to perform all components of successful modeling during each target activity as documented with the PAI observation checklist. A one-way repeated measures ANOVA revealed statistically significant increases in percentages of utterances modeled between the two pretest and the two post-test samples
Each individual parent also demonstrated a statistically significant increase in modeling between pretest and post-test when analyzed using a paired samples
Parent models produced at post-test were analyzed to determine percentage of unique words modeled (i.e., type-token ratio). Unique words modeled varied by activity and ranged from 37.04% to 74.51% (
In summary, parents demonstrated significant increases in the percentage of utterances modeled between pretest and post-test, however a decrease in modeling was seen between the two post-test measures. Parents demonstrated good variety in words modeled as indicated by type-token ratios. Children’s raw data showed increases in unique words used at post-test, however differences were not statistically significant.
Social validity
All parents strongly agreed (
Discussion
Overall, Kent-Walsh and McNaughton’s eight-step instruction model [3]appeared to be effective in teaching parents to model language for children using core vocabularies on their dynamic display SGDs during core family leisure activities. The significant increase in modeling seen is consistent with partner gains reported in a previous study using this model to teach PAI [60]. Over the course of a 12-week period, parents with varying levels of experience and backgrounds demonstrated statistically significant increases in modeling on their children’s SGDs. Group data also revealed statistically significant increases in modeling. However, decreases in modeling were noted at the second post-test. No follow-up visits were done during this study so it is unclear whether modeling would have stabilized or further dropped with increased time after completion of the training. This suggests the need to further assess the frequency and intensity of training sessions and/or follow-up necessary to create lasting changes in parent modeling behavior.
Responses on the social validity questionnaire indicated that parents found the structure of the training package to be beneficial. They also perceived themselves and their children as being more comfortable and confident in using the SGD at the conclusion of the program. In addition, parents noted increase child device use at home following participation in training.
Alant et al. [63] suggest that “although the percentage of modeled utterances provides us with some information, there is no evidence that these modeled utterances … could not have been highly repetitive and stereotyped.” Parents were instructed to frequently repeat targeted vocabulary words (i.e., provide focused stimulation), however producing targeted words in a variety of contexts was also encouraged. Parent models produced at post-test were analyzed to determine percentage of unique words modeled (i.e., type-token ratio). A high percentage of unique words modeled indicates a large amount of lexical variation. The data suggest a variety of words modeled, rather than simple stereotyped exchanges or programmed interactions. This analysis was not performed for pretest data because most parents demonstrated few or no models at pretest and type-token ratio is influenced by sample length.
Despite the diversity in the child participants’ vocabularies, length of device use, and language levels, the use of PAI by parents appeared to have a positive effect on the number of unique words used by three of the four children, however the combined data were not statistically significant. The unique words used by children were heavily influenced by the nature and content of each activity as well as the language level of each child. This inter-participant variability resulted in high standard deviations. This, along with a small sample size, likely affected statistical significance. A larger sample size could possibly demonstrate a significant difference in unique words used.
Clinical implications
The instructional model proposed by Kent-Walsh and McNaughton [3] includes training elements known to be effective in parent instruction. The results of this study suggest that parents can learn to model language on their children’s existing SGDs and also provide varied input during core family leisure activities when trained using this model. It also appeared that there were benefits to some of the child participants in terms of increases in independently generated unique words on their SGD, however these weren’t statistically significant. The authors of the current study agree with previous conclusions that parent instruction results in changes in both parents and children and should be routinely provided as an intervention when children first receive an SGD [10]. This should include teaching parents to use the child’s existing SGD during naturally-occurring activities at home. Furthermore, professionals involved in AAC evaluation and intervention should develop competency in providing parent instruction [24].
Limitations and future research
The only necessary commonality among children using SGDs is a severe expressive language impairment, in other words, children who use AAC are inherently a diverse and heterogeneous population. Children who use AAC may vary in age, diagnoses, language levels, and specific SGDs used. Furthermore, incidence of AAC use is low, resulting in small numbers of participants in many research studies, including the present project. Despite attempts to control some candidacy criteria for participants in the present study, the small number of participants along with inter-participant variability necessitates interpreting these results with caution.
In addition, parents self-selected to participate in the study, therefore results may not be generalizable to other parent groups. In particular, all mothers had some college education, which may have increased their responsivity to this type of program. All mothers were married, which may have afforded them more opportunities to share household duties and thus spend 1:1 time with their children. This type of instruction may prove to be more difficult with single-parent families and/or those with less education. This area warrants additional investigation.
Finally, parents found scheduling and traveling to clinic-based sessions suboptimal. Online programs can increase accessibility of instructional programs to parents who face barriers such as lack of transportation, lack of childcare, and living in a rural or remote area [64]. Online programs can incorporate both asynchronous (i.e., recorded elements) as well as synchronous (i.e., client interactive) services that would allow a clinician to provide real-time feedback such as the coaching provided during controlled and advanced practice. Future research on using this instructional model to teach parents to use PAI using an online program would be valuable to conduct.
Footnotes
Acknowledgments
This project was partially funded by a Midwestern University-College of Health Sciences Research and Facilitation Grant, 2017.
Conflict of interest
None to report.
End nnotes
Appendix
Percentage of utterances modeled by Parent 1 on her child’s SGD. Bubbles: PRE 1 – 0%, PRE 2 – 0%, POST 1 – 30.61%, POST 2 – 21.05%. Puzzle: PRE 1 – 0%, PRE 2 – 1.72%, POST 1 – 57.73%, POST 2 – 15.96%. Snack: PRE 1 – 0%, PRE 2 – 1.23%, POST 1 – 47.37%, POST 2 – 35.96%.
Percentage of utterances modeled by Parent 2 on her child’s SGD. Video: PRE 1 – 0%, PRE 2 – 0%, POST 1 – 91.30%, POST 2 – 74.36%. Snack: PRE 1 – 16.66%, PRE 2 – 0%, POST 1 – 57.41% POST 2 – 55.17%. Book: PRE 1 – 2.44%, PRE 2 – 7.14%, POST 1 – 43.66%, POST 2 – 40.86%.
Percentage of utterances modeled by Parent 3 on her child’s SGD. Game: PRE 1 – 20.16%, PRE 2 – 20.00%, POST 1 – 66.01%, POST 2 – 41.46%. Snack: PRE 1 – 24.74% PRE 2 – 20.78%, POST 1 – 49.40%, POST 2 – 54.72%. Book: PRE 1 – 1.15%, PRE 2 – 4.82%, POST 1 – 50.00%, POST 2 – 37.04%.
Percentage of utterances modeled by Parent 4 on her child’s SGD. Video: PRE 1 – 2.41%, PRE 2 – 5.59% POST 1 – 35.52%, POST 2 – 26.32%. Game: PRE 1 – 7.53%, PRE 2 – 4.07%, POST 1 – 37.73%, POST 2 – 29.41%. Snack: PRE 1 – 1.34%, PRE 2 – 4.08%, POST 1 – 34.15%, POST 2 – 30.59%.