
Abstract
BACKGROUND:
Dynamic exoskeleton orthoses provide assistance needed to complete movements that would otherwise be impossible after stroke. Beyond the demonstration of their effectiveness, the subjective experience of dynamic orthoses also needs to be considered.
OBJECTIVE:
To support functional recovery after stroke through the development of Hand-TaPS (Task Practice after Stroke), an instrument to evaluate dynamic hand orthoses in home therapy.
METHODS:
Dynamic hand orthosis subject matter experts (
RESULTS:
Four themes (5/20 items) appraised highly relevant for Hand-TaPS. The remaining eight themes (15/20 items) were deemed in need of modification.
CONCLUSIONS:
Dynamic hand orthoses constitute a special case of AT; the assistance they provide targets therapy, not ADLs. Our work to develop Hand-TaPS provides a clear example of the theoretical difference between rehabilitative and assistive technology and underscores the importance of consideration of how a device is used in its assessment.
Background
Rehabilitation of the hand after stroke
Optimizing an individual’s rehabilitation after stroke by integrating therapy into daily life has been the goal of a wide array of home-based technologies [1]. Of the 15 principles of neurorehabilitation operationalized in therapies to promote functional recovery after stroke [2], fully two-thirds describe a strategy of practice. In post-stroke rehabilitation of the hand, unassisted task practice is effective in individuals with mild impairment who have some degree of finger extension ability [3, 4], however moderately to severely impaired individuals find task practice frustrating and fatiguing [5]. This negative experience impedes adherence to a home practice regimen working the hand and reduces the benefit that an individual might gain from consistent and sustained exercise.
To reduce patient burden and corresponding disincentive, the conventional clinical response has been to limit practice to tasks that can be achieved using compensation, i.e. “work arounds.” This approach focuses on developing strategies to replace versus regain hand function lost through stroke and risks confounding goals of actual recovery of function [6]. Dynamic hand exoskeleton technologies, both passive mechanical and robotic, provide proper, biomechanical alignment. Through titration of forces applied to the hand in a personalized manner, hand exoskeleton orthoses provide individuals the assistance needed to complete movements, and practice tasks, that would otherwise be impossible carry out at any given milestone of recovery after stroke. A recent Cochrane review of electromechanically assisted, upper extremity training after stroke rated the evidence for effectiveness as high [7], an affirmation that supports increasing the ability of people with stroke to leverage hand exoskeleton orthoses in their recovery-focused practice at home.
Need for subjective assessment
Beyond the fundamental demonstration of the effectiveness of dynamic hand orthoses, use factors also need to be considered in the technology’s current implementation as well as in the design and evolution of next-generation systems. An accurate mapping of user needs to the functionalities a technology delivers, and the ability to measure user satisfaction with technology once placed in use, are crucial to the support of therapeutic outcomes, as well as to the progressive improvement of rehabilitation technologies [8, 9]. Given the rapidly evolving landscape of dynamic hand orthoses [10], little is known of factors impacting their use in both clinical and home contexts and across disability domains. Further, the additional functionality (gamification features, for example) available in robot-supported hand orthoses increases the challenge of measuring the relation between device characteristics and the needs of individual users. A systematic review (SR) of subjective measures used to evaluate explicitly robotic assistive or rehabilitative technology (A/RT) found that none of the 31 studies examined used an instrument specifically tailored to robotics and only eight studies used any instrument whose validity and reliability had been assessed [11].
This finding led to the development of the PYTHEIA, an instrument designed to capture subjective, user-reported outcomes for specifically robotic AR/T [12]. The PYTHEIA explicitly sites itself [11, 12, 13] in the line of inheritance of two valid and reliable, pre-robotic era assistive technology (AT) assessments that have been widely used: the QUEST 2.0 [14, 15, 16] and the Assistive Technology Device Predisposition Assessment (ATDPA) Device Form [17]. Though demonstrated to be a valid and reliable [12, 13] instrument in its original, Greek-language version, the PYTHEIA has not yet been tested with English-speaking users nor in the specific contexts of dynamic hand orthoses, stroke, or home-based rehabilitative practice.
Objective
Our long-term objective is to support functional recovery after stroke through the development of Hand-TaPS (Task Practice after Stroke), an instrument to evaluate the subjective experience of dynamic hand orthoses as they function to facilitate therapeutic task practice in the home. Here, we report the initial, Conceptual Phase of instrument development.
Methods
Since the PYTHEIA both builds on the legacy of well-used technology assessment instruments as well as incorporates the flexibility to parse the complex functionality that increasingly characterizes robotic AR/T, it served as the point of departure for the design of Hand-TaPs.
Hand-TaPS development process.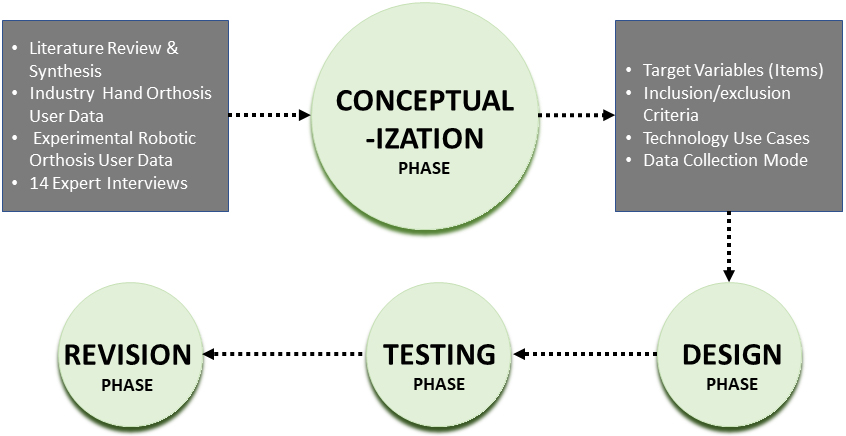
The Usability, Social acceptance, User experience, and Societal impact – USUS Framework (Adapted from Weiss et al., 2009).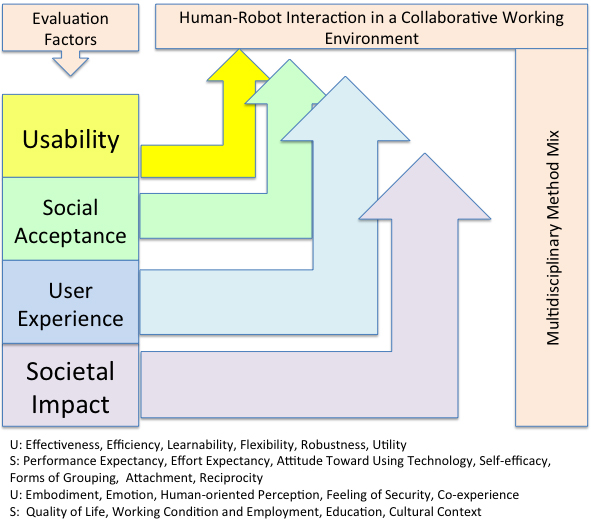
The current project incorporates the systematic procedures [18] used to develop the PYTHEIA. These procedures encompass four main stages: Conceptualization (focus of this paper), Design, Testing, and Revision (see Fig. 1). Gathering and analyzing expert feedback on the face validity of PYTHEIA items in the context of dynamic home hand orthotics was the specific goal of conceptualization activities.
The study was approved by the MedStar Health Institutional Review Board.
Participants
We identified a range of subject matter experts whose combined experience of dynamic hand orthoses provided insights from the perspectives of stroke patients/ consumers and their family members, clinicians, engineers, and commercial product support professionals. Though we ultimately seek to identify use factors for specifically robotic hand orthoses as the rising trend in technological development, we also recruited persons with experience using passive mechanical devices, across experimental (research), clinical, and home-based contexts. Passive hand orthoses, actuated by springs or elastic bands, are similar in appearance to robotic ones, perform similar basic functions, but are much more widely distributed than are next-generation, robot-controlled devices that leverage motors, pneumatics, or hydraulics for actuation. These latter systems are currently used in the home only in research contexts, hence users with experience of them are limited.
Participating experts included: two hand robotics research engineers; two occupational therapists, one with research as well as clinical experience of hand exoskeletons, passive and robotic; two consumer advocates, individuals employed by commercial device providers who support clients (both clinicians and individuals/ families with stroke) selecting, learning, and using devices; five individuals with stroke whose pooled experience included passive and robotic, as well as research and commercial, products; and three family members supporting individuals using hand exoskeletons at home after stroke. All informants were located on the Eastern Seaboard of the United States. The clinical providers from whom consumer participants received their rehabilitation services ranged from local community, generalist occupational therapists to certified neurorehabilitation specialists affiliated with major regional rehabilitation centers.
Procedure
We conducted and audio-recorded, in-depth, semi-structured interviews, 60–90 minutes in length, with 14 individuals either in person or by phone. Participants received a thank-you stipend in appreciation of their time and expertise.
Interactions were structured by an interview guide composed of two segments. The first segment elicited spontaneous narratives of individuals’ experience of stroke and hand orthosis-based therapy in the home or in a simulated home setting in the case of one robotic technology still in the earlier phases of research. The second segment guided participants through the items of PYTHEIA instrument, as published in English by its authors (Table 1). We asked participants to reflect on how each item aligned with their personal experience of dynamic hand orthosis use to explore points of convergence and divergence.
Original PYTHEIA items
Original PYTHEIA items
PYTHEIA item scale format
The distinction between task practice and functional ADL.
The PYTHEIA itself is structured in two parts (Table 2). Part A presents 15 items focused on individuals’ overall experience of a robotic A/RT. As is true of the QUEST 2.0 and the ATDPA, the core experiential constructs emerging from confirmatory factor analysis of the PYTHEIA, Fit to Use and Ease of Use, are consonant with Davis earlier foundational work on technology acceptance [19], a concept itself grounded in the theory of reasoned action [20]. The Fit to Use and Ease of Use consonant with the more recent USUS framework (Fig. 1) proposed for the evaluation of human-robot interaction [21]. Similar to the design of foundational AT instruments, PYTHEIA Part A items are in the format of Likert items (5-point, with an N/A option) measuring either satisfaction of temporality (see Table 2).
Part B of the PYTHEIA facilitates adaptation of the assessment to heterogeneous technologies through an additional five items (four reiterated from Part A and a fifth focused on reliability) that drill down on the individual functionalities of a system. Part B provides the flexibility to evaluate user satisfaction (see Table 2) with as many functionalities as deemed appropriate to the technology under assessment. Prior to exploration of Part B items, interviewees provided their perceptions of the important individual functionalities in the dynamic hand orthoses with which they had experience.
The interview guide was updated after each interaction to reflect new information received from each participant and carried forward to subsequent interviewees.
Key points of participant feedback on PYTHEIA robotic A/RT evaluation themes
Audio files were imported to NVivo12 for transcription, iterative annotation and memo creation, and coding. We used an Interpretative Phenomenological Analytic [22] approach wherein the narrative of each expert was evaluated as a discrete unit and then connections across cases subsequently made. The thematic structure of the interview guide (reflecting the themes of the PYTHEIA) served as initial codes. Novel themes introduced by participants but not reflected in the PYTHEIA were also captured.
Results
Table 3 shows the themes embodied in the items of the original PYTHEIA, their associated item numbers, the convergent validity of each item (i.e. Pearson’s
Secure, confident, protected
The item 10/IF5 dyad of the PYTHEIA maps to the fit-to-use construct and deals with how secure, in the sense of being confident and protected, the device user feels when using the device. Item 10 is measured on the temporal scale, whereas IF5 is measured on the satisfaction scale. From the perspectives of clinicians, engineers, and patient advocates, this item pair represented an important factor in dynamic hand orthosis acceptance. Conversely, persons with stroke downplayed its meaningfulness. However, the theme of insecurity, lack of confidence in the home therapy context did emerge in consumers’ narratives of issues that also dealt with device reliability (item IF4), ease of donning and setup (item 5, ease of use), and pain (not directly mapping to any item, but most relevant, in consumers’ opinion, to item 6, safety/security).
Social comfort: Three levels
Three items measure with how comfortable individuals feel using a device around others: 13, out in the community (encompassing strangers); 14, around colleagues (work environment), and 15, in the company of family and friends. Informants diverged in their feedback about how relevant social comfort was to dynamic hand orthosis use. Devices, given their exoskeleton configuration, are not concealed by clothing and open to view by others. Consumers denied, while professionals endorsed, the items’ relevance. Several consumers described a cultivated indifference to how other people perceived their impairments. Two framed their impairments as opportunities to teach able-bodied individuals about living with disability. All interviewees, however, perceived comfort around friends and comfort around family, combined in Item 15, to be distinct situations.
Sufficiency of functionalities
Item 9 measures the sufficiency of a technology’s existing functionalities. It was deemed relevant to dynamic hand orthosis evaluation by all participants, but in need of further exploration. Participants’ responses pointed to conceptual overlap between item 9, functionality sufficiency and items 3 and 4, which deal with the learnability of device functions, as well as item 5, which assesses device complexity and was universally endorsed by participants as highly relevant to dynamic hand orthosis use. Putting on (donning) the orthosis quickly and correctly was universally identified as fundamental to satisfactory use, with different devices offering different functionalities to accommodate coaxing a hemiparetic hand into the orthosis. Clinicians and one caregiver noted that because every stroke survivor’s impairment is unique, functionality has to be learned in adaptation to the individual, making the process of distinguishing between sufficiency of learnability less clear.
Adaptability to everyday environments
Participants were not able to link their experience with dynamic hand orthoses to a need for the devices to adapt to everyday environments (item 1). In framing his response, one consumer conflated the concept of adaptation with that of compensation. The latter term, as noted in the introduction, refers to a “work around” approach to therapy that is, in fact, the opposite of the recovery-oriented goal of task repetition aided by a hand exoskeleton. The notion of portability, however, was deemed important since it was common practice to take one’s orthosis with one to clinic appointments for supervised practice and professional adjustments.
Improvements to everyday life
Items 2 and IF2 measure device-mediated improvements to everyday life. Consumers initially interpreted this item in one of two ways. Either they focused on the extent to which their orthoses had mediated functional recovery and thereby improved their everyday lives, or (more commonly) they considered how they had (or might) use their dynamic hand orthosis to carry out activities of daily living (ADLs).
Clinicians and commercial product placement professional recognized the consumer expectation that a device might help with ADLs versus therapy as a threat to consumer satisfaction with the device. Robotics engineers further affirmed that it was the prospect of return of function for ADLs that captured their research subjects’ enthusiasm most about dynamic hand orthoses.
Learnability
Items 3 and 4 refer to the learnability of both basic and lesser-used exoskeleton functions. Participants had difficulty identifying what constituted a functionality of the devices with which they had experience, a prerequisite for evaluating how easy it is to learn to use a functionality. As happened during consideration of how the dynamic hand orthosis they used improved their everyday lives, participants had difficulty assessing this item and again lapsed into conflating assistance in training with assistance in ADLs. Persons whose experience was with passive mechanical versus robotic hand orthoses were at a greater loss in identifying functionalities than were those responding for robotic devices, which typically provided a function menu. In the case of passive devices, only across several interviews were the functionality groups of donning, doffing, tensioning, opening, and closing identified. Once functionality was identified, ease of learning was endorsed as relevant.
Autonomy
Item 11 deals with the feeling of autonomy one has using a device and item 12, with needing help from another person. Participants did not interpret the items consistently. One interpretation framed autonomy and needing help as opposites. The other understood personal control as being central to autonomy and that personal control might include enlisting the services of another in carrying out one’s tasks. As in previous items, the perceived purpose of a dynamic hand orthosis, carrying out therapy versus performing ADLs, influenced participants’ assessment of the relevance of autonomy/needing help in evaluating the technology.
Security (satisfaction scale)
Items 6 and IF3, similar to the item 10/IF5 dyad, measure the user experience of the security of a device. Absent the qualifiers, “protected” and “confident” that amplify items 10 and IF5, participants focused on security in the sense of threat of injury in considering items 6/IF3. Small size was the principal reason given for denying the relevance of this item. Despite its unusual appearance, no informant thought security or safety was at all an issue with the dynamic hand exoskeleton orthosis. Robotics research engineers identified safety assurance as a fundamental design requirement but could not remember a subject who had shared a concern for safety with them. Pain opening one’s hand to don the orthosis and in the act of task practice mediated by the device was cited by participants with stroke as a barrier to device acceptance, no one linked avoidance of pain and security.
Discussion
Information provided by our cohort of consumer, clinician, technical, and commercial experts in dynamic hand exoskeleton orthoses will shape the items composing the initial Hand-TaPS as we move to the next phase of observational and cognitive testing. The PYTHEIA refined pre-robotic instruments to accommodate the increased complexity of robotic over pre-robotic technologies generally. Hand-TaPS builds off the foundation of the PYTHEIA, adapting it to optimize selection of increasingly complex technologies, both robotic and mechanical, to support functional recovery of the hand after stroke. Similar adaptations have taken place as subjective measurement of A/RT technologies has increasingly expanded. For example, in the case of the Psychosocial Impact of Assistive Devices Scale (PIADS) [23], adaptations to specific populations, such as children, and specific domains, such as continence, in addition to numerous language translations and cultural adaptations, now constitute an assessment portfolio. (
Assistance versus therapy
The central issue brought to light through participants’ reflection across multiple PYTHEIA items (Social Comfort, 13–15; Sufficiency of Functionalities, 9; Adaptability to Everyday Environments, 1; Improvements to Everyday Life, 2, IF2; Autonomy, 11) was the lack of clarity that exists in device users’ thinking about the distinction between therapeutic and potentially assistive (ADL) functions of dynamic hand orthoses. Both of these uses are well-defined on the technology develop roadmap [10], but need to be evaluated separately for the evaluation to be meaningful.
Our findings here recall the International Classification of Function (ICF) model developed Cowan et al. [24] that distinguishes direct versus indirect AT. A technology used to further rehabilitation is indirectly assistive. It assists with therapeutic task performance that, in turn, facilitates functional gains that enable better performance of ADLs. Direct AT is technology that restores function by compensating disability, and directly enabling ADLs.
All the items listed in paragraph 1 of this section have an underlying valence suggesting interpretation in the domain of direct assistance to promote ADLs versus indirect assistance as a tool for therapy to effect an improved outcome. If carried forward to the Hand-TaPS, these items will need to be worded such that they do not imply assessment for use to support ADLs.
Social comfort
We observed several areas where consumers and professional came to opposite conclusions about an item’s relevance. The area of social comfort (items 13–15) was the most striking disparity in opinion where professionals strongly endorsed and participants with stroke strongly denied the importance of being comfortable using the odd-looking device a hand exoskeleton orthosis is around different categories of people in one’s life.
The social comfort items set is an artifact the PYTHEIA carries forward from earlier valid and reliable measure of specifically assistive technology, the QUEST 2.0 [14, 15, 16] and the ATDPA [8, 9]. These items, further, evidenced some of the highest correlations with total score in the PYTHEIA validation study [12]. We note again that a hand orthosis whose purpose is to facilitate task practice at home is not meant to become part of an individual’s all-day routine; it’s not a device like a cane or wheelchair that a person with stroke uses continually as s/he goes about daily life. Further, hand orthoses are small and, as noted by several interviewees with stroke, no more likely to flag an individual as being a stroke survivor than hemiparesis itself. Further, anyone who would observe it in use would observe it in a specific and limited context. This limited context of use may have underlain consumers insouciance relative to being observed while using their hand orthoses.
Conversely, our stroke survivor informants were all open and accepting of their impairments. As previously noted, two among them stated they enjoyed opportunities to teach others about what it means to live with stroke. As such, their responses may be atypical and reflect an accepting user bias. The responses of professionals, all endorsing the importance of social comfort to hand orthoses acceptance, may reflect their wider vision, having observed reactions to visually distinctive technologies such as hand exoskeleton orthoses across numerous patients or clients.
This uncertainty argues for clarifying the context of task practice (not ADLs) and retaining the social comfort items for the initial version of Hand-TaPS for cognitive testing. We will also expand the family/friends item to two categories, as participants were unanimous in their estimation that the categories were different.
Secure, confident, protected/safety and security
Another area of disagreement between professionals and consumers was relative to the importance of feeling confident using a dynamic hand orthosis (items 10/IF5) and feeling physically safe using it (items 6/IF3). Consumers denied the importance of the confidence their device might instill in them to carry out their task practice program when asked directly. However, they recounted being despondent when they experienced failures of their systems, frustration that they couldn’t carry through with their program as a result. As noted, these issues became salient in the context of reflection on device reliability (item IF4), ease of use (item 5), and pain interference (a novel theme that emerged). It may be useful to elevate item IF4 to an overall device evaluation item in addition to using it to drill down on individual functionalities.
It is unclear why professionals endorsed the importance of these themes when consumers did not. It is possible that health professional would be uncomfortable negating security, protection, and safety with respect their patients/clients. Perhaps notably, the security/confidence/safety items are a legacy from the ATDPA [25] and QUEST 2.0 [14] instruments. In other work on the validation of the Greek version of a QUEST 2.0 subscale [26], Koumpouros and colleagues have noted the ambiguity inherent in the concepts of safety and security. An approach for testing in the initial version of Hand-TaPS may be to revise the confidence/security/safety items to incorporate the notion of reliability and the impact of pain as a result of device normal use.
Sufficiency of functionalities/learning basic and individual functions
All participants struggled with conceptualizing the functionalities of the devices they used despite their considerable experience with them. Consumers and professionals alike needed scaffolding to articulate device functionalities. It was clear that these items imposed a high cognitive load on participants working to frame their responses. These items are among the least correlated with total item score in the PYTHEIA validation study (see Table 3), perhaps reflecting similar difficulty among the original test cohort.
We will consider addressing the problem in Hand-TaPS by altering the order of PYTHEIA items and presenting the IF items, with individual functionalities of interest pre-defined, first. We would then present the items (3, 4, and 9) that ask respondents to generalize across device as a whole with respect to overall functional sufficiency and ease of learning. This approach might also mitigate the risk that a respondent might focus on a functionality in the undesired ADL versus therapy class. It would also assure that all respondents were evaluating the same functionality enhancing validity.
Adaptability
Despite its relatively high convergent validity (
Improvement to everyday life
Though the interpretation of the improvement-to-everyday-life items (2, IF2) in the context of speculative or “off-label” use in service of ADLs is clearly not desirable, the interpretation that focuses on how effective using one’s dynamic hand orthosis has been in regaining function may in fact be the most appropriate approach to measuring impact on everyday life. The alternative would constrain “everyday life” to the segment of time one spends on task practice and the evaluation would be the degree to which the orthosis facilitated practice, irrespective of realization of the functional improvement that is task practice’s goal. This latter interpretation may be more appropriate to the item asked with respect to each identified individual functionality. The former interpretation, conversely, may be more appropriately asked of the orthosis overall. We will test this split configuration for Hand-TaPS during cognitive testing.
Autonomy and needing help from others
Autonomy is a key concept in the use of assistive technology to facilitate ADLs and in the broader realm of disability philosophy [27]. To evaluate the impact of their dynamic hand orthosis on their autonomy, as in previous examples, individuals need to interpret the concept uniformly. Item 11 (autonomy) needs to make it clear that ADLs are not at issue. Rather, respondents are being asked to evaluation the degree to which their hand orthosis has empowered them to continue therapy at home outside of the clinic. Needing help from another person (for example) to don and doff the orthosis does not impact decisional autonomy, though it may cause individuals to rate the experience of their device lower. Wording elucidating this distinction between items 11 and 12 will be tested in the next phase of development of Hand-TaPS.
Conclusions
The focus of Hand-TaPS is the assessment of patients’/consumers’ subjective experience of dynamic hand orthoses as they assist in home-based task practice to promote functional recovery of the hand after stroke. As such, these dynamic orthoses constitute a special case of assistive technology; the assistance they provide targets therapy, not ADLs, as is the more usual understanding of technology-mediated assistance [24]. Persons with stroke, but also professionals who participated in interviews, frequently blurred this important distinction in use. This observation underscores the need to exercise extreme vigilance in wording Hand-TaPS items unambiguously. Testing in the next phase of instrument development will clarify best practice for wording items to promote uniformity in interpretation.
Our work to develop Hand-TaPS provides a clear example of the theoretical difference between rehabilitative and assistive technology [24] and underscores the importance of consideration of how a device is actually used in its assessment.
Footnotes
Acknowledgments
This work was conducted under grant #90REGE0004, the Rehabilitation Engineering Research Center on Patient-centered, Home-based Technologies to Assess and Treat Motor Impairment in Individuals with Neurologic Injury, from the National Institute on Disability, Independent Living, and Rehabilitation Research.