
Abstract
BACKGROUND:
People with severe/profound intellectual and multiple disabilities often need support for their occupational engagement.
OBJECTIVE:
This study assessed a smartphone-based intervention program to strengthen a functional object manipulation response (i.e., collecting and putting away objects) and possibly improve the mood of five adult participants with severe/profound intellectual disability and visual-motor impairment.
METHODS:
The intervention program, which relied on a smartphone linked to a motion sensor, was implemented according to a nonconcurrent multiple baseline across participants design. During the program phase, every object manipulation response (detected by the motion sensor) caused the smartphone to provide the participants with 9 or 10 s of preferred stimulation. Failure to respond for a preset period of time caused the smartphone to present a verbal encouragement/prompt.
RESULTS:
Data showed that during baseline (prior to the intervention program), the participants’ mean frequency of object manipulation responses per 5-min session was always below three. During the intervention phase, the mean frequency of object manipulation responses varied between about 14.5 and 20.5 per session. Moreover, participants showed mood improvement.
CONCLUSIONS:
These results suggest that a smartphone-based intervention program may promote functional responding and improve mood in people with severe/profound intellectual and multiple disabilities.
Keywords
Introduction
People with severe/profound intellectual disability and visual or visual and motor impairment tend to be passive and detached from their immediate environment, thus failing (a) to engage in beneficial motor activity and (b) to interact with objects [1, 2, 3]. This situation has negative implications for their physical condition and for their social and cognitive development, and also limits their overall stimulation input [4, 5, 6, 7, 8]. To improve this situation, different intervention approaches have been suggested. Those approaches have involved among others (a) increased opportunities of social contact, (b) experience of multisensory rooms, (c) exposure to multi-sensory storytelling, and (d) access to self-regulated stimulation [1, 9, 10, 11].
Ensuring increased opportunities of social contact requires a relatively extended involvement of staff, family members and others in interacting with the person with disabilities and trying to facilitate/promote the person’s active engagement [2, 11, 12, 13]. The use of multi-sensory rooms consists of introducing the person to multiple stimulation sources designed to engage the person’s senses and offer the person a feeling of well-being and pleasure [14, 15, 16]. Adopting multi-sensory storytelling exposes the person to the narration of simple stories interspersed with the presentation of the stimuli characterizing the stories [10, 17, 18]. Promoting self-regulated stimulation involves the use of a technology system that allows the person to access preferred environmental stimulation independently (i.e., through the performance of simple responses available in the person’s repertoire) [19, 20, 21].
While all these approaches have shown to be valuable for improving the situation of people with intellectual and multiple disabilities, some considerations about them may need to be made. For example, the use of increased social contact and multi-sensory storytelling, which privileges the human aspect in the stimulation process (i.e., with direct involvement of personnel), would be relatively expensive in terms of staff and/or family time and thus not always feasible. Multi-sensory rooms may be rather expensive to arrange and thus may not be affordable in a number of daily care settings or in home contexts. A self-regulated stimulation approach may be viewed as relatively practical and inexpensive in terms of staff or family time and also rather affordable in terms of the technology required [1, 9, 21, 22, 23]. Moreover, this approach is the only one that is explicitly focused on (a) developing the participant’s responding as a means for controlling environmental stimulation and thus (b) building independence and self-determination for stimulation access.
Recent studies aimed at helping people with intellectual and multiple disabilities manage self-regulated stimulation have adopted new, fairly advanced and easily accessible smartphone-based technology solutions instead of conventional solutions relying on the use of microswitches linked to specific control systems or computers [1, 20]. The participants’ response that these recent studies targeted as a means to access environmental stimulation consisted of pushing a panel in front of the smartphone. This response led to the activation of the smartphone’s proximity sensor and in turn to the smartphone delivering a brief period of preferred stimulation. The results were largely positive with the participants showing an increase in their responding (i.e., panel pushing) and an improvement in their mood (i.e., in their indices of happiness).
Notwithstanding the positive results obtained, one could argue that a more elaborate and advanced response (e.g., collecting and putting away objects) would be fitting and advantageous for participants whose overall level of motor impairment does not preclude such a response [24, 25]. Indeed, collecting and putting away objects would represent a recognized functional activity as well as a mild form of physical exercise (each of which may be viewed as a relevant target within a rehabilitation and care context [9, 19, 23, 24]). For these participants, for example, objects of different shape and/or dimension and weight could be made available in a specific area of the table at which they sit, and their response could consist of putting away those objects (e.g., transferring those objects from that specific area into a near container). The technology required for monitoring such a functional object manipulation response and enabling the delivery of stimulation contingent on its occurrence may consist of a smartphone linked via Bluetooth to a motion sensor placed inside the container and detecting response occurrences.
This study assessed the possibility of fostering the aforementioned response with a smartphone and motion sensor technology setup, which was designed to provide brief periods of preferred stimulation contingent on the response occurrences and verbal encouragements/prompts in case of no responding. The study also determined whether the use of such a technology setup would have a positive impact on the participants’ mood (i.e., would increase their indices of happiness) [20, 23]. Five participants were involved in the study.
Participants’ pseudonyms, chronological age, visual and motor conditions, and Vineland age equivalents for daily living skills (personal sub-domain)
Participants’ pseudonyms, chronological age, visual and motor conditions, and Vineland age equivalents for daily living skills (personal sub-domain)
Participants
Six participants were initially recruited, but one was withdrawn shortly after the beginning of the study due to health and related behavioral problems (i.e., seizures and unresponsiveness). The participants, who represented a convenience sample, were recruited on the basis of the following criteria. First, they were largely passive and detached with virtually no contact with objects or other material surrounding them without staff supervision. Second, they were capable of manipulating objects (e.g., taking objects from a certain space in their reach and putting those objects away). Third, they showed positive behavioral reactions (e.g., orienting and smiling) toward environmental stimuli, such as songs, music pieces, chimes, and excited familiar voices. Thus, it was assumed that they would enjoy being involved in an intervention program allowing them access to those stimuli. Fourth, they tended to react to verbal encouragements/prompts (e.g., by resuming a previously interrupted response engagement). Fifth, staff supported this study (i.e., its aims and the technology involved), which had been presented to them in advance. Their support was motivated by the fact that the study was aimed at promoting the participants’ positive response engagement, at increasing their stimulation access, and at fostering response initiative and self-determination.
Table 1 lists the five participants who completed the study by their pseudonyms, and reports their chronological age, their visual and motor condition, and their age equivalents for daily living skills on the second edition of the Vineland Adaptive Behavior Scales [26, 27]. The participants’ chronological age ranged between 23 and 44 years. Three participants (i.e., Ian, Lucy and Avery) had minimal residual vision, that is, they were able to see objects/obstacles in their immediate proximity. The other two (i.e., Abel and Grace) were totally blind. Two of them were able to walk without support (Abel and Avery). Two could briefly walk with staff’s physical support (Ian and Grace). The fifth participant (Lucy) was nonambulatory and required the use of a wheelchair. Their Vineland age equivalents for daily living skills (personal sub-domain) ranged between 1 year and 2 months (Lucy) and 2 years and 4 months (Avery). All participants attended rehabilitation and care centers. The psychological services of those centers estimated the participants’ level of intellectual disability to be within the severe to profound range, but no formal testing had been carried out with them given their conditions.
While it was assumed that the participants might find their involvement in the study an enjoyable experience due to the possibility of accessing preferred stimuli (see below), there was no direct way to determine their assent to the study. Therefore, their legal representatives were asked to sign a consent form allowing such an involvement prior to the beginning of the study. The study complied with the 1964 Helsinki Declaration and its later amendments and was approved by an institutional ethics committee.
Setting, sessions, stimuli, and research assistants
A quiet room of the centers that the participants attended was used as setting for the study (i.e., for baseline, intervention, and control sessions). Baseline and intervention sessions lasted 5 min and were typically carried out two to four times a day, 3 to 6 days a week. During those sessions, the participants were sitting at a desk and had objects in front of them. The objects were in a tray or box. Next to this tray or box, there was a special wooden container where the objects were eventually to be placed. Control sessions, which also lasted 5 min, were carried out immediately before the beginning of intervention sessions (i.e., so as to attain a series of control-intervention session pairs; see below).
The stimuli used contingent on each object successfully transferred to the wooden container during the intervention sessions involved music and songs, chimes, and excited voices. Those stimuli, which had been recommended by staff, were selected for the study after a stimulus preference screening. The screening process involved at least 10 non-consecutive presentations of two or three 10-s segments of each of the songs, music pieces, chimes, and voices included in the screening. A stimulus was retained for the study if a research assistant and a staff member involved in the screening agreed that such stimulus produced positive participant’s reactions (e.g., alerting, orienting, smiles, or excited movements) in at least 50% of the segment presentations. Research assistants, who were responsible for implementing the sessions and recording part of the data (see below), were familiar with the use of technology-aided interventions with people with intellectual and multiple disabilities as well as with data collection procedures.
Technology system
The main component of the technology system used for the intervention program was a Samsung Galaxy A22 with Android 11 operating system, which was (a) equipped with Amazon Alexa, MacroDroid, and Philips Hue applications, and (b) supplied with a series of audio files concerning the participants’ preferred stimuli and one- or two-word verbal encouragements/prompts. The technology system also involved (a) a Philips Hue indoor motion sensor, (b) a Philips Hue Bridge and Philips Hue smart bulb working via Bluetooth, (c) a 4G Long-Term Evolution Wi-Fi router, and (d) a Bluetooth mini speaker. The Philips Hue Bridge, smart bulb, and application, and the router served to enable the functioning of the Philips Hue sensor. The Amazon Alexa and MacroDroid applications were set up to ensure an interaction between the smartphone and the sensor (see below). The MacroDroid application, moreover, served to record the sessions’ data through the system log, which provided a detailed history of the sessions.
The sensor was a box-like device with a 5.5-cm side and 3.5-cm height and was located inside a wooden container, into which the participant was to transfer series/groups of objects. The objects were displayed in a tray or box in front of the participant and the container was to the side or behind the tray/box. As soon as the participant placed an object in the container the sensor was activated. Sensor activation was identified via the Amazon Alexa application and transmitted to the smartphone via MacroDroid. Following each sensor activation (i.e., response), the smartphone provided 9 or 10 s of preferred stimulation (e.g., of a preferred song or chime). If no sensor activation occurred for 20–25 s (i.e., the participant had not produced a new response for 20–25 s), the smartphone provided a verbal encouragement/prompt, which could be repeated (see below). Preferred stimulation and encouragements/prompts were delivered via the mini speaker.
Measures and data recording
The measures recorded were: (a) the number of functional object manipulation responses (i.e., the number of objects the participants took from the tray/box and placed in the wooden container), (b) the number of smartphone’s encouragement/prompt instances, (c) the number of research assistant’s guidance instances, and (d) the indices of happiness (i.e., smiles, vocalizations, or excited hand or head movements [1, 28]). The first three measures were automatically recorded via the smartphone. In fact, the smartphone logged via the MacroDroid (a) the number of sensor activations (i.e., the number of objects transferred into the container), (b) the times of those activations and thus whether the responses producing the activations occurred independently or following research assistant’s guidance (see Sections 2.5.1. and 2.5.2.) and (c) the instances in which smartphone’s encouragements/prompts were emitted.
The research assistants recorded the participants’ indices of happiness using a partial interval recording system, in which 10-s observation intervals were followed by 5-s scoring periods [1, 28]. A positive score indicated the presence of one or more indices of happiness during the observation interval regardless of how long they lasted. A negative score indicated the absence of those indices. Indices of happiness were recorded for each participant during 30 intervention sessions and as many control sessions (see Sections 2.5.2. and 2.5.3.). Interrater agreement on indices of happiness was assessed in more than 30% of the sessions with a reliability observer joining the research assistant in data recording. The percentage of agreement (computed for the single sessions by dividing the intervals with the same “positive” or “negative” score from the research assistant and reliability observer by the total number of intervals and multiplying by 100%) ranged between 80 and 100%, with means exceeding 92% for all participants.
Experimental conditions and data analysis
The intervention program was introduced according to a nonconcurrent multiple baseline design across participants [29, 30]. Based on the design requirements, the participants received different numbers (i.e., between 5 and 12) of baseline sessions. The baseline sessions were followed by 95 to 119 intervention sessions. Thirty intervention sessions were preceded by (paired with) control sessions. Those 30 control-intervention session pairs served to record and compare the participants’ indices of happiness in the two session conditions. To ensure procedural fidelity [31], a study coordinator with access to video recordings of the sessions provided the research assistants with regular feedback on their performance.
The participants’ data for object manipulation responses (i.e., during baseline and intervention sessions) and indices of happiness (during intervention and control session pairs) are reported in graphic form. In order to simplify the graphic display, the data are summarized in blocks of sessions (see Section 3.). Consequently, the data points graphed for object manipulation responses represent mean frequencies per session and the data points graphed for indices of happiness represent mean percentages per session. To analyze the differences (a) between baseline and intervention data on object manipulation responses, and (b) between intervention and control data on indices of happiness, the “Percentage of nonoverlapping data (PND)” method [32] was used for each of the participants separately. Specifically, for each participant it was determined the percentage of intervention data points that exceeded the highest baseline data point [32].
Baseline sessions
During the baseline sessions, the participants sat at a desk and had (a) a combination of objects (e.g., pegs, glasses, and rolls) in a tray/box in front of them, and (b) a special wooden container which was located to the right or left of the tray/box or behind the tray/box, depending upon the response scheme that suited the participants best. Prior to the start of the session, the research assistant provided the participants with verbal and physical guidance for carrying out an object manipulation response, that is for taking an object from the tray/box in front of them and placing the object in the wooden container. The technology system was available, but served only to record the responses without providing stimulation or encouragements/prompts. During the session, the research assistant guided the participants verbally and physically to perform a response if they failed to do so independently for 40 s. At the end of the session, the responses the participant performed with research assistant’s verbal and physical guidance (i.e., logged in the smartphone’s system at intervals of 40 s from any previous response) were subtracted from the total number of responses recorded by the smartphone, so that only the independent responses would be counted and reported.
Intervention sessions
Intervention sessions were directed at the implementation of the intervention program. The participants sat at the desk with a combination of objects and a wooden container as in baseline, but the technology system worked as described in the Technology System section. Specifically, every object manipulation response (i.e., every object placed in the container) was followed by 9 or 10 s of preferred stimulation, and failure to respond for 20–25 s led to the automatic presentation of a smartphone’s encouragement/prompt. The encouragement/prompt was repeated at intervals of 10 s if the participant failed to respond in relation to its first presentation. Research assistant’s verbal and physical guidance would be added to the second repetition of the smartphone’s encouragement/prompt during the first 10 intervention sessions. Responses performed with research assistant’s guidance were substracted from the total number of responses recorded by the smartphone as during baseline. After the initial 10 sessions, research assistant’s guidance was no longer available. During 30 intervention sessions concentrated in the second half of the intervention phase, the research assistants also recorded the participants’ indices of happiness.
Control sessions
Each of the participants’ 30 intervention sessions used for recording their indices of happiness was immediately preceded by a control session. During the control sessions, the participants were sitting in an unsupervised situation, without any specific activity or set of objects available to them or any specific stimulation directed to them. Recording of their indices of happiness occurred as in the intervention sessions.
The five panels summarize the baseline, intervention, and control sessions’ data for the five participants. The black squares represent mean frequencies of object manipulation responses (i.e., independent of research assistant’s guidance) per session computed over blocks of three sessions during the baseline and five sessions during the intervention. Blocks including a different number of sessions (i.e., at the end of the baseline and intervention phases) are marked by a numeral, which indicates how many sessions are included. The empty and gray circles represent mean percentages of intervals with indices of happiness over blocks of five intervention sessions and blocks of five control sessions, respectively.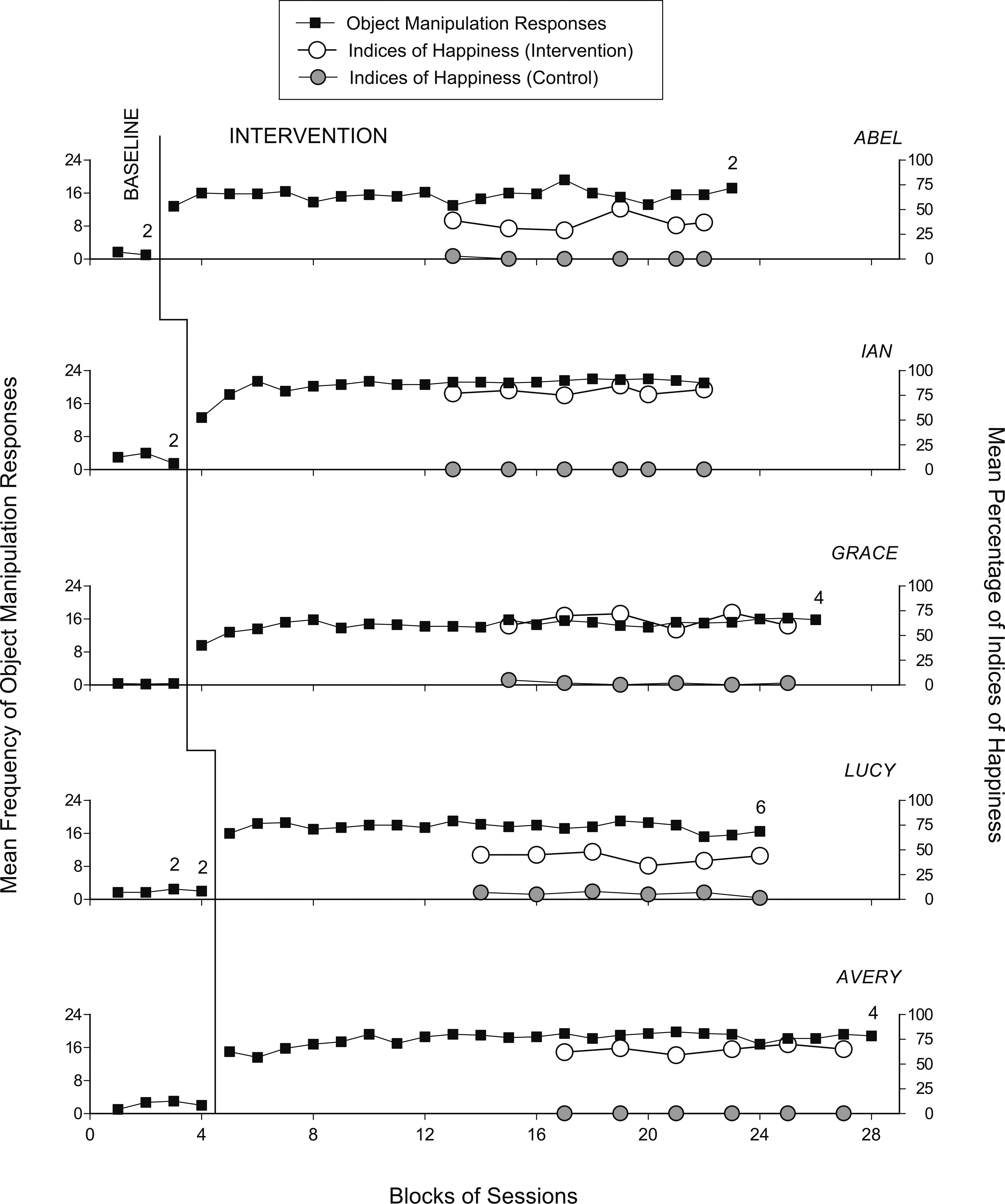
The five panels of Fig. 1 summarize the participants’ data during the baseline, intervention, and control sessions. The black squares represent mean frequencies of functional object manipulation responses (i.e., independent of research assistant’s guidance) per session computed over blocks of three sessions during the baseline and five sessions during the intervention. Blocks including a different number of sessions (i.e., at the end of the baseline and intervention phase) are marked by a numeral indicating how many sessions are included. The empty and gray circles represent mean percentages of intervals with indices of happiness over blocks of five intervention sessions and blocks of five control sessions, respectively.
During the baseline phase, the participants’ mean frequency of object manipulation responses carried out independent of research assistants’ guidance varied between close to zero (Grace) and about 3 (Ian). During the intervention phase, the participants’ mean frequency of object manipulation responses independent of research assistant’s guidance varied from about 14.5 (Grace) to about 20.5 (Ian). Comparisons of the baseline and intervention session data points, using the PND method, showed indices of 1.0 (i.e., 100% of the participants’ intervention data values exceeded their highest baseline data value) confirming a strong effect of the technology-based intervention program. The mean frequency of smartphone’s encouragement/prompt instances (not reported in Fig. 1) varied from about 1 every three sessions (Ian and Avery) to slightly above 1 per session (Abel).
The participants’ mean percentages of intervals with indices of happiness during the intervention sessions varied from 37 (Abel) to 79 (Ian). Their mean percentages during the control sessions varied between zero (Ian and Avery) and 6 (Lucy). Comparisons between the data points of the intervention sessions and those of the control sessions using the PND method showed indices of 1.0 for Ian, Grace, Lucy and Avery (i.e., 100% of their intervention data values exceeded their highest control data value) and 0.93 for Abel (i.e., 28 of his 30 intervention data values were higher than his highest control data value). Both indices (i.e., 1.0 and 0.93) confirm a strong positive effect of the intervention conditions [32].
Discussion
The data suggest that the smartphone-based program used during the intervention phase was effective in promoting the participants’ responding (i.e., their functional object manipulation responses) and improving their mood (i.e., increasing their indices of happiness). These results corroborate previous data concerning the possibility of using technology systems to enable people with intellectual and multiple disabilities to (a) develop and strengthen responding to access preferred environmental stimulation and (b) enjoy such a situation (i.e., the relationship between responding and stimulation) [9, 19, 20, 23]. In light of the results, a few considerations may be in order.
First, the object manipulation responding promoted in this study (i.e., taking objects from a tray/box and placing them in a special container) represents a form of functional occupation for people with severe/profound intellectual or multiple disabilities [33, 34, 35]. Making that occupation successful (as shown by the relatively high frequency of responses) and apparently pleasant/satisfactory (as shown by the indices of happiness) may be viewed as practically relevant. Indeed, helping people to independently (and happily) engage in an easily recognized functional activity would not only enrich their daily life but also facilitate (a) an immediate appreciation of their engagement by staff and caregivers, and (b) an improvement of their social image [36, 37]. The fact that the results were obtained with the use of a technology system based on common commercial components may help rehabilitation and care staff to see those results as a realistic objective for a number of daily contexts [38].
Second, the smartphone-based system used in this study represents an easily accessible tool compared to the systems based on computers or specific control devices linked to microswitches [9, 19, 23]. Nonetheless, it should be noted that the smartphone-based system is not a ready-made (off-the-shelf) tool, but needs to be arranged through the combination of commercial components (including common applications). The cost of the reported system may be estimated at about US $400 (i.e., approximately US $175 for the Samsung smartphone, US $50 for the Philips Hue sensors, US $25 for the mini speaker, and US $150 for the Philips Hue Bridge, the Philips Hue smart bulb, and the 4G Long-Term Evolution Wi-Fi router). This cost cannot be considered irrelevant. Yet, the system offers relevant occupation opportunities (can also be used for different individuals in turns) and is fairly easy to operate for personnel in charge of the sessions and friendly for the participants [39, 40, 41, 42].
Third, while no generalization and maintenance assessment was carried out in this study, one might believe that a positive outcome could be obtained in both areas. In essence, generalization across quiet daily settings might be foreseeable because the technology and procedural (response and stimulation) conditions would remain unchanged irrespective of where the sessions are carried out. Generalization across intervention agents (staff and caregivers) might be facilitated by the fact that (a) those agents have a marginal role and (b) the procedural conditions are directly supervised by the technology system. Maintenance may be a realistic and reachable objective if one ensures that the stimulation available for the participants’ responses is enjoyable and motivating [43, 44]. For this purpose, professionals or caregivers in charge of the sessions should periodically carry out stimulus preference checks and determine the stimuli that should be retained or replaced, and the new stimuli that might be introduced to boost the participants’ interest and motivation [43].
Study limitations and conclusion
Three limitations of the study may be mentioned here. The first limitation is the small number of participants involved in the investigation. Direct and systematic replication studies would be needed to verify the reliability of the present findings and the possibility to develop adapted/upgraded technology versions to reach a wider range of people with special needs [45, 46]. A second limitation concerns the absence of a social validation of the technology system and intervention conditions. Such validation would be considered an essential component of the assessment effort and a critical step to determine the validity of the results obtained and the acceptability and functionality of the approach within daily contexts. The validation could be carried out by showing staff personnel, caregivers, and service providers video clips of the intervention sessions and ask them to rate the content of those clips (i.e., the technology-aided program) in terms of effectiveness, applicability, and likely shortcomings to be corrected [21, 47, 48]. A possible third limitation of the study concerns the fact that research assistants were employed to carry out the study sessions. It might have been practically relevant to (a) involve regular staff personnel (rather than research assistants) in carrying out those sessions and (b) determine how rapidly and easily these personnel could be prepared to perform such task. Given the friendliness of the technology system and the simplicity of the procedural conditions, the expectations would be that regular staff personnel could be ready for carrying out the task reliably after a very brief introduction training [37].
In conclusion, the results suggest that the smartphone-based intervention program evaluated in this study can help people with intellectual disability and visual or visual and motor impairments engage in a functional form of occupation and enjoy such occupation (i.e., with increased indices of happiness). Although these results are encouraging, general statements about the effectiveness and generality of the intervention conditions and the technology system should be postponed until new research has addressed the limitations of this study. Future research may also try to expand the scope of this study with the inclusion of new functional responses and new versions of the technology system.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors report no conflicts of interest.
Ethical considerations
The study was approved by an institutional ethics committee. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The participants’ legal representatives provided written informed consent for the participants’ involvement in the study.