
Abstract
BACKGROUND:
Automated in-vehicle technologies, specifically in-vehicle information systems (IVIS) and advanced driver assistance systems (ADAS), are increasingly common in today’s cars. Previous studies illustrate benefits of using IVIS and ADAS to improve safety, convenience, and comfort in healthy older drivers. However, research is sparse on the feasibility of such technologies for medically at-risk drivers, such as those with Parkinson’s disease (PD).
OBJECTIVE:
This study enrolled healthy volunteer drivers to examine the feasibility of the procedures and measures for evaluating the effects of IVIS and ADAS on their driving performance.
METHODS:
During this feasibility study researchers compared drives completed with and without support of IVIS and ADAS, as participants drove a 2019 Toyota Camry XLE. The test vehicle was equipped with IVIS, ADAS, cameras, a telematics system, and sensors. Participants drove the road course supervised by a Driver Rehabilitation Specialist (DRS).
RESULTS:
Overall study procedures and vehicle equipment were feasible and provided sufficient data collection for measuring the impact of IVIS and ADAS on driving performance. Data observation by the DRS combined with data captured from cameras and telematics, facilitated comparisons to increase data reliability and validity.
CONCLUSIONS:
Feasibility study findings informed a randomized clinical trial, examining the use of IVIS and ADAS technologies as an intervention to support drivers with Parkinson’s disease.
Keywords
Introduction
New car technologies to aid drivers in safety, convenience, and comfort have emerged over the past few decades. In-vehicle Information Systems (IVIS) and Advanced Driver Assistance Systems (ADAS), both representing automated in-vehicle technologies, are installed in approximately 92.7% of new cars since 2018 [1]. IVIS are technologies that provide information (e.g., traffic condition, navigation information, weather conditions, or hazard alerts) to support drivers but do not assume tactical (e.g., lane choice) or operational (e.g., longitudinal or lateral control of the vehicle) functions of the driving task. In contrast, ADAS, such as Adaptive Cruise Control and Lane Steering Assist, offer functionality that incorporates tactical or operational driving tasks during high-risk (e.g., emergency braking) or daily driving (maintaining a safe distance in the flow of traffic) situations.
Drivers with disabilities have shown difficulty with tactical and operational driving tasks during routine driving (e.g., lane maintenance and changing lanes) as well as during high-risk situations (e.g., car ahead suddenly stops or slows) [2, 3]. Specifically, findings from research with drivers who have Parkinson’s disease identify lane maintenance and vehicle position as two driving errors [4, 5] that may be mitigated – in part or whole – by use of IVIS or ADAS. Several IVIS and ADAS studies have focused on drivers with disabilities [6, 7] but on-road studies are limited, especially studies with a clinical focus. Although these technologies have the potential to improve driver safety, comfort, or convenience [8], the procedures and outcomes used to evaluate their impact on driving performance must be established. Researchers must examine the feasibility of the data collection procedures and proposed outcomes before quantifying the effects of such technologies on driving performance. A feasibility study on the effects of IVIS and ADAS on the driving performance of healthy drivers will lay the foundation for an anticipated successful execution of the formal study with a population of drivers with Parkinson’s disease (PD) [9].
Literature review
Feasibility study
Findings from feasibility studies are helpful before planning a randomized controlled trial (RCT) – specifically, to answer the question “Can this study be done?” [10, p. 172]. Feasibility studies focus on the process of developing and implementing interventions, and result in the preliminary examination of participant responses to such interventions [11]. Although the main study must test the hypotheses of intervention effectiveness, hypothesis testing is not appropriate for feasibility studies, given the study purpose and the small sample size [10]. Instead, feasibility studies can answer questions for clinical trial planning surrounding implementation practicality [12]. Such questions are more critical when the planned study is novel and/or complex [13].
Orsmond and Cohn [11] presented objectives and guiding questions for conducting a feasibility study. Their guidelines highlighted five major objectives in assessing the feasibility: (1) assessment of recruitment capability and resulting sample characteristics; (2) evaluation and refinement of data collection measures and procedures to ensure appropriateness for the target population; (3) acceptability of the intervention and data collection methods to indicate if such procedures and methods are suitable for the participants; (4) ability to manage the study, especially determining if the research team has the resources and ability to execute the study; (5) and a preliminary evaluation of participant response to the intervention, for determining if the intervention shows promise of being successful with the target population. Since a feasibility study is a developmental learning process, researchers may adapt the study procedures and intervention to achieve the most promising outcomes. Thus, a well-executed feasibility study is critical to the successful implementation and validity of a planned trial [10].
IVIS and ADAS studies involving on-road exposure
Evidence indicates that researchers have established methods to collect data on IVIS and ADAS during on-road driving studies [14, 15, 16, 17, 18]. In these studies, participants drove routes carefully selected based on traffic density, speed limit, distance, and neighborhood characteristics (e.g., urban, sub-urban, city, or rural). The researchers instrumented the vehicles with sensors, small cameras, and laptop computers, and with data collection software. By comparing vehicle kinematics (e.g., speed, acceleration/deceleration, direction) and video data collected during different driving conditions, researchers quantify the effects of IVIS or ADAS on actual driving performance. Besides observing driving errors (e.g., signaling errors, speeding errors) from the data, researchers can also examine driving behaviors (e.g., glances towards the visual display) and vehicle maneuvers (e.g., the number of lane departure warning activations, the number of lane centering maneuvers) with and without the activation of IVIS or ADAS [14, 16, 17, 18].
Naturalistic studies pose the greatest level of external validity as researchers collect data continuously and inconspicuously with small cameras and sensors to register driver behaviors, vehicle maneuvers, and the influence of external conditions such as obstacles in the road. Such data are generally collected via a data acquisition center, often located in the test vehicle, which may be used for further analysis [18]. For studies involving IVIS or ADAS, researchers may focus on critical events that impact driving performance. For example, a driver may swerve to avoid road debris. Such actions may be misinterpreted in studies where a human observer (e.g., a driver rehabilitation specialist – a trained health professional for evaluating individual’s fitness to drive) or other sensing modality (e.g., video footage) are not available. As such, a human observer and/or other sensory device (e.g., cameras) become paramount to accurately interpret the driver’s performance and the vehicle maneuvers, within a dynamic environment [15, 18].
Types of data collected in IVIS and ADAS studies
In on-road studies [19, 20, 21], researchers can collect subjective measures, e.g., self-reported driving performance, perceptions about IVIS and ADAS systems; but also objective measures, such as average counts for forward-collision warning, average lane departure warnings, speeding errors, lane departure errors, or signaling errors. In addition to capturing vehicle kinematic data (e.g., speed, acceleration/deceleration, direction), video footage is useful to reflect the interaction between the driver, the vehicle, and the on-road environment [15, 18]. Such data collection methods ensure contextual relevance to better examine and quantify the driver’s performance [22].
However, additional enhanced methods, to supplement data collection other than those mentioned (i.e., human observer data, kinematics data, and video data) can be employed. Particularly, to indicate vehicle metrics pertaining to speed, acceleration, and/or sharp turns, researchers employ Freematics OBD-II data loggers, the GreenRoad kinematic-based system, or the Mobileye vision-based In-Vehicle Collision Avoidance Warning System [23, 24]. The usage of sensors embedded in these technologies, allow researchers to collect additional driving performance data in a more accurate way. Sensors enrich the collection of driving performance metrics for IVIS or ADAS which can be challenging, or even impossible, for a human observer to collect with the same level of accuracy [22].
In summary, having human observers log driving errors in real-time and using sensors (e.g., Freematics OBD-II data loggers, the GreenRoad kinematic-based system) to enhance the vehicle kinematics, are well documented in the IVIS and ADAS literature. However, understanding the feasibility of such procedures and measures among healthy and medically at-risk drivers, is not well documented. Thus, this study also examines the strengths and weaknesses of data collected by driver rehabilitation specialists and technology-based measurement techniques (e.g., telemetry).
Occupational therapy/engineering collaborations
The feasibility and fidelity of driving research, especially with automated and/or instrumented vehicles, can be increased by collaboration among engineers and occupational therapy researchers [25]. Ideally a collaboration will start with study design – to plan engineering solutions for optimal data collection [22, 26]. Occupational therapists can adapt the vehicle and road course so drivers, including those with disabilities and/or medically at-risk conditions, are set up for a realistic driving experience. Under these conditions, and via the study process and procedures, researchers can capture valid driving data.
Objectives
Although IVIS and ADAS are available in existing vehicles, we do not know if they will benefit the driving performance of drivers with medically at-risk conditions. Given the documented benefits related to safety and comfort of IVIS and ADAS for older drivers [8], we must examine the feasibility of the procedures (e.g., data collection) and measures (e.g., driving errors), as well as the effects of IVIS and ADAS on healthy drivers, before examining medically-at-risk populations. If a study on healthy drivers confirms the feasibility of IVIS and ADAS data collection procedures and measures, the research team will be more confident to apply such procedures and measures to those who are medically at-risk for driving.
Therefore, the current study examined the feasibility of the experimental procedure and measures that are important in assessing the effects of IVIS and ADAS on the driving performance of healthy volunteer drivers in a test vehicle in traffic. Specifically, we examined the data collection systems and procedures by having healthy volunteers drive a selected road course, with and without, the activation of IVIS and ADAS. Additionally, the research team evaluated how participants performed in relation to driving performance metrics, including speeding, lane maintenance, and signaling. The research team expected this feasibility study to provide fundamental information to pursue continued work in drivers with PD [9].
Blind Spot Monitor, Lane Departure Warning, Adaptive Cruise Control, and Lane Steering Assist. Note. Figure 1 shows (a) indicators of Adaptive Cruise Control (ACC), Lane Departure Warning (LDW), and Lane Steering Assist (LSA) on the multi-information display. By changing the number of horizontal bars in the indicator of Adaptive Cruise Control, drivers specified the headway distance. Lane Departure Warning and Lane Steering Assist shared the same indicator, but signaled with different colors: when the vehicle deviated from the center of the lane, Lane Steering Assist was activated. The indicator turned to green from white. When the vehicle further crossed the edge of the lane (as shown in (b)), Lane Departure Warning was activated. The shared indicator turned to orange from green. If the other vehicle approached in the adjacent lane, the indicator of Blind Spot Monitor flashed on the side mirror (see in (c)).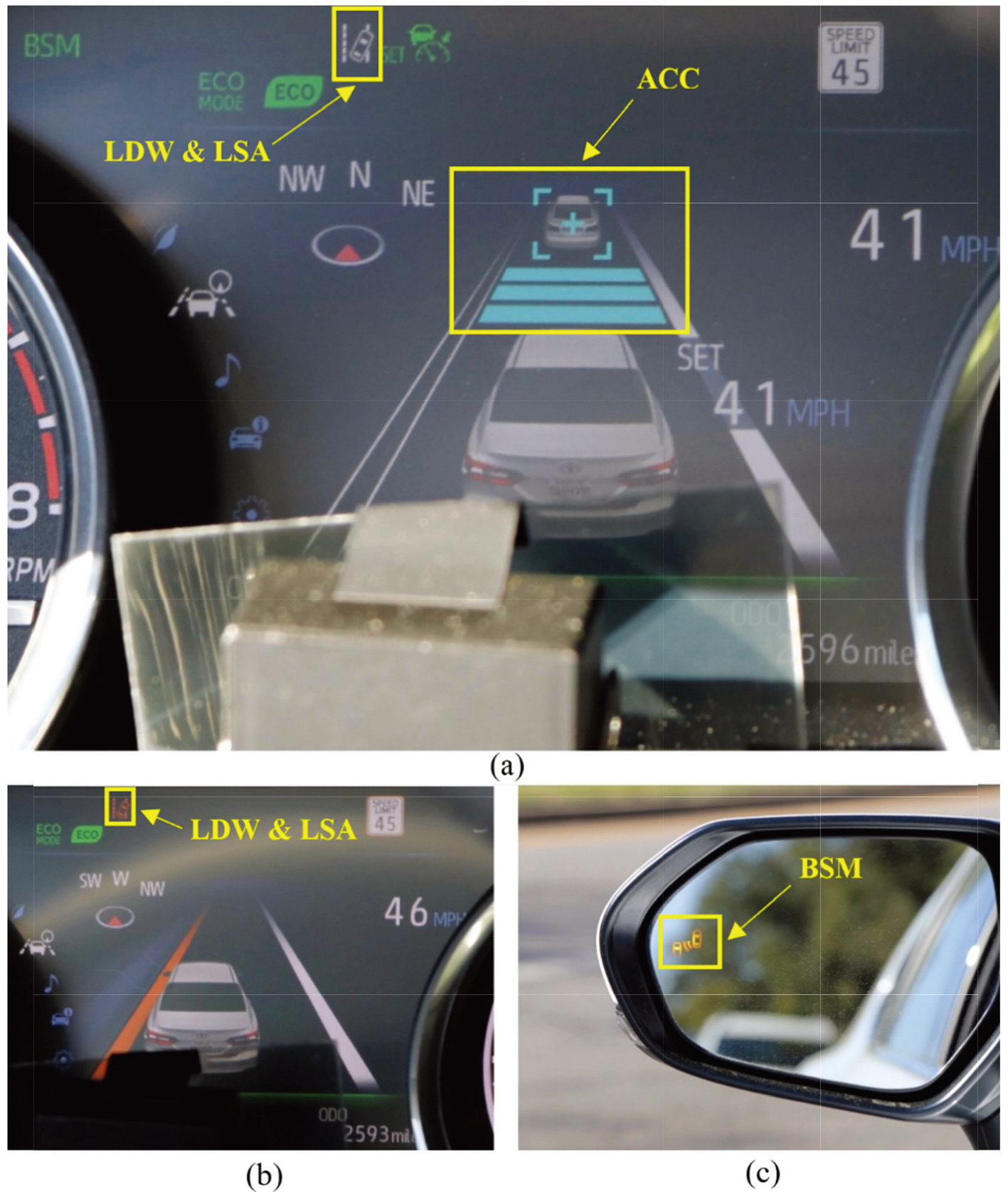
Ethics and IRB approval
This feasibility study was conducted under the affiliation of a randomized controlled trial (RCT) entitled: Driving Performance of People with Parkinson’s using Automated In-Vehicle Technologies. The university issued institutional full review board (IRB) approval (IRB #: 202002321).
Participants
The participants were a convenience sample of healthy (no self-reported medical conditions) volunteers, with valid drivers’ licenses, from the University of Florida network. Two drivers were male and one was female, all between 25 and 35. Each participant provided verbal informed consent prior to the on-road experience.
Materials and apparatus
The test vehicle was a 2019 Toyota Camry XLE outfitted with an auxiliary brake and an eye check mirror. A driver rehabilitation specialist provided route instructions to the driver from the passenger seat, ensured safe vehicle operations, and recorded driving errors. The vehicle was also equipped with an advanced active safety driver assist package. Within this study, researchers specifically examined the IVIS (i.e., Blind Spot Monitor and Lane Departure Warning) and ADAS (i.e., Adaptive Cruise Control and Lane Steering Assist) features (see Fig. 1). For the IVIS features, the Blind Spot Monitor provided a visual warning to alert drivers of vehicles approaching the adjacent lane on the side mirrors. The Lane Departure Warning informed drivers when they drifted out of their lanes without a turn signal via a visual prompt on the multi-information display in the instrument cluster. Among the ADAS features, Adaptive Cruise Control allowed drivers to set the desired cruising speed and a desired following distance from lead vehicles. If a lead vehicle moved slower than the set cruising speed, the Adaptive Cruise Control automatically slowed the test vehicle down to maintain the pre-set following distance, then accelerated again to the original pre-determined speed once the lead vehicle moved out of the way. When the wheel(s) crossed over the lane line(s), the Lane Steering Assist was activated and then automatically steered to keep the vehicle in its lane.
The research team adopted a low-cost solution that used the car’s built-in IVIS and ADAS sensors and algorithms, off-the-shelf cameras and telemetry kit, and data processing algorithms to further instrument the vehicle. The research team installed two GoPro Hero 7 Silver cameras, three USB cameras (two ELP wide-angle cameras recording at 720p resolution, one Logitech C922 webcam recording at 1080p resolution), and one Garmin 55W dash-camera to collect video data. Video data were used in conjunction with the data collected by the driver rehabilitation specialist (see Fig. 2a–d). Specifically, two GoPro cameras were mounted on the outside of the driver side and passenger side windows. By pointing at the side mirrors, the GoPro video captured the activation of the Blind Spot Monitor when a vehicle in the adjacent lane approached. Inside the vehicle, one ELP camera pointed at the multi-information display (the multi-information display recorded the activation of Lane Departure Warning, Lane Steering Assist, and Adaptive Cruise Control). For reducing glare, a polarizing film was applied to the camera. The other ELP camera was placed beneath the driver’s seat to record driver behaviors related to acceleration and braking. The Logitech webcam, mounted behind the front passenger seat, pointed at the steering wheel. This camera recorded the driver’s steering behaviors. The Garmin dash camera, mounted on the upper middle of the windshield, recorded the forward driving scene. Video data of the in-vehicle sources was combined into a single video stream using the free, open-source web-camera recording software Open Broadcasting Software (OBS). Along with the cameras, the research team utilized a Freematics ONE
Cameras and Freematics (KIT-4) Vehicle Telemetry Starter Kit used in the study. Note. Figure 2 shows (a) a GoPro Hero 7 Silver camera capturing the activation of the Blind Spot Monitor, (b) an Axis PTZ camera mounted at the multi-information display, (c) a Logitech webcam recording drivers’ steering behaviors, (d) a Garmin 55W dash-camera recording the forward driving scene, and (e) a Freematics (KIT-4) Vehicle Telemetry Starter Kit collecting kinematic data of the vehicle.
In this feasibility study the driving condition was the independent variable. Participants experienced two driving conditions: one with the IVIS and ADAS activated, and another with the IVIS and ADAS deactivated. Specifically, while the IVIS and ADAS were active, the Blind Spot Monitor, Lane Departure Warning, and Lane Steering Assist were used throughout one half of the drive. When traveling on the highway for half the drive, the adaptive cruise control was utilized.
Dependent variable measurement comparison
Dependent variable measurement comparison
Table 1 summarizes the dependent measures used in the study, and the sources of data for each variable. Driving errors were recorded by the driver rehabilitation specialist, specifically the number of speeding (under or over) errors, lane maintenance (wide or encroach) errors, and signaling errors. Specifically, the driver rehabilitation specialist logged driving errors as count data on a standardized error sheet during the on-road drive. Speeding errors had two categories, over-speeding and under-speeding. If the driver was traveling 5 mph above or below the posted speed, an error was marked. Likewise, lane maintenance errors were classified as encroaching or wide. During straight driving, wide referred to the situation when the vehicle crossed over the lane marking towards the road shoulder, while encroaching took place when the vehicle crossed over the lane marking towards oncoming traffic. While making a turn, encroaching referred to crossing over the lane marking nearest the inside of the turn, while wide occurred when the driver crossed over the outside lane marking [27, 28]. Signaling errors referred to making a turn or a lane change without activating or deactivating the turn signal. Signaling errors were recorded as a dichotomous yes/no variable and were assessed 100 feet before and after turning or changing lanes. Speeding and lane maintenance driving errors were also captured using data from the mounted cameras (i.e., two GoPro cameras, three USB cameras) and a Freematics ONE
Information about the timing, duration, and count of IVIS and ADAS systems were recorded using video of the Camry’s dashboard (i.e., the multi-information display) and side mirrors (i.e., the blind spot monitor alerts). When the IVIS and ADAS features were activated, icons and alerts appeared on the display and were captured on the video. The relevant IVIS and ADAS variables (timing, duration, and count of these activations) were detected using a computer vision algorithm that took images generated from the videos as input and returned whether certain pre-determined objects (e.g., interface icons represent the different IVIS and ADAS systems as shown in Fig. 1) were present, and the length, count, and duration of these IVIS and ADAS events. The computer vision models were trained to detect the activation of Lane Departure Warnings, Lane Steering Assist, and Adaptive Cruise Control. A separate computer vision model was trained to detect the number of Blind Spot Monitor alerts. Finally, the Freematics system collected the vehicle’s speed (km/h) and GPS location (latitude and longitude).
Google Map Image of the Road Course. Legend: Drive 1 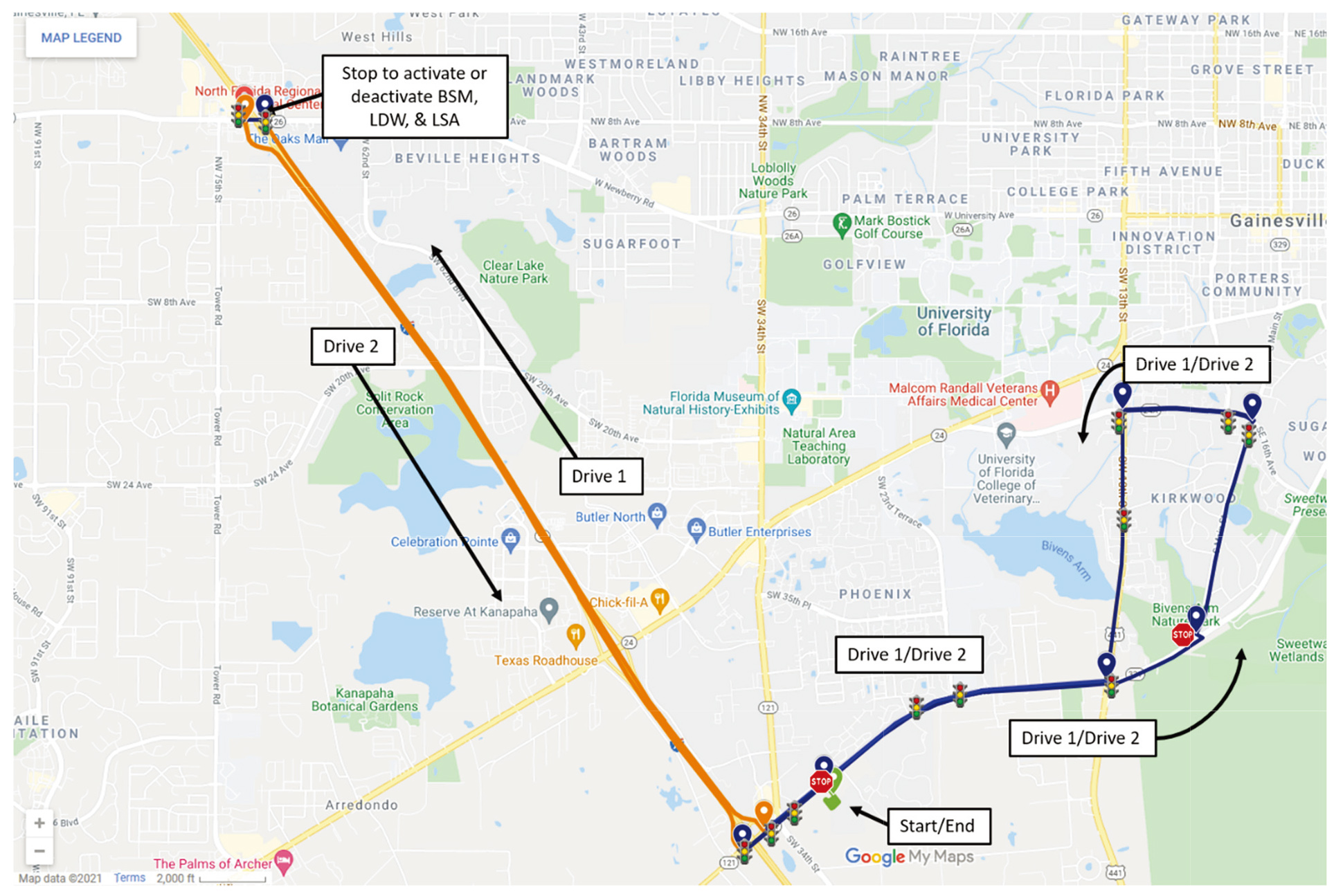
Consistent with existing literature on road course development [27, 28], the driver rehabilitation specialist used Google maps (Google, n.d.) to develop a road course for this study (see Fig. 3). To ensure that participants drove under a variety of conditions, the road course included 29 controlled intersections (i.e., includes traffic signs or signals), 107 uncontrolled intersections, 11 left turns, and 11 right turns. The speed limits varied between 10–70 mph (16–112 kph) on two-lane and four-lane roadways and a divided highway. The zones included: a parking lot to orient the participant to the vehicle (10–20 mph/16–32 kph), a suburban zone (21–50 mph/34–80 kph), and a highway zone (51–70 mph/51–112 kph). The road course was 26.5 miles (just under 43 km) in driving distance and took approximately 50–65 minutes to drive, depending on traffic flow. When developing the course, the driver rehabilitation specialist and two team members drove the proposed course twice to assess the real-time road conditions (e.g., traffic volume, signage, road geometry, etc.). After the drives, the team members agreed that the traffic and road conditions were similar to documented and standardized road courses [3, 4, 29] and were suitable for on-road data collection.
The driver rehabilitation specialist documented errors on a standardized error sheet (see Appendix). Modeled after Classen et al. [27], the error sheet was divided into three zones, the parking lot, suburban roadways, and a highway – and provided an area for the driver rehabilitation specialist to log the speed, lane maintenance, and signaling errors. Additional factors were recorded including total errors made, weather conditions (i.e., sunny, cloudy, and rainy), and if participants had prior experience with IVIS and/or ADAS technology. Three dichotomous Yes/No questions distinguished IVIS and/or ADAS experience using IVIS exclusively, using ADAS exclusively, or using both IVIS and ADAS. During the trial drives with the team members, the driver rehabilitation specialist collected the driving errors as per the above procedure and protocol. For telemetry and video data, variables were segmented into different parts of the road course using GPS information from the Freematics ONE
Participants drove a 2019 Toyota Camry XLE vehicle equipped with IVIS and ADAS, cameras, and the Freematics ONE
Specifically, the drive started in a parking lot, led to a suburban area, and then a highway area. Right after exiting the highway, the driver rehabilitation specialist required the participants to stop the vehicle in a parking lot for (dis)enabling the IVIS and ADAS depending on the condition that they were allocated to (with or without IVIS and ADAS). Next, participants completed the drive described above, but in reverse order. The driver rehabilitation specialist used standardized and scripted verbal cues to give directional instructions (e.g., “when it is safe, change your lane”). All three participants completed the entire drive as instructed by the driver rehabilitation specialist and according to the study protocol.
Data collection
Besides driving errors logged on the standardized error sheet, onboard data recording of kinematic data (i.e., vehicle’s speed and GPS location) were collected from the secure digital card inserted in the Freematics One
Video data was cleaned and processed using the computer vision models and a Python script to extract the counts, durations, and other relevant data (e.g., direction of lane departure) from the IVIS and ADAS feature activations. A human research assistant checked the outputs of the computer vision model and corrected the discrepancies. Kinematic data was cleaned and processed to determine the different segments of the drive (suburban vs. highway; IVIS and ADAS activated vs. not activated) and the associated speed limits using the GPS coordinates. For each segment, the vehicle’s speed was compared with the posted speed limit. Each time the speed was greater or under 5 mph it was counted as either an over-speeding or under-speeding error. The total number of speeding errors was calculated by summing the errors across the road segments for the ADAS activated vs. deactivated conditions.
Data analysis
To determine the feasibility of capturing the driving errors of interest (i.e., speeding, lane maintenance, and signaling errors), recorded data from the driver rehabilitation specialist and the onboard-collected data were evaluated. For speeding errors, both the driver rehabilitation specialist and the Freematics system logged speeding errors during the drives. However, for lane maintenance errors, the video data could only be used for identifying lane departures when the ADAS technology was active. Thus, the driver rehabilitation specialist’s assessment of errors made during turns and straight driving was used to evaluate lane maintenance to allow for comparisons when the technology was on and off. Finally, signaling errors were evaluated using the driver rehabilitation specialist’s on-road assessment because the telemetry and video data was unable to capture this type of error.
Results
Speeding errors logged by both the driver rehabilitation specialist and Freematics
Number of speeding errors logged by the driver rehabilitation specialist
Number of speeding errors logged by the driver rehabilitation specialist
Numbers of speeding errors logged by the Freematics system
Numbers of wide and encroaching errors by the driver rehabilitation specialist
As indicated in Table 2, the effect of IVIS and ADAS on over-speeding errors logged by the driver rehabilitation specialist varied between participants. Compared to the driving condition with IVIS and ADAS disabled, IVIS and ADAS enabled reduced over-speeding errors for Participant 1. Participant 2 did not make any errors regardless of condition (i.e., IVIS and ADAS activation or deactivation). Participant 3 had more over-speeding errors when IVIS and ADAS were activated compared to when it was deactivated. In terms of the under-speeding errors, Participant 2 and Participant 3 had more under-speeding errors when IVIS and ADAS were activated. Participant 1 made no under-speeding errors regardless of the condition.
Though the absolute number of speeding errors captured by the Freematics system differed from the driver rehabilitation specialist, the overall trend in over-speeding errors was similar (see, Table 2). For under-speeding errors, all three participants made more under-speeding errors when IVIS and ADAS were activated, compared to when it was deactivated. However, for Participant 1, the difference was small (19 under-speeding errors when IVIS and ADAS were activated, versus 15 under-speeding errors when IVIS and ADAS were deactivated). Overall, and as expected due to sampling rate, the Freematics system logged more over-speeding and under-speeding events than the driver rehabilitation specialist.
Participant 1 and Participant 2 made fewer lane maintenance errors (i.e., encroaching and wide errors) with IVIS and ADAS in the activated vs. deactivated condition. Participant 3 had more lane maintenance errors when IVIS and ADAS were activated compared to when it was deactivated. Specifically, Participant 1 made two wide errors and one encroaching error when IVIS and ADAS were deactivated, while no errors occurred in the IVIS and ADAS activated condition. Participant 2 made two wide errors with IVIS and ADAS deactivated, and one wide error with IVIS and ADAS activated. Finally, Participant 3 made three wide errors with IVIS and ADAS deactivated, in contrast to four wide errors and one encroaching error with IVIS and ADAS activated (see, Table 3).
Signaling errors logged by the driver rehabilitation specialist
According to the driver rehabilitation specialist, none of the three participants made signaling errors, regardless of IVIS and ADAS being activated, or not.
Discussion
Purpose
The current study examined the feasibility of procedures and measures by having healthy volunteers drive a standardized road course with and without the activation of IVIS and ADAS. The research team evaluated the feasibility of measures by collecting and comparing three driving performance measures, of significance for people with PD (i.e., speed, lane maintenance, and signaling errors [4] (Classen et al., 2014)). Specifically, the feasibility of the driving measures, data collection systems, and procedures used to evaluate the driving errors of three healthy volunteer drivers under the two conditions (IVIS and ADAS, activated vs. deactivated), were examined.
Speeding errors
Both the Freematics system and the driver rehabilitation specialist were able to log errors in driving behaviors under both driving conditions (IVIS and ADAS (de)activation). The Freematics system was capable of capturing speeding errors (i.e., over-speeding and under-speeding) by comparing the vehicle’s instantaneous speed to the posted speed limit. The driver rehabilitation specialist’s notes pertaining to flow of traffic, weather, and other contextual factors – provided a useful context for interpreting the speed data. The feasibility study showed that both methods captured the general trends of whether individual participants were over- or under-speeding, given the two driving conditions.
Lane maintenance errors
For lane maintenance errors, vehicle instrumentation (i.e., video of the car’s multi-information display) was used to count the number of activations of the Lane Departure Warning and Lane Steering Assist when the IVIS and ADAS were activated, and when lanes were clearly marked and visible – thus they were not engaged when the drivers performed a turning maneuver. In contrast, the driver rehabilitation specialist was able to record the lane maintenance errors (i.e., encroaching and wide errors), and assess the quality of the turn, regardless of the (de)activation of the IVIS and ADAS. The feasibility study demonstrated that it was possible to capture differences in lane maintenance errors made by different participants. Furthermore, the standardized data collection sheet allowed for categorizations of lane maintenance errors (wide or encroach) during specific turns or sections of the road course.
Signaling errors
For signaling errors, due to the position of the turn signal indicators on both the multi-information display and the side mirrors, it was not possible to reliably log participants’ signaling during the drive using the cameras and computer vision models in the current data collection system. Thus, the driver rehabilitation specialist was solely responsible for capturing signaling errors made by the participants. None of the participants in the feasibility study made any signaling errors.
Significance of driver rehabilitation specialist data
While it is tempting to rely solely on vehicle instrumentation to capture driving performance, the use of two separate data collection methods allowed both the driver rehabilitation specialist and the vehicle instrumentation to contribute to the findings. For example, over-speeding and under-speeding were determined by comparing the reported speed of the vehicle with the posted speed limit, plus or minus 5 mph, consistent with Florida statute [30]. The driver rehabilitation specialist categorized speeding errors on the road by visually inspecting the speedometer during the drive while also monitoring the road conditions and general safety of the drive. In contrast, the Freematics telemetry system recorded the vehicle’s speed at 20 Hz, a much higher sampling frequency than the driver rehabilitation specialist. This difference was represented in the results through the higher counts of over- and under-speeding by the Freematics system, as the vehicle instrumentation can better capture short periods of over-speeding. However, when evaluating under-speeding errors, the driver rehabilitation specialist considered traffic information, such as the front traffic light turning red, or a vehicle cutting into the lane – and thus provided contextually rich information to better interpret the driving maneuver. If the speed was 5 mph below the posted speed limit because of the traffic situation (e.g., the slowing traffic or the traffic signal ahead), the driver rehabilitation specialist did not consider this low-speed driving as an under-speeding error. In contrast, the under-speeding counts created using the Freematic’s telemetry information were based solely on the speed and did not have access to this additional information. Additional sensors and data fusion algorithms were needed to make sense of the driving situation to compare with the critical reasoning of the driver rehabilitation specialist. Thus, a discrepancy existed in the number of speeding errors between the Freematics data and the results from the driver rehabilitation specialist, with the Freematics data likely overestimating the number of under-speeding events.
During the IVIS and ADAS deactivated condition, the research team was not able to collect lane maintenance errors through the camera. In comparison, the driver rehabilitation specialist recorded lane maintenance errors (i.e., wide and encroaching errors) under both IVIS and ADAS (de)activated conditions, for straight driving and during turns. Similarly, the research team relied on the driver rehabilitation specialist to collect signaling error data since no device in the current data collection system could capture the vehicle’s signaling. As per Florida statute the use of a signal is needed for a turn or lane change and its use should be observed 100 feet before and after such an event [31] The ability of the driver rehabilitation specialist to log this diverse set of variables while drawing on their knowledge of the driving context, makes them an invaluable part of the data pipeline.
There are implications of the current data collection procedures that rely on qualitative assessments made by the driver rehabilitation specialist only. First, the driver rehabilitation specialist could misjudge or misidentify driving errors. However, the additional instrumentation in the vehicle (e.g., through the dashcam, the vehicle telemetry data, and the mirror cams) helped to mitigate these errors by allowing the driver rehabilitation specialist to revisit and revise errors if needed. Second, using a driver rehabilitation specialist can be costly due to the length of the experimental drives and involvement before (set-up and explanation), during (recording errors) and after (report writing) the drive. However, these costs may be justified as the driver rehabilitation specialist also serving as a safety monitor during the on-road section. The need to have a trained driver rehabilitation specialist is especially important when dealing with driver populations that may be more prone to driving errors, such as drivers with PD [4, 32, 33]. Replicating the expertise of the driver rehabilitation specialist in using contextual information (e.g., traffic flow, driving environment, etc.) to process driving performance measures is challenging. However, building a dataset including both “ground-truth” judgments made by a driver rehabilitation specialist, and a rich dataset of vehicle telemetry and video data – allowed the research team to generate future machine learning algorithms to simplify the data management process. As such, this is an exciting new and plausible opportunity for occupational therapists, driver rehabilitation specialists, and engineers to collaborate – and as such to better serve medically-at-risk drivers with automated vehicle technologies.
Taken together, the results of the feasibility study provide evidence that the procedures and data collection methods used were effective in capturing the important driving performance outcomes used to evaluate the benefits or drawbacks of IVIS and ADAS systems on the driving performance in healthy volunteers. The feasibly study also allowed for the refinement of the experimental procedure, equipment setup, and participant orientation to the use of the equipment. The feasibility of the road course and the variety of driving situations encountered were assessed by the team and slight refinements were made. The equipment setup process and corresponding video data analyses informed the set-up of the instrumentation, i.e., cameras and sensors. The feasibility study also demonstrated the utility of data obtained from both the driver rehabilitation specialist and the vehicle instrumentation.
Conclusions
This study confirmed the sufficiency of the equipment set-up and proposed procedures to collect driving performance data, under IVIS and ADAS activated and deactivated conditions. As such the feasibility study contributed to the successful implementation of a randomized clinical trial examining autonomous vehicle technology as an intervention to support drivers with Parkinson’s disease. Feasibility study findings allowed comparison of data collections from both the driver rehabilitation specialist and the Freematics system. Each method captured driving errors with IVIS and ADAS (de)activated. However, the number of speeding errors generated by the Freematics system and those collected by the driver rehabilitation specialist differed. Considering the limitation of the Freematics data (i.e., relying solely on vehicle speed and the speed limit to determine speeding errors), the driver rehabilitation specialist contributed to both the accuracy of the speeding data and being engaged in a valid method of collecting these data. As such, the team is well-positioned to compare driving errors in different driving conditions. The greater understanding of data collection methods may also help the team identify additional phenomena occurring in drivers with PD, beyond those occurring during this feasibility study with healthy drivers. This feasibility study was a critical step to ensure practicality of the intervention testing and reliable data collection for the novel randomized clinical trial that proceeded.
Author contributions
Dr. Sherrilene Classen conceived the parent grant and is PI, she also led design on the feasibility study referred to in this manuscript and supervised performance of all work. Dr. Classen directed the data analysis and led the results interpretation. The manuscript was prepared in conjunction with Drs. Winter, Giang, and Wei. She reviewed all drafts and provided revisions. Her important intellectual content included content expertise for driving rehabilitation/research, Parkinson’s Disease, and preparation for clinical trials. Dr. Classen supervised the team including direct supervision/co-writing with Sandra Winter and Robin Wei and student supervision of Mary Jeghers.
Dr. Sandra Winter was a contributor to parent grant conception and a Co-investigator. She wrote the final drafts leading to this submission, with review by Dr. Classen. Her important intellectual content included adding the clinical perspective for occupational therapy, and adding a section on occupational therapy and engineering collaboration. Dr. Classen supervised the team including direct supervision/co-writing with Sandra Winter and Robin Wei and student supervision of Mary Jeghers. Dr. Winter had a supervisory role with Dr. Wei and Mary Jeghers.
Dr. Robin Wei was a Post-doctoral fellow at the time of the study. He was part of feasibility study design, planning and implementation. His performance of work focused on technical support, engineering of vehicles, data collection and data management. Dr. Wei analyzed the data under supervision of Drs. Classen and Giang. He wrote initial drafts of manuscript under guidance of Drs. Classen and Giang.
Dr. Mary Jeghers contributed practical and clinical guidance to feasibility study from perspective of Driver Rehabilitation Specialist. She monitored safety and collected data during on-road portion. She reviewed drafts of manuscript and provided feedback.
Mr. Jason Rogers contributed planning of feasibility study from Computer Science/IT perspective. Performance of work included selection and set-up of test vehicle including all instrumentation, planning for data collection and data management.
Dr. Wayne Giang was a was a contributor to parent grant conception and a Co-investigator. He planned aspects of feasibility study from an engineering perspective. His performance of work included collaboration regarding selection and set-up of test vehicle including all instrumentation, planning for data collection and data management. Dr. Giang also is the leader of the lab where data was stored and analyzed. Dr. Giang guided the data analysis dedicated to car IVIS and ADAS data, data from additional instrumentation, and creation of algorithms for data analysis. He co-wrote manuscript sections on methods and results. His important intellectual content contributions included engineering knowledge related to autonomous vehicles and necessary data capture sensors. Dr. Giang participated in supervision of Dr. Wei (post-doctoral fellow) and supervised students from his lab engaged in data management and data analyses.
Ethical considerations
This feasibility study was conducted under the affiliation of a randomized controlled trial (RCT) entitled: Driving Performance of People with Parkinson’s using Automated In-Vehicle Technologies. The university issued institutional full review board (IRB) approval (IRB #: 202002321) in 2020.
Footnotes
Acknowledgments
The authors thank the volunteer drivers as well as the infrastructure and support from the Institute for Disability, Activity, Participation and Technology (I-DAPT) and the Human Systems Engineering Laboratory in the Department of Industrial and Systems Engineering at the University of Florida. This study was supported by the National Institute on Disability, Independent Living, and Rehabilitation Research under award number 90IFRE0035. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Disability, Independent Living, and Rehabilitation Research.
Conflict of interest
This study was supported by the National Institute on Disability, Independent Living, and Rehabilitation Research under award number 90IFRE0035. The authors have no conflicts of interest to declare.
Appendix. Standardized Error Sheet
Zone
Directions & roadways
Length (miles)
Speed
Lane maintenance
Signaling
Comments
Over
Under
Encroach
Wide
Orientation to vehicle
UF Fixel parking lot
0.60
RIGHT on SW Williston Rd
Suburban roadways
SW Williston Rd
2.35
LEFT on S Main St
S Main St
1.22
LEFT on SW 16
SW 16
0.72
LEFT on SW 13
SW 13
1.50
RIGHT on SW Williston Rd
SW Williston Rd
2.14
RIGHT onto I75 North on-ramp
Highway roadways
I-75 North
4.82
LEFT on W Newberry Rd
Suburban roadways
W Newberry Rd
0.14
RIGHT into Hardee’s parking lot
Hardee’s parking lot
0.05
Exit straight out of Hardee’s parking lot onto I75
South entrance
Highway roadways
I-75 South
4.93
LEFT on SW Williston Rd
Suburban roadways
SW Williston Rd
2.94
LEFT on S Main St
S Main St
1.22
LEFT on SW 16
SW 16
0.72
LEFT on SW 13
SW 13
1.50
RIGHT on SW Williston Rd
SW Williston Rd
1.71
LEFT into UF Fixel Institute
Speeding
Over
Under
Lane Maintenance
Encroach
Wide
Signaling
Notes:
Weather:
Experience with IVIS/ADAS:
Yes
No
Additional info:
Drive 1: IVIS/ADAS
ON
OFF
Drive 2: IVIS/ADAS
ON
OFF
Note. The standardized error sheet contained information about zones, direction of roadways, length of each roadway, driving errors made in roadways, comments associated with driving errors, weather information, experience with IVIS and/or ADAS technology, and allocation of IVIS/ADAS to Drive1 and Drive2.