
Abstract
BACKGROUND:
Total hip arthroplasty (THA) is one of the most common orthopedic procedures in developed countries, and the high volume of surgery and the socioeconomic burden of failures demand continuous optimization. Operative time has been identified as a significant independent factor influencing the clinical outcome of THA.
OBJECTIVE:
The aim of this study was to analyze factors influencing the operative time for THA in a large, single-center cohort.
METHODS:
A consecutive series of 7,674 cases undergoing primary THA was identified, and after multiple imputation of missing values, univariable and multivariable linear regression analyses were performed.
RESULTS:
In the univariable analysis, all factors showed significant influences on operative time, while multivariable regression analysis revealed that sex, a diagnosis of hip dysplasia and small femoral component size did not reach significance. Younger age, an underlying diagnosis other than osteoarthritis or hip dysplasia, a large stem size, usage of a conventional stem rather than a short stem, a larger cup size and a cemented fixation technique, however, remained significantly influential in terms of a longer operative time.
CONCLUSIONS:
This study identified risk factors for longer operative time that in turn is associated with a higher rate of periprosthetic joint infection and impaired clinical outcome. Our findings could help to refine scheduling of total hip arthroplasty procedures in times of increasing cost and efficiency pressure.
Background
Total hip arthroplasty (THA) is one of the most common procedures in orthopedic surgery, undertaken in up to 200 inpatient cases per 100,000 of the population each year in more developed countries [1]. The procedure has become highly standardized, with strict indications, pre-operative templating, standardized surgical techniques and postoperative care and rehabilitation considered essential. While the overall outcome of THA is excellent in most single- or multicenter reports and national registries, the high volume of surgery and the immense socioeconomic burden of failures demand continual optimization and critical assessment of established standards. Operative time has been identified as a significant independent factor influencing the clinical outcome after THA [2, 3]. In particular, the risk of infection in total joint arthroplasty is significantly increased with longer operative time [4, 5, 6].
Various patient-specific or surgical factors might be expected to influence operative time. To the best of our knowledge, there has been no detailed examination of the influence of patients’ demographic and clinical characteristics, and intraoperative factors, on operative time in a large cohort of patients undergoing THA.
We aimed to establish the factors influencing THA operative time in a large, single-center cohort. Besides the clinical importance of operative time in THA, modern health care systems continuously demand increasing efficiency, including better management of surgical capacity [7]. Our study might therefore also help to optimize planning of procedures and inform future financial reimbursement for THA.
Methods
A retrospective cohort analysis was performed, reviewing the arthroplasty database of a single university hospital. A consecutive series of 7,674 patients who had undergone primary THA was identified. Our hospital is a high volume center for THA, and is certified as a center of maximum care for THA in Germany (Endocert
The most recent version of the Declaration of Helsinki was followed. Our local ethics committee approved the study (reference number: 2392–2014) and the requirement for informed consent was waived. All data were pseudonymized before analysis.
Inclusion criteria
The operation management software (OpDis, c.a.r.u.s. HMS GmbH, Norderstedt, Germany) of the hospital information system (HIS) was used to extract data for analysis. All surgical procedures carried out between June 2001 and December 2013 were searched for matches with the effective operation and procedure code for primary THA (5-820.xx) according to the German adaptation (OPS) of the International Classification of Procedures in Medicine (ICPM). Although data extraction was not feasible for each single parameter in all cases owing to incorrect use of the HIS in some cases and incomplete documentation in others, complete datasets were obtained in more than 5,000 cases.
Two femoral implants were mainly used in our institution during the study period: the Bicontact
Exclusion criteria
Prostheses implanted less than 20 times per year were excluded. Patients undergoing hip resurfacing were also excluded.
Data extraction
Operative time, patient age, sex, underlying diagnosis, type and size of femoral component, size of acetabular component and type of fixation (cemented or non-cemented) were extracted from the HIS. Age was documented as an absolute number in years, and patients were allocated to one of three groups: young (
Statistical analysis
Descriptive statistics
Quantitative variables were summarized by mean, standard deviation (SD) and percentiles (0, 25, 50, 75, 100), qualitative variables by count and percentage. Box plots show the median, upper and lower quartile, interquartile range, whiskers and extreme values (
Imputation of missing values
Missing values were multiple imputed (10 times) based on fully conditional specifications. Univariable and multivariable analysis were performed for the original and imputed datasets. Results of the pooled data analysis and available datasets for each variable are reported.
Univariable analysis
For comparison of two groups, a two-tailed Welch-modified
Multivariable analysis
To assess independent effects of multiple variablels, a multivariable linear regression analysis was performed, including all signficant variables from the univarable analysis. The relationship between lnOT and age was examined in two ways: by age group (variant A) or as continuous data (variant B). The pooled results of 10 imputations are shown and coefficients (betas),
IBM SPSS Statistics 22 (IBM Corporation, Armonk, NY, USA) and Microsoft Excel 2008 for Mac version 12.3.6 (Microsoft Corporation, Redmond, WA, USA) were used for statistical analysis. All statistical analyses were undertaken by a biostatistician and a senior resident in arthroplasty.
Results
Descriptive analysis of variables
Operative time was not normally distributed, so was transformed using the natural logarithm (Fig. 1A). The mean age was 65.1 years (range 16–95 years, standard deviation, SD 12.1 years; Fig. 1B). The majority of patients (4,620, 60.2%) were female; 192 (2.5%) stems were cemented and 5,733 (74.7%) were non-cemented, but fixation technique was not recorded in 22.8% of cases. A short stem was used in 2,010 cases (26.2%) and a long stem in 5,621 cases (73.2%); data were missing in 43 cases (0.6%). The femoral stem was small in 2,235 cases (29.1%), medium in 4,022 cases (52.4%) and large in 421 cases (5.5%); data were missing in 996 cases (13.0%). The acetabular size was small in 862 cases (35.3%), medium in 4,015 cases (41.1%) and large in 310 cases (4.0%); data were missing in 1,499 cases (19.5%). Osteoarthritis was the underlying diagnosis in 5,818 (75.8%) of cases, ONFH in 1,108 (14.4%) and HD in 453 (5.9%); other diagnoses were made in 288 (3.8%) of patients and in seven cases (0.1%) data were missing. The influence of each variable on absolute operative time is shown in Table 1.
Histogram of 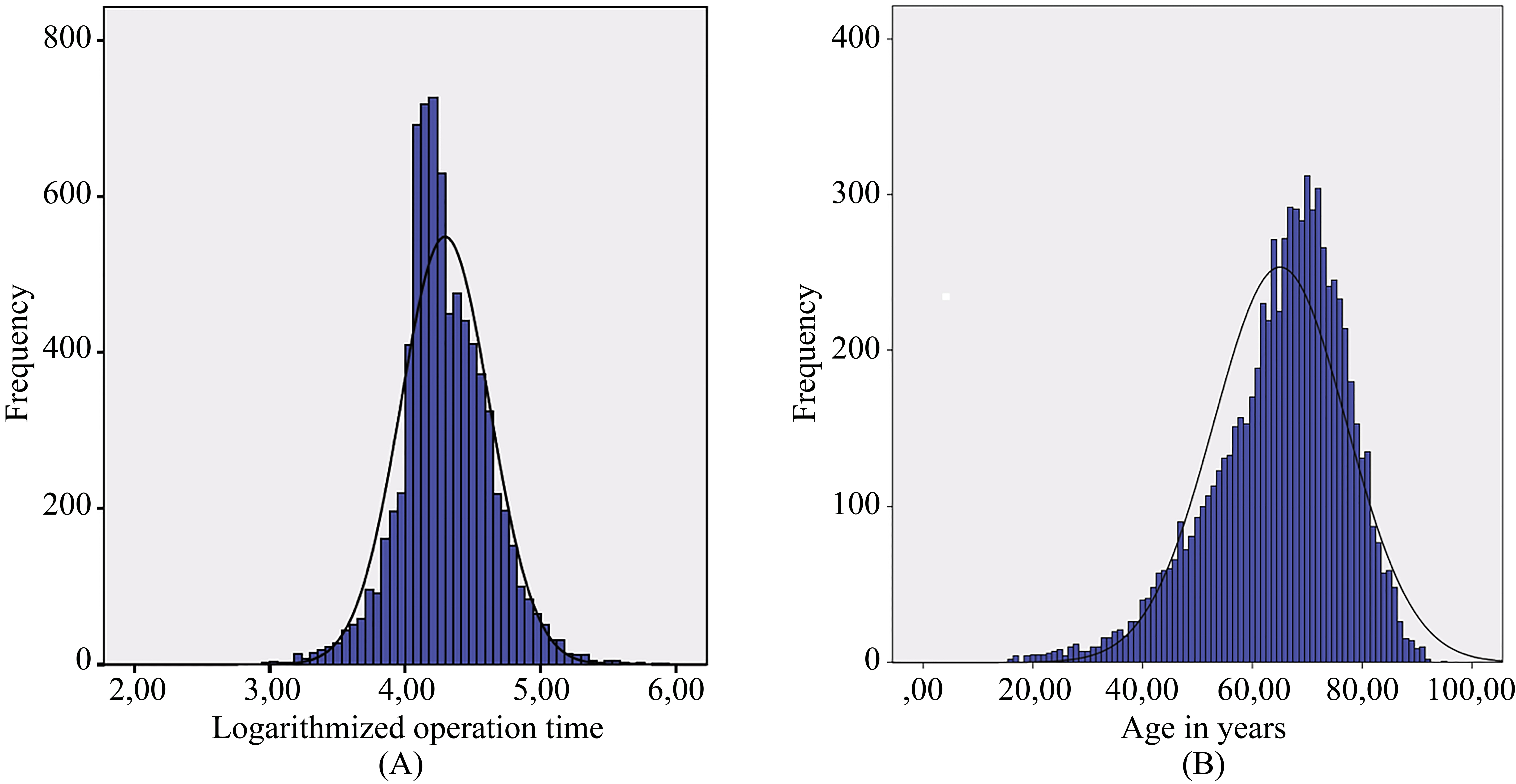
Descriptive analysis of pooled imputed data is shown in Table 2. Over 60% of patient records were complete, and over 80% were either complete or were missing only the femoral fixation type.
Influence of patients’ demographic and clinical characteristics on absolute operative time
Influence of patients’ demographic and clinical characteristics on absolute operative time
Abbreviations: SD, standard deviation; min, minimum; max, maximum; OA, osteoarthritis; ONFH, osteonecrosis of the femoral head; HD, hip dysplasia.
Influence of patients’ demographic and clinical characteristics on absolute operative time for pooled imputed variables
Abbreviations: SD, standard deviation; min, minimum; max, maximum; OA, osteoarthritis; ONFH, osteonecrosis of the femoral head; HD, hip dysplasia.
Multivariable regression analysis of original, non-imputed data for variant A with grouped age
Abbreviations: OA, osteoarthritis; ONFH, osteonecrosis of the femoral head; HD, hip dysplasia.
Multivariable regression analysis of imputed data for variant A with age in groups
Abbreviations: OA, osteoarthritis; ONFH, osteonecrosis of the femoral head; HD, hip dysplasia.
Multivariable regression analysis of original, non-imputed data for variant B (continuous age)
Abbreviations: OA, osteoarthritis; ONFH, osteonecrosis of the femoral head; HD, hip dysplasia.
Multivariable regression analysis of imputed data for variant B (continuous age)
Abbreviations: OA, osteoarthritis; ONFH, osteonecrosis of the femoral head; HD, hip dysplasia.
All analyzed variables were found to significantly influence operative time.
For non-imputed data, fixation technique (
On analysis of imputed data by linear regression, statistically significant relationships between lnOT and age (beta
Multivariable linear regression analysis
Sex, a diagnosis of HD and small femoral component size did not influence lnOT on multiple linear regression analysis, but significant relationships between lnOT and all other variables were found (Tables 3–6). Findings are presented for analysis of non-imputed original data (Tables 3 and 5) and imputed data (Tables 4 and 6) with age by group (variant A, Tables 3 and 4) or analyzed as a continuous variable (variant B, Tables 5 and 6).
Discussion
We examined the influence of patient-specific and surgery-specific variables on operative time in THA. This single center retrospective cohort study found that patient age, femoral component design, acetabular cup size, underlying diagnosis and fixation technique influenced operative time in a multivariable regression analysis.
Operative time is reported to be a significant influence on patient outcome following THA, and to play an important role in peri-prosthetic infection [8]. Although obesity is recognized as a risk factor for increased operative time, little is known about other factors [9]. Possible confounding factors include a wide range of patient-, surgeon-, implant- or hospital-specific factors. While national registries represent the largest collection of data that can illuminate many of these confounding factors (and prosthesis survival), they comprise heterogeneous data from a wide range of hospitals and surgeons. It can therefore be difficult to draw firm conclusions from such large datasets. In contrast, our large single center cohort of over 7,600 THA procedures presents a more homogeneous dataset.
Because of the retrospective design of our study, the type and number of variables was limited; however, seven major variables with nine subcategories were included in the univariable and multivariable regression analyses. While all tested variables were found to be significantly influential in the univariable analysis, multivariable analysis was able to account for confounding variables. Our analysis was also dependent on multiple imputations to reconstruct missing datasets [10]. The use of imputations for missing data has become a standard and widely accepted method in clinical research [11]. Univariable analysis was performed for the non-imputed original datasets as well as the imputed datasets. For transparency, results of the analyses of both the imputed and non-imputed data are presented, but the findings were broadly comparable, suggesting that our imputation technique did not alter our results and allowing us to conclude that the results of the multiple regression analysis of the pooled imputed datasets are also reliable.
Despite the size of our cohort, we categorized patients according to age, and femoral and acetabular implant sizes. We also present two different multiple imputation datasets with age groups or as a continuous variable; analysis of both found that younger age was associated with longer operative time, which is likely a result of increased muscle mass or more challenging anatomy in younger patients. Soft tissue mass and obesity (or increased body mass index) have been found to have a substantial influence on operative time and postoperative complications [12]. We did not examine the influence of body mass index on operative time, and further studies will be needed to examine the influence of age, weight and height on operative time.
Underlying diagnosis also influenced operative time in our cohort. While there was no significant relationship between HD and lnOT, ONFH and other diagnoses were associated with significantly longer operative time than OA. A longer operative time would perhaps be expected in HD owing to the need for acetabular reconstruction, further research is recommended in this field. The use of complex reconstructions and reinforcement cages were not analyzed in this cohort, and thus these factors will also need to be analyzed in future studies.
We found that patients with avascular necrosis of the femoral head, and those with miscellaneous underlying diagnoses required the longest operative time. To a certain extent this is to be expected, as the miscellaneous group comprised diagnoses such as Perthes’ disease and post-traumatic hip fractures that would likely require more complex and challenging surgery. We were surprised, however, that femoral head necrosis was associated with a longer operative time, and propose that this may have been a consequence of these patients’ relative youth and greater muscle mass.
Operative time was significantly longer in patients undergoing cemented THA, likely because of the time taken to prepare and cure orthopedic cement. The size of implanted components influenced operative time, but not in a consistent way – while operative time increased with the size of acetabular cup, and large femoral stems required significantly longer operative time than medium and small stems, the difference between small- and medium-sized stems was not significant. It is possible that an interval rather than an ordinal scale of component size would yield more conclusive results. Interestingly, the implantation of a short stem THA was associated with shorter operative time, perhaps owing to the requirement for less preparatory work on the femur before insertion of the prosthesis [13].
Our study has several limitations. Firstly, we do not have taken the surgeon as the presumably most important influencing factor into account. However, the influence of the surgeon’s skills, experience and personal operative technique is already well-known and obvious and has previously been described several times [2, 3]. Therefore, the focus of this study was placed on further influencing factors beyond the surgical skills. Due to the retrospective study design, a high number of surgeons with inhomogeneous levels of training have contributed to our high study population. They did not only underlie fluctuations due to staff changes, but also underwent a presumed learning curve during the rather long term of observation that would have biased the analysis significantly. Therefore, the surgeon as an influencing factor has been excluded for the benefit of a high case number that in term is supposed to equalize the surgeon factor to reflect the real conditions in healthcare supply.
Secondly, we have no clinical outcome data. Operative time has, however, been clearly identified as a risk factor for outcome and to our knowledge, no large scale analysis of factors influencing operative time has been performed before. Furthermore, we did not take the type of acetabular component or application of acetabular plastics into account. These might influence operative time, and should be examined in future studies. Finally, we had considered whether Cox regression analysis would have been a more appropriate technique for statistical analysis and so ran the analysis in parallel, but were reassured that this yielded similar results. Consequently we are confident that our analysis and findings are robust.
Conclusion
In conclusion, we found that a large number of factors influence operative time in THA. We identified that younger age, an underlying diagnosis other than osteoarthritis or hip dysplasia, a large stem size, usage of a conventional stem rather than a short stem, a larger cup size and a cemented fixation technique are associated with longer operative time in an analysis of 7,674 cases. These findings could help to refine scheduling of total hip arthroplasty procedures, leading to a more efficient utilization of surgical capacities in times of increasing cost and efficiency pressure.
Footnotes
Conflict of interest
Three of the authors (TF, HW and GL) are paid instructors and Consultants for the company B.Braun Aesculap, Tuttlingen, Germany. The other authors have declared that no competing interests exist.