
Abstract
BACKGROUND:
Knee and hip replacement surgery are still the mainstay therapy for osteoarthritis. In spite of the improvement of techniques and implants, anemia is a relatively common complication, with transfusion rates of up to 23% in some centers.
OBJECTIVE:
The purpose of the study was to determine a correlation of transfusions to complications including infection since this topic is still being debated or even disputed in the literature.
METHODS:
This is a level III, single center retrospective observational cohort study of 2760 unilateral primary knee and hip replacements. Preoperative assessment, the number of transfusions and the occurrence of complications were collected and the correlations were analyzed using analysis of variance and logistic regression.
RESULTS:
Fifteen percent of all patients developed at least one complication. Transfusion rate was 9%. Risk factors for receiving a transfusion were female gender, hip replacement, American Society of Anesthesiologists’ Score (ASA)
CONCLUSIONS:
The complication rate is higher in transfused patients. The number of complications rises linearly with the number of transfusions. Infection rate is also higher after a transfusion. Efforts should be made to reduce the transfusion rate.
Introduction
Total knee (TKA) and hip arthroplasty (THA) are therapeutic mainstays for advanced osteoarthritis, and their number is on the rise [1, 2, 3] while the complication rate is falling [4]. Germany is the world leader in the number of total hip and knee replacements at 295 per 100,000 people [5] or 375,000 yearly, with an estimated market value of €2.6 billion. Anemia due to blood loss is a relatively common complication after both hip and knee arthroplasty, and its major form is treated with blood transfusion from an allogenic donor [6]. Authors report transfusion rates after these procedures to be between 5% and 26% [6, 7, 8, 9]. Browne et al. suggested that transfusion rate during or after THA is increasing in the United States and other countries [10]. Blood transfusions have been deemed safe after rigorous screening for hepatitis and human immunodeficiency virus.
However, data shows that blood transfusion still carries risks [11]. Even though studies from orthopedics and other surgical fields show an increased complication rate in patients receiving transfusion [7, 12], there is still an ongoing debate on the validity of this data [6].
The purpose of this study was to determine risk factors for receiving a transfusion, determining if there is a possibility of reduction of transfusion using blood collecting systems and to determine if there is a correlation between transfusions and the overall complication rate. The hypothesis was that the number of transfusions increases the number of complications and the infection rate.
Patients and methods
Patients
The data for our level III, single center, retrospective observational cohort study was collected in house, where, with the exception of open spine procedures, the full spectrum of orthopedic surgery is performed, mainstay being elective surgery. The most frequent surgery is joint replacement surgery, particularly TKA and THA.
At the time of the study, there were 5 senior surgeons in the department and all operations were performed by them or under their immediate supervision. The surgeries have been performed in three operating rooms.
The data was recorded for postoperative in-hospital stay in a cohort of
Patient inclusion diagram.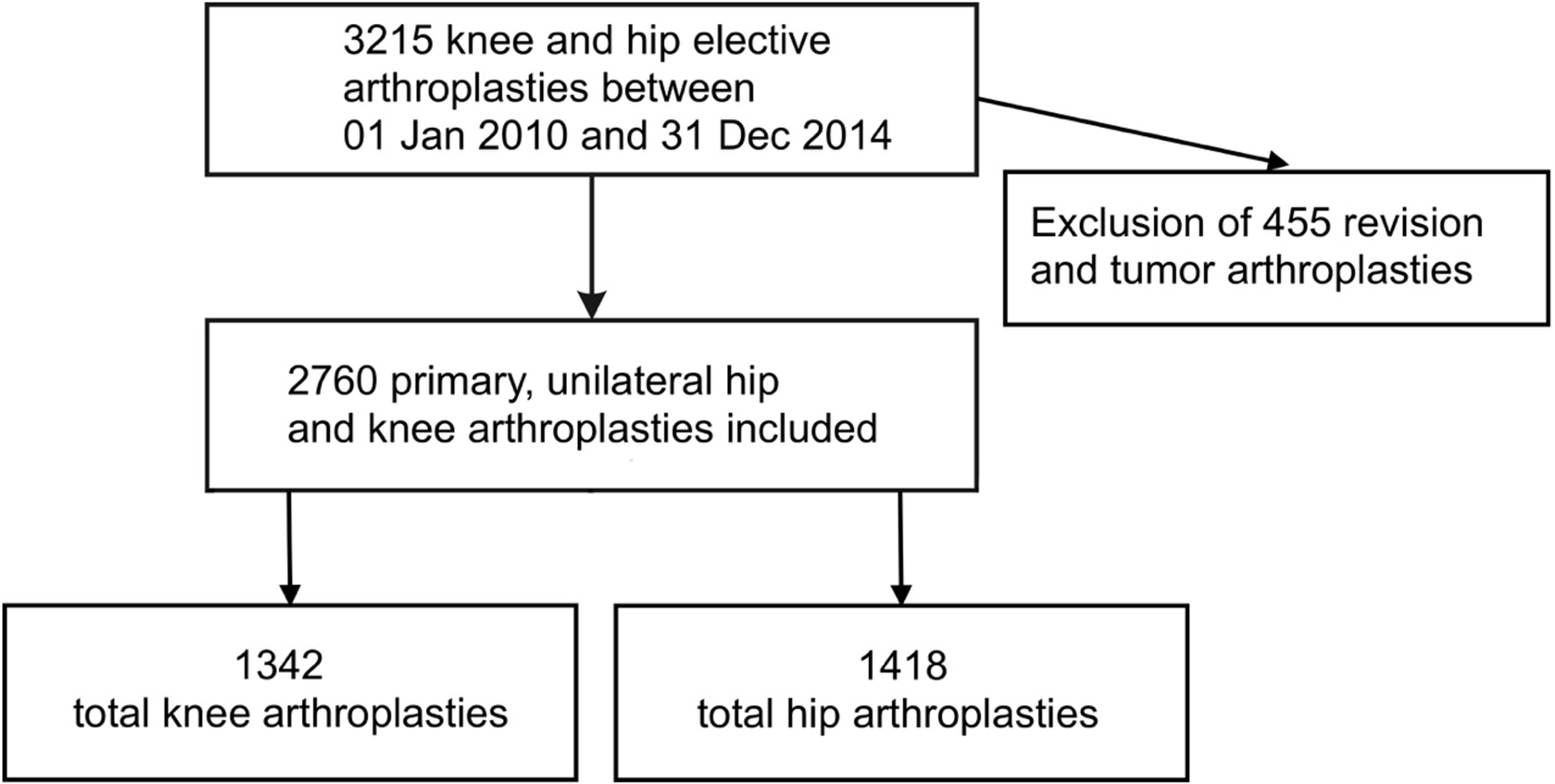
Patients undergoing revision surgery, fracture and tumor prostheses, were excluded from this study. Patient inclusion flow chart is shown in Fig. 1. The average patient age was 69.6 years. The youngest patient was a 23-year-old male who had a dysplastic hip on both sides. The oldest patient was aged 94. The majority of patients
The
Tranexamic acid was not used routinely at that time in our clinic. For thromboembolic prophylaxis enoxaparine (Clexane©; Sanofi, Paris, France) was used. Patients without oral anticoagulation
Ethical committee approval was obtained (study number F-2015-010).
We collected blood intraoperatively and within 6 hours postoperatively, using the intraoperatively applied drainages with the CellSaver System (Haemonetics, Braintree, MA, USA). All patients received a drainage. Contraindication for the use of the CellSaver systems were all types of malignant diseases in the patient history and religious grounds. The retransfusion was done when at least 200 mL of blood could have been retransfusioned. The hemoglobin level was documented preoperatively, after 24 and 48 hours as well as on the 5th day and on the 10th day, if applicable. The drainages were removed after 48 h. Complications were defined as by Dindo et al. [13]. Transfusion trigger were the guidelines of the German Transfusion Society which recommends a single blood transfusion in patients who are symptomatic and have a hemoglobin level lower than 8 mg/dL, or asymptomatic with hemoglobin less than 7 mg/dL [14]. Body mass index (BMI) was calculated from the height and the weight which was collected by the anesthesiologist during preparation. Length of surgery has been documented. Further predictors that were collected are: age, gender, arterial hypertension, usage of anticoagulation and the type, history of myocardial infarction, chronic heart and renal disease, diabetes, chronic obstructive pulmonary disease (COPD) and American Society of Anesthesiologists’ (ASA) score. Lab results that were collected preoperatively were C-reactive protein level and number of leukocytes. The predictors are shown in Table 1.
Predictors for calculating the correlation of transfusion to complications
Predictors for calculating the correlation of transfusion to complications
BMI – body mass index; ASA – American Society of Anesthesiologists; ASS – acetylsalicylic acid; COPD – chronic obstructive pulmonary diease.
Statistical software SPSS 22 (SPSS, IBM, Armonk, NY, USA; licensed to University of Marburg) was used to determine the frequency of single factors and complications. Analysis of variance was used for calculating the correlations. Comparison of mean and median showed a normal distribution of the data. The odds ratios were calculated with a confidence interval of 95% using binary logistic regression and
Results
Results
Table 2 shows the results. A total of
Gender did not play a role in the development of a postoperative complication, but female gender was a risk factor for receiving a transfusion (
The risk factors for receiving a transfusion were the following: an ASA score of III and IV, age more than 70 years, history of myocardial infarction, chronic cardiac disease, diabetes mellitus, chronic kidney disease, and length of surgery (
Preoperative hemoglobin level showed no correlation to the number of transfusions (
Scattered plots of the number of complications (y axis) and number of transfusions (x axis).
Four hundred and seventeen patients (15%) developed a complication. Complication rate was 34.7% (
Transfusion increases the complication rate and the risk of wound infection. This confirms the hypothesis of this study.
The general risks associated with allogenic transfusion have been well known for some time and include immunological reactions [15], disease transmission, transfusion-induced coagulopathy, thromboembolic complications [16], transfusion-induced sepsis, and acute lung injury [17]. Effective preoperative management programs that reduce the need for transfusion already exist [18].
This study is not the first in this field that had these observations. Two recent studies [7, 12] had similar results to this study. Their findings included that the prediction factors for receiving an allogenic transfusion were hemoglobin level, age, female gender, BMI, high creatinine levels, TKA, operating room time, and blood loss. The transfusion rates reported were 9.27% for TKA and 26.6% for THA. In their study the rate of surgical site infection rose from 0.5% in non-transfused patients to 2.4% in transfused patients. These findings correlate almost to the decimal with the findings of this study. Interestingly, in the Frisch study, high hemoglobin was protective against an allogenic transfusion, which we did not observe. The lack of protection against transfusion has been observed in other studies [19]. One additional study [20] had similar results, but the chronology of events has not been cleared and it is a multicentric cohort. It still adds to the argumentation of the negative role of the transfusions.
The difference in the infection rate between transfused and non-transfused patients has also been recently observed in Europe [21]. Also, increased mortality rates, higher rates of pneumonia, and higher rates of cardiovascular and cerebral complications have already been documented [22].
One of the main motivations for doing this study was our contribution to a still ongoing scientific debate whether these correlations are real or completely due to confounding. Since ethical boundaries prevent a double blinded, placebo controlled study, especially on a scale large enough to prove or disprove these correlations, levels II and III studies are the only scientific sources.
Opposite findings to ours regarding the role of transfusion is also well documented in literature [6, 10] with authors blaming confounding. Authors from other surgical fields, such as cardiac surgery report similar correlational findings [15, 23] or claim that transfusions increase mortality and morbidity even in low hematocrit patients [24]. General surgery offers very similar conclusions [25, 26]. There are, however, help and alternatives. Widespread use of tranexamic acid is proven useful [27, 28, 29]. Another well documented alternative is Epoetin alfa but the widespread use is still missing [30, 31, 32].
A very large cohort within one center is a strength of this study in an environment of vast registry data from dozens of clinics that is often used in these types of studies.
The main limitation is the not-controlled retrospective nature of the study. The use of tranexamic acid was very limited, one has to assume that the transfusion levels would be even lower, had it had been used routinely. Additionally, preoperative optimization of hemoglobin is not routinely done since it is in the primary domain of the general practitioner. This would probably impact the reduction of the transfusion rate and consequently the complications eve further.
Level II observational studies have been conducted in the area of hip fracture implants [20]. However, the comorbidity level and average age of these patients does not overlap with elective hip and knee surgery and can therefore not be directly compared.
To conclude the study, both increased ASA score and age were risk factors for a complication. However, the complication rate still is higher in transfused patients and the individual odds-ratios for complication categories have been shown. Also, the number of complications rises with the number of transfusions. Infection rate is also higher. Efforts should be made to reduce the transfusion rate.
Footnotes
Acknowledgments
We thank Prof. Albert Benzing and PD Thomas Leonhard for their support of the study.
Conflict of interest
None to report.