
Abstract
BACKGROUND:
Blood transfusion is a common practice, but it is not without cost and risk. A model that predicts the risk of blood transfusion could guide informed preoperative blood ordering and use of blood loss preventive measures.
OBJECTIVE:
This study aimed to develop a prediction model of blood transfusion in children with developmental dysplasia of the hip (DDH) undergoing surgery.
METHODS:
A retrospective cohort of DDH patients from 2008 to 2017. The included patients were between 1 to 9 years old, underwent anterior open reduction and/or acetabular osteotomy with and without femoral shortening. The unit of analysis was undergoing such an operation. The outcome was allogenic blood transfusion. Potential predictors were age, sex, body mass index (BMI), international hip dysplasia institute grade, type of surgery, intervention bilaterally during the same operative session, primary versus reoperation surgery, the addition of regional anaesthesia, preoperative haemoglobin and hematocrit.
RESULTS:
A total of 524 patients who met the inclusion criteria underwent 721 operative sessions. The median age (interquartile range) at operation was 23 (20–33) months. The blood transfusion rate was 11.8%. Independent predictors were lower preoperative haemoglobin, reduced BMI, simultaneous bilateral surgery and the extent of surgical treatment.
CONCLUSIONS:
The developed prognostic model allows prediction for blood transfusion in DDH patients undergoing surgery.
Introduction
The treatment of developmental dysplasia of the hip (DDH) entails open surgical intervention if nonsurgical measures fail or if the child presents late. The anterior surgical approach, which facilitates wide capsular exposure, is generally preferred if the child is older than one year. An iliac osteotomy is usually added after 18 months of age [1]. Femoral shortening is added in the older child with superior migration of the femoral head and the final decision to do this is made intraoperatively [2].
With open surgical operations, comes the risk of blood loss, which may mandate blood transfusion. Morbidity and even mortality from transfusion related complications are well documented in the literature [3]. In a study that included over fifty-thousand pediatric surgical patients from different subspecialties; blood transfusion was associated with prolonged hospital length of stay and an increased complication rate [4].
Predictors of the requirement for blood transfusion have been studied repeatedly in paediatric craniofacial, cardiac and scoliosis surgery [5, 6, 7], but less in paediatric hip surgery. Recently, Sherrod et al. found in an administrative database that there is, a blood transfusion risk of 9.8% in a subgroup of hip dysplasia patients with no known co-morbidities; the independent risk factors for transfusion in their study were acetabular osteotomy, female sex, operative time and older patient age [8]. Knowledge of the predicted probability of needing a blood transfusion may guide preoperative blood ordering and implementation of costly preoperative blood management programs in high risk patients [9, 10]. Patients with a high probability of blood transfusion may benefit from measures to minimise allogeneic blood transfusion which may include, acute normovolemic hemodilution [11], hypotensive anaesthesia [12], autologous blood donation with or without administration of recombinant human Erythropoietin [13, 14], cell salvage and antifibrinolytics [15, 16].
Therefore, the goal of this study is to develop a prognostic model to predict the probability of blood transfusion in pediatric DDH patients undergoing surgery.
Materials and methods
Patients
The study is based on a retrospective cohort of patients from a single centre. After local ethics review board approval (log number: 16–386), we screened data of consecutive patients that had undergone anterior DDH surgery between February 2008 and July 2017 at a tertiary hospital. Six attending physicians served in the paediatric orthopaedic unit during the study period. Patients were included if they were diagnosed with DDH, operated between the age 1 and 9 years, had an open reduction, pelvic and/or femoral osteotomies. All such operations were included, including reoperations. We excluded patients with syndromic, neuromuscular or haematological diseases.
Surgical procedures
All operations were performed through anterior exposure to the hip under general anaesthesia. Pelvic osteotomy was performed by a single iliac cut with variation in the direction based on surgeon’s preference. Open reduction was accompanied by percutaneous adductor tenotomy. Femoral shortening osteotomy was through a standard lateral approach. Regional anaesthesia used was either caudal epidural or lumbar plexus block.
Outcome predicted
The outcome of interest was any blood transfusion during hospitalisation. Only allogenic blood was administered at the discretion of the anesthesiologist for intraoperative transfusions or the house staff postoperatively for acute anaemia, which is often symptomatic. The institution used a separate consent for blood products transfusion and there was no predetermined transfusion trigger.
Predictors of outcome
Electronic charts and digital radiographs were reviewed to determine predictors and outcome. Predictors were considered based on their availability in routine daily practice. We included age at the time of surgery, sex, body mass index (BMI), international hip dysplasia institute (IHDI) grade [17], type of surgery (i.e., open reduction, pelvic and/or femoral osteotomy), whether both hips were done simultaneously or not, primary versus reoperation surgery, the addition of regional anaesthesia, preoperative haemoglobin and hematocrit. Surgical drains, antifibrinolytics and cell salvage were not used. The IHDI grading is the only subjective measure here and was ascertained by an investigator who was blinded to both predictor variables and outcome.
Data analysis
The study period was maximised to increase the number of outcome events, and hence power and to improve the generalisability of the model. Undergoing an operation was the unit of analysis unless specified otherwise. Possible correlation between multiple operations within the same patient was not taken into account. Each procedure was analysed independently. For univariate analysis, the normality of distribution and equality of variances were assessed graphically. Accordingly, two-tailed two-sample Mann-Whitney-Wilcoxon test, independent Student’s
We used binary logistic regression to determine the strength of the association of predictors with the outcome. We included all predictors in the model and then performed backward stepwise selection. Predictor selection was based on
Results
Fourteen patients (2.6%) had missing hospital electronic charts with absent outcome and were believed to have been missing completely at random, and were excluded. There were 721 operative sessions in 524 patients eligible for inclusion. Other missing clinical variables were assumed to have been missing at random. Multiple imputations were performed for 66 clinical data items; 64 (8.9%) height, one (0.1%) preoperative haemoglobin and hematocrit values. Baseline characteristics along with univariate comparisons are shown in Table 1. Unadjusted analysis revealed no association between sex, side, reoperation and regional anaesthesia. Out of the 721 analysed operations, 85 (11.8%) required blood transfusion once. The median blood transfused was 100 ml and the interquartile range was (50–150), 42.3% of the transfusions were administered intraoperatively.
Participant characteristics at baseline
Participant characteristics at baseline
IQR
Using backward regression and fractional polynomials for continues variables, the predictors in the final model were: preoperative haemoglobin, BMI, simultaneous bilateral surgery and the extent of surgical treatment were independent predictors for blood transfusion (Table 2). All pairwise VIF values were below the predefined cut-off for high collinearity. The ROC which measures model discrimination is seen in Fig. 1. Present the AUC and its confidence interval. An AUC of 0.5 indicates the inability of the model to differentiate between those who do or do not experience the outcome of interest. Calibration is the model ability to estimate the probability of the outcome and shown in Fig. 2; it is close to the 45 degrees line of perfect calibration. The nomogram is drawn in Fig. 3 for estimation of the transfusion probability.
The final logistic regression model for the probability of blood transfusion in pediatric DDH surgery
DDH
The receiver operator characteristic (ROC) curve, the area under the curve (AUC), 95% confidence interval is (0.79 to 0.87).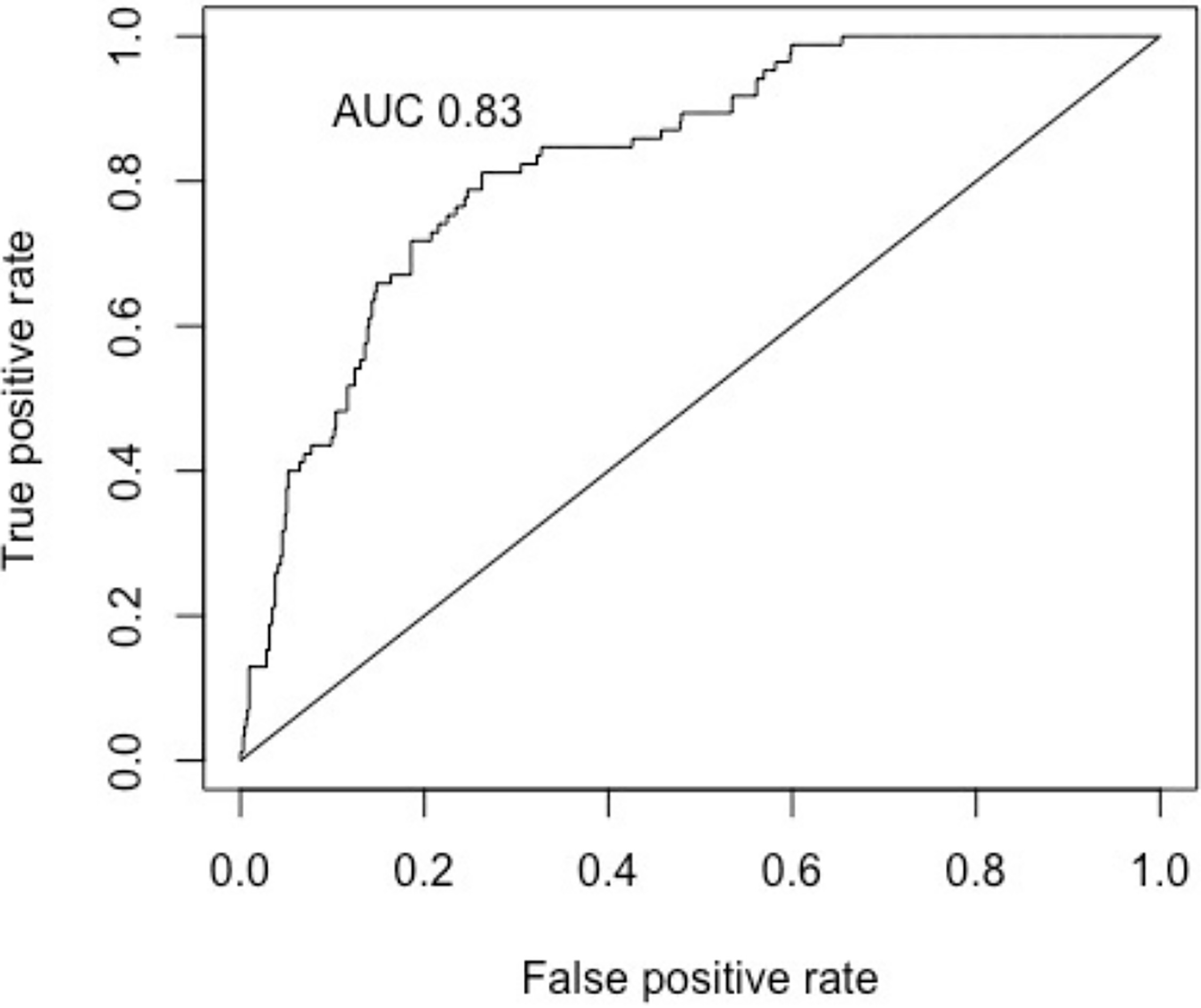
The calibration plot.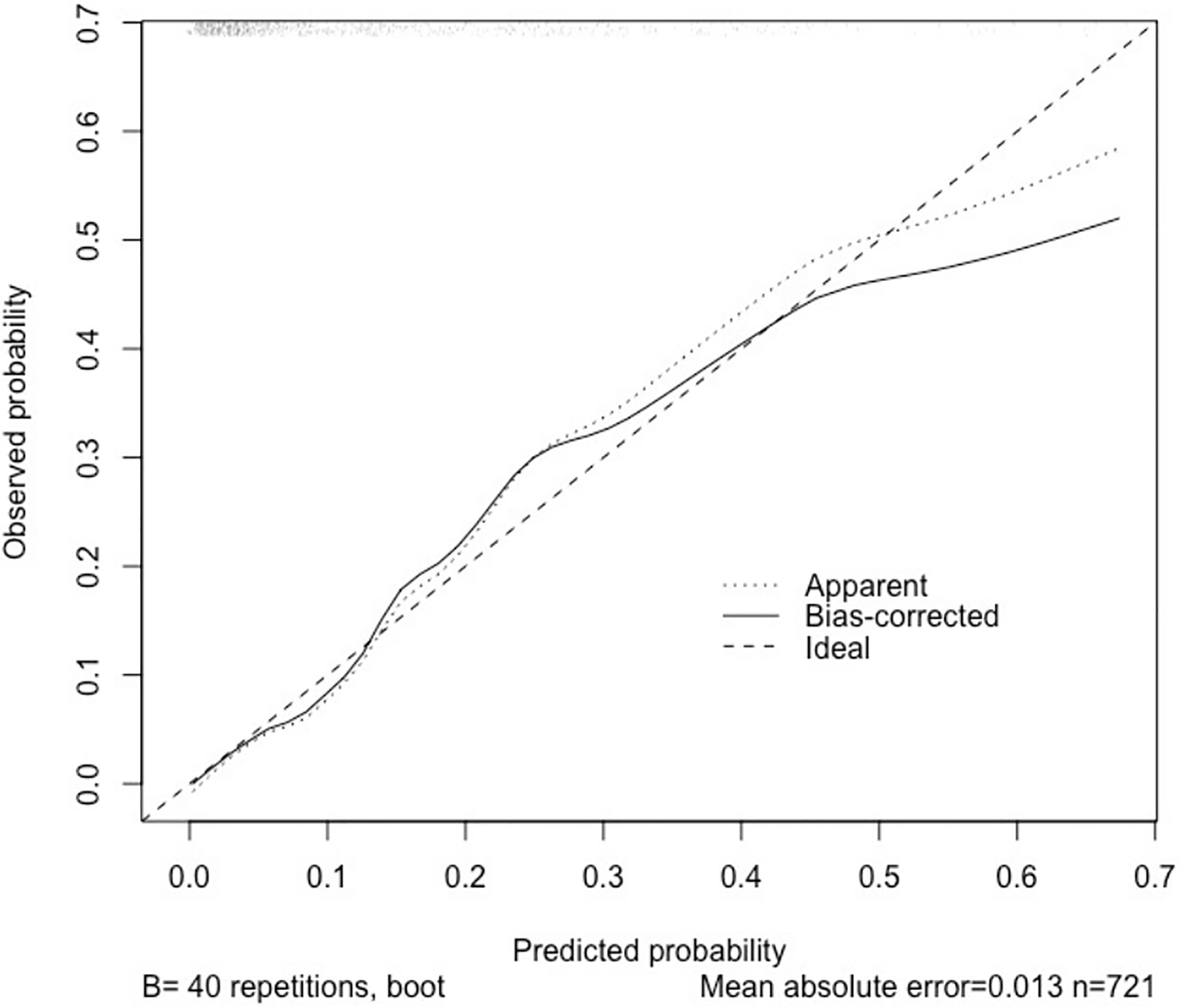
The nomogram. Each predictor with a given value is mapped to the Point axis. The sum of these points is applied to Total points axis. The probability is obtained from the corresponding point on the Probability axis.
We developed and internally validated a model for calculating the probability of blood transfusion in pediatric DDH patients undergoing surgery. The AUC was 0.83, which indicates good discrimination. Independent predictors that increased the risk of blood transfusion were decreased BMI, lower preoperative haemoglobin, bilateral procedures and the extent of surgical intervention. There was an 11.8% risk of blood transfusion.
Sherrod et al. analysed 1,184 patients with all types of hip dysplasia, including neuromuscular and syndromic etiologies, up to the age of 18 years [8]. The transfusion rate for patients without systemic or neuromuscular disease, to approximate the DDH population was 44/451 (9.8%). Also, blood transfusion was associated with longer hospital stay and higher complication rate. The independent predictors were female sex, addition of acetabular osteotomy, increased operative time and older age. Except for acetabular osteotomy, the predictors were not similar to the findings from the present study, largely because of the difference in the variables included in the initial regression model. We did not include the duration of the surgery because it is an intraoperative parameter.
Several variables were associated with higher risk of blood transfusion in the present study (Table 1). This compares well with previous reports, but in different patient populations. In paediatric cardiac surgery patients, Mulaj et al. found that lower preoperative hematocrit levels are an independent predictor of blood transfusion [6]. Vassal et al. analysed 110 paediatric craniotomies for brain tumour removal and found that low preoperative haemoglobin is an independent risk factor for intraoperative allogeneic blood transfusion [5]. In a study of 147 paediatric scoliosis patients by Dupuis et al., a weight below the 3rd percentile was an independent predictor for transfusion [7]. Toyama et al. reviewed 29 studies of blood transfusion predictors in adult orthopaedic surgical procedures, the most frequent independent predictor was preoperative haemoglobin followed by older patient age and increased complexity of the surgery [12]. Although regional anaesthesia is not a biologically plausible predictor, it was included because of the modifiability, and it was not associated with blood transfusion.
Besides implementation of preventive measures, identification of high-risk groups proposed by the model presented here may improve blood product utilisation, and reduce unnecessary preoperative testing and associated costs [19]. Lin et al. suggest that type and screen could be disregarded without jeopardising patients’ safety if the transfusion probability is less than 5% and crossmatching is only performed for patients with clinically significant antibodies or for operations that have an average transfusion volume of 2 units or more [20]. In our cohort, the predicted risk from our model was below 5% in 45% of our operations. This would mean that type and screen could have been avoided in these patients. The number of operations in this low risk that still needed blood transfusion was 3%.
Our study lacks external validation and there were 6.5 outcome events per potential predictor in the full model, which is less than the general rule of 10 events per predictor [21]. We did apply shrinkage to the coefficients of our model to improve predictions in new patients. Still external validation and, if necessary updating of our model, would be valuable. Because empirical evidence suggesting optimal transfusion practices in paediatric surgical patients are sparse, the amount and trigger of blood transfusion remain subjective in many situations [18]. But, we believe that blood transfusion as an endpoint is more objective and meaningful than intraoperative estimated blood loss.
Conclusions
This prognostic model allows prediction of the risk of needing blood transfusion in DDH patients undergoing surgery. Individualised risk predictions may guide clinicians into rational blood utilisation and blood transfusion preventative measures.
Footnotes
Acknowledgments
The authors thank Omar Kasule for his help in the design of this study.
Conflict of interest
None to report.