
Abstract
BACKGROUND:
Total hip replacement (THR) for Crowe type IV developmental dysplasia of the hip (DDH) is still challenging due to specific joint deformities and the high incidence of post-operative complications.
OBJECTIVE:
This study aimed to evaluate the clinical effect of trochanteric slide osteotomy (TSO) combined with a cementless femoral conical stem in THR for the treatment of Crowe type IV DDH.
METHODS:
Thirty-one total hip replacements (26 patients) with Crowe type IV DDH were performed using TSO combined with a cementless femoral conical stem. Surgical outcomes were evaluated using leg length discrepancy (LLD), Harris hip score, and post-operative complications.
RESULTS:
The average pre-operative LLD was 51 mm (range 46–58 mm), decreasing to an average of 10 mm (range 8–12 mm) post-operatively. As a result, the post-operative incidence of the Trendelenburg sign significantly decreased compared with the pre-operative incidence (
CONCLUSION:
TSO combined with a cementless conical stem in THR is an appropriate option for patients with high congenital hip dislocation.
Introduction
Total hip replacement (THR) for Crowe type IV developmental dysplasia of the hip (DDH) is still challenging due to specific joint deformities and the high incidence of post-operative complications [1]. Subtrochanteric transverse shortening osteotomy is a commonly used surgical procedure, which has the advantage of being able to adjust the rotation angle while preserving the original proximal femoral anatomy [2]. Due to the centrosymmetric nature of the intersecting surfaces, adjustment of the two fragments the proximal femoral caused by a transverse osteotomy is easy during the surgery. However, the intersecting surfaces of the two fragments are relatively small, which can increase rotational instability and lead to non-union of the osteotomy [3]. Several modified osteotomy techniques have been developed to overcome these complications, including oblique, step-cut, and chevron osteotomies; however, these techniques usually require longer operative durations and compromise the rotational deformity of femoral anteversion [4]. Furthermore, evidence for the superiority of these techniques is still insufficient [3, 4].
Greater trochanteric osteotomy, or trochanteric slide osteotomy (TSO), preserves the integrity of the sleeve of the musculoskeletal muscles, including the gluteus medius, gluteus minimus, greater trochanter, and vastus lateralis [5]. This technique is mostly used in acetabular fracture internal fixation or complex hip revision, because it provides perfect exposure to the acetabular and femoral sides and minimizes damage to the hip’s soft-tissue envelope [6, 7].
Since 2016, this osteotomy technique, combined with a cementless femoral conical stem system, i.e., a Wagner cone prosthesis, has been used to treat all patients with high congenital hip dislocation at the First People’s Hospital of Wenling. The objective of the present retrospective study is to determine the mid-term effects of TSO combined with a cementless femoral conical stem in patients with Crowe type IV DDH.
Material and methods
Inclusion and exclusion criteria
Inclusion criteria: (1) patients with Crowe type IV DDH who underwent THR in the Department of Arthroplasty at the First People’s Hospital of Wenling between January 2016 and October 2017; (2) patients were treated with TSO combined with a cementless femoral conical stem (Wagner cone; Zimmer Biomet, Warsaw, IN, USA) and a cementless cup (IT; Zimmer Biomet, Warsaw, IN, USA) (Table 1); (3) the related pre-operative data and post-operative outcomes of patients were completely recorded.
Implants size imformation
Implants size imformation
Exclusion criteria: (1) a history of pelvic trauma or previous pelvic surgery; (2) history of hip infection or tumor; (3) absence of any necessary data; (4) lumbar spine stiffness (lumbar spine lateral curve
Patients’ demographics
A total of 26 patients (31 hips) were included in this study (Table 2). This group consisted of one male patient and 25 female patients, with an average age of 49.9 years (range 18–66 years) at the time of operation (Table 2). Five of the female patients underwent two-stage bilateral THR, with a mean interval of 4 months (range 3–6) between operations. Evaluations of pre-operative leg length discrepancy (LLD), pain-related visual analog scale (VAS), and Harris hip score (HHS) were performed, and incidence of the Trendelenburg sign was recorded (Table 3).
Pre-operative, operative, and post-operative procedures
Pre-operative examinations were regularly conducted to aid in the development of personalized surgical plans. Preoperative routine pelvic x-ray and three-dimensional CT reconstruction of the proximal femur and acetabulum were performed to assess the developmental deformities. According to the template measurement, the size of the prosthesis and the position and angle of the Cup were determined. The size of planned osteotomy was also evaluated according to the difference of the length of both lower limbs and the stability of hip joint. Ceramic-to-ceramic bioprosthesis was routinely used during the operation.
All operations were performed under general or epidural anesthesia by the same senior orthopedic surgeon (Jiang Chang), and the posterolateral incision was used routinely. 1–1.5 cm of the femoral calcar was retained and the femoral neck was transected. After resection of the hypertrophic capsule and fibrous scars, the anterior rectus femoris, insertion of the quadratus femoris, gluteus maximus, and the iliopsoas were carefully and completely released. After full exposure, the true acetabulum center was determined and then was carefully reamed. The acetabular cup was installed using press fit technique, when necessary, two or three dome screws were applied to fix the acetabular cup. For those with large acetabular defects (
Diagrams of trochanteric slide osteotomy showing: (A) a short oblique osteotomy being conducted; (B–C) the cutting trochanter fragment being slid anteriorly to facilitate exposure; (D) the osteotomy fragment of the greater trochanter being retracted; (E-F) additional shortening being conducted by progressively resecting bone from the calcar femorale if reduction is difficult; (G) insertion of the implant into the proximal fragment of the femur; (H) titanium cables being used to maintain the abducted position of the hip with tension of the gluteus medius. 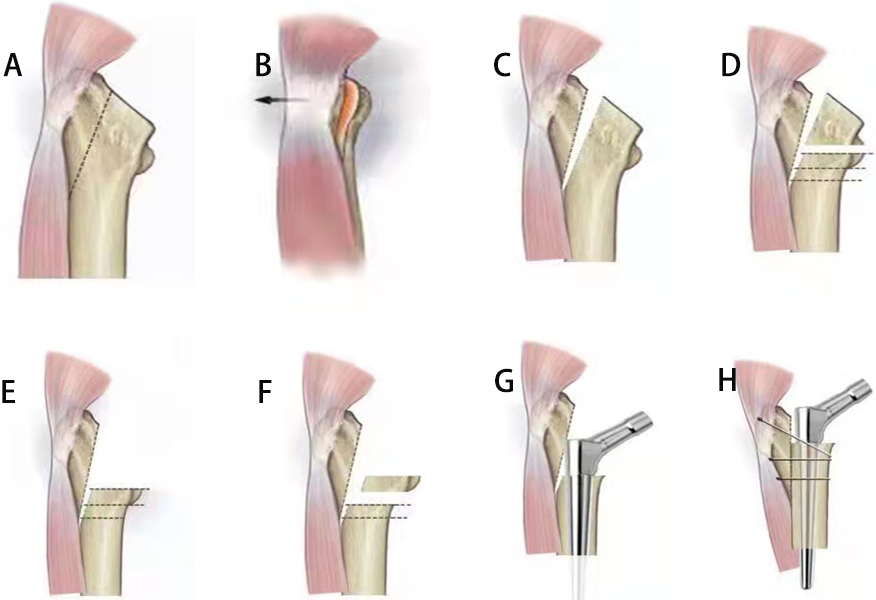
Lower limb traction was used to evaluate muscle tightness and reduction. A short oblique osteotomy was performed using an oscillating saw from posterior to anterior along the proximal end of the femoral neck osteotomy surface to the distal end (see Fig. 1). The length of Proximal femoral osteotomy was adjusted according to preoperative planning and intraoperative comprehensive evaluation. Reaming of the femoral cavity was performed after each osteotomy, and a model was inserted choosing an appropriate anteversion for final evaluation. In order to prevent a split fracture of the proximal femur, prophylactic cerclage wires were usually applied before reaming. After the prosthesis was installed, the osteotomy fragment was reduced in the abductor position and fixed with titanium cables or trochanteric plate to ensure the normal tension of the gluteus medius (see Figs 2–4).
Surgical procedure of trochanteric slide osteotomy showing: (A) position of osteotomy; (B) the cutting trochanteric fragment is shown; (C) the proximal fragment of the femur after osteotomy; (D) the stem is inserted into the proximal fragment of the femur; (E) the trochanteric fragment is reattached to the lateral border of the femoral shaft.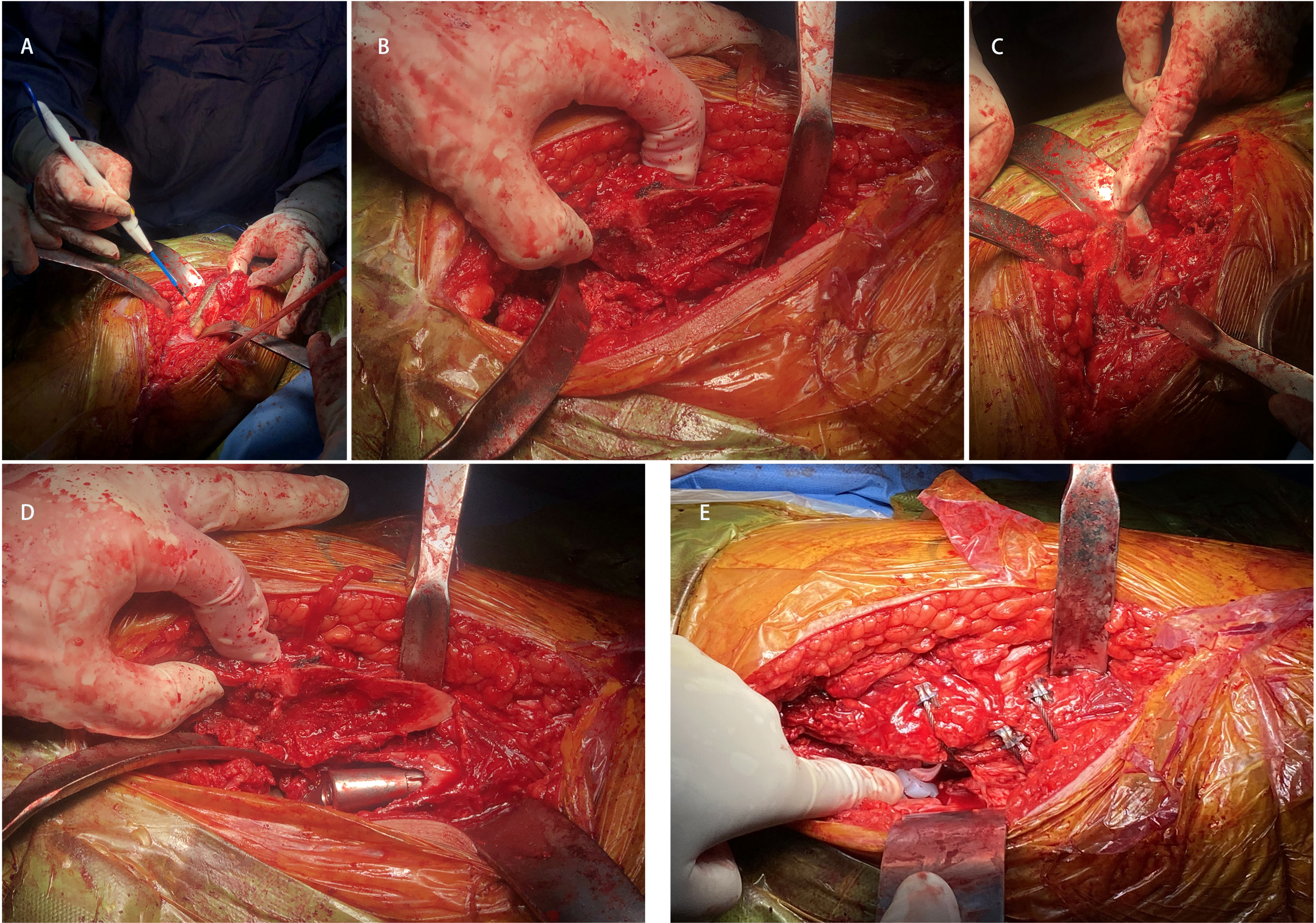
Early postoperative activity was encouraged, if there was no accidental femoral side fracture, the patient was allowed to bear weight with the assistance of crutches 6 to 8 hours after surgery. Complete weight-bearing was usually achieved after 6–8 weeks.
Postoperative follow-up and monitoring of related indicators, including operation time, blood loss, postoperative pain score, hip function score, LLD, Trendelenburg gait and Surgical complication (including intraoperative fracture, bone non-union, deep venous thrombosis, nerve injury, prosthesis loosening, dislocation and infection) were performed after operation.
Statistical analysis
All results were presented as mean value
Results
All patients were followed up for an average of 32.6 months (range 27–39 months) (Figs 3 and 4). The average operating time was 105 minutes (range 90–125 minutes), the average peri-operative blood loss was 640 mL (range 530–800 mL), and the average perioperative allogenic blood transfusion was 2.3 U (range 2–4 U) (Table 2).
Clinically, LLD improved significantly from 51
Patients’ clinical results
Patients’ clinical results
A 32-year-old woman with bilateral high congenital hip dislocation underwent a cementless total hip arthroplasty using treated with trochanteric slide osteotomy: (A) the preoperative radiograph; (B) immediate postoperative of right side; (C) immediate postoperative of left side (2 months postoperatively on the right side); (D-E) Postoperative X-ray follow-up, 14 months of right side and 12 months of left side.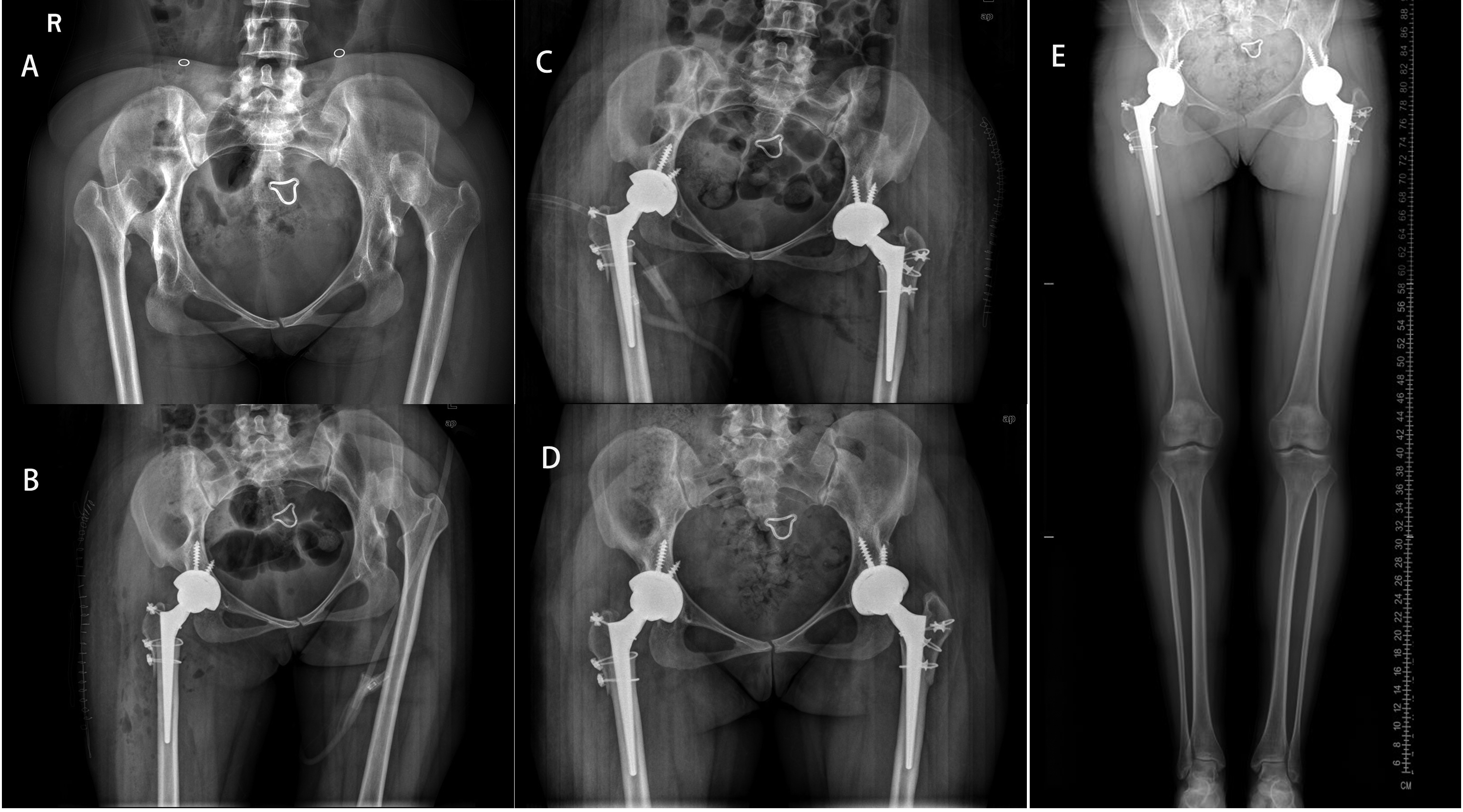
A 53-year-old woman with right high congenital hip dislocation underwent a cementless total hip arthroplasty using treated with trochanteric slide osteotomy: (A) the preoperative radiograph; (B) immediate postoperative of right side: the osteotomy fragment was fixed with trochanteric plate and the proximal femoral was treated with cerclage fixation (C) 8 months postoperatively on the right side: The osteotomy of greater trochanter resulted in nonunion with screw fracture and plate displacement; (D-E) 12 months Postoperative X-ray follow-up (3 months after the internal fixation was removed): there was no bony union but no obvious displacement of the greater trochanter; (F) 18 months postoperative follow-up: the patient had good hip motion and no lameness.
One case (3.2%) of medial femoral cortical fracture occurred during the implantation of a Wagner cone stem in a patient of his left hip. Intraoperative cerclage fixation was given. At 12 weeks after operation, the fracture healed without displacement of the prosthesis stem. Two patients (6.5%) showed early symptoms of sciatic palsy. They had mild signs of sciatic nerve irritation (paresthesia in the ipsilateral foot and a decrease in dorsal extensor muscle strength). Both patients recovered completely and their symptoms disappeared 6 months after surgery. The anterolateral X ray was used to evaluate the healing of the osteotomy site. The current consensus that the gap less than 15 mm for fibrous healing, larger than 15 mm gap is considered non-healing [8]. There was bony union in 26 hips (83.9%), fibrous union in four (12.9%), and non-union in one (3.2%) (see Fig. 4). No infection or deep venous thrombosis were detected.
THR is the ultimate treatment for high dislocation of DDH, Due to the high technical requirements of surgery, there is a high incidence of complications. The most frequent complications are LLD, intra-operative femur fractures, delayed union or non-union of the osteotomy site, neurovascular injury, and implant failure [9, 10]. The methods of femoral osteotomy and the selection of the stem have been thoroughly studied in the previous literature [11, 12]. In this study, the functional scores and complications of Crowe type IV DDH surgery cases who underwent reconstruction using TSO combined with a Wagner cone stem were analyzed retrospectively.
LLD is an especially common complication in patients who present with a severe unilateral dislocation [9]. In patients with Crowe type IV DDH, LLD manifests in several different ways, including bony LLD, functional LLD, and anatomical LLD. Bony LLD can be effectively balanced by TSO, in which a trial reduction of the hip is usually performed to assess the stiffness of the circumarticular soft tissue and check limb length. The TSO technique has the advantage of maintaining limb balance. Oblique osteotomy of the greater trochanter is equivalent to loosening the muscle groups attached to it, including the lateral thigh muscles; more importantly, it relieves the difficulty of reduction caused by the high middle gluteal muscle tension due to abnormal development, which provided better control on the amount of proximal femur osteotomy. In the present study, LLD improved significantly in all cases, with an average LLD of 10 mm (range 8–12 mm). Studies have reported LLD greater than 5 mm can affect the prognosis, and greater than 10 mm can cause gait asymmetry [9, 13]. However, to protect the sciatic nerve, the length of the limb is often compromised during THR in cases of high dislocation or extensive soft tissue contracture. Edwards et al. showed that the preoperative LLD of more than 40 mm increased the risk of nerve damage. In our present study, the average pre-operative LLD was 51 mm (range 46–58 mm), and all the patients presented a pre-operative LLD greater than 40 mm. However, only two patients (two hips, 6.5%) experienced sciatic nerve palsy, both of whom completely recovered within 6 months after conservative treatment.
Despite these results, it should be recognized that if the surgical leg is extended by more than 40–45 mm, the risk of sciatic nerve paralysis increases. As a result, additional osteotomies are often recommended for the consideration of nerve strain during THR. However, TSO with greater trochanteric osteotomy can achieve sufficient muscle tissue release and better exposure on both the acetabular and femoral side during surgery, which can minimize the occurrence of these conditions.
The Trendelenburg sign is an important index to evaluate the abductor strength of the HIP, in this study, 25 cases (86.2%) showed significant improvement. TSO can preserve the musculo-osseous-muscular sleeve hip abductors and maintain the continuity of the greater trochanter and vastus lateralis. After TSO, the tension of the gluteus medius can be adjusted by fixation of the osteotomy block via titanium cables. This technique has been shown to improve hip abductor biomechanics and hip joint stability by increasing abductor length and arm strength [12]. Furthermore, subtrochanteric osteotomy is mainly based on the overall soft-tissue tension around the hip joint to adjust the length of the cut bone, and then achieve the purpose of reduction. It cannot easily adjust the moment arm or tension of the hip abductors, such as the gluteus medius. Therefore, compared with subtrochanteric transverse osteotomy, TSO may have more advantages in controlling limb length and post-operative gait.
Femoral abnormalities increase the risk of intra-operative femoral fracture, the incidence of which has been found to range from 6% to 14% [9]. In the present study, one patient suffered a proximal femoral fracture during femoral prosthesis implantation, and the maximum press-fit was still achieved after cerclage fixation, and good results were obtained after follow-up.
One of the major causes of intraoperative femoral fractures is the mismatch between the femoral stem and the femoral medullary cavity due to the anatomical dysplasia of the femur. Ollivier et al. reviewed 28 cases of cementless THR in patients with Crowe IV type DDH and found that intraoperative fractures occurred in 5 of 28 hips (17.8%) [15]. However, these fractures were managed properly, with no sequelae or new problems. Although successful management of the fracture does not affect the clinical outcome and survival of the implant, it is suggested that a cerclage band can be prophylactically placed before implant insertion.
Although THR is currently regarded as the gold standard treatment in end-stage hip disorders, performing THR in patients with Crowe type IV DDH is still technically demanding due to abnormal proximal femoral morphology and poor bone stock, especially when treated with a metaphyseal-fitting flat-wedge taper or fit and fill stem [13]. In these situations, a diaphyseal engaging stem that preserves bone stock and allows for the creation of the desired amount of anteversion is desirable [16]. The Wagner cone is a short diaphyseal engaging femoral stem, with a 5
In a recent retrospective study, no cases required revision for aseptic loosening or subsidence of the stem in those THRs of proximal femoral anatomic deformity using Wagner cones during mid-term follow-up [16]. In the present study, a Wagner cone femoral stem was used in all THRs, and no cases of aseptic loosening or subsidence were observed during follow-up. The loosening rate and sinking rate of the prosthesis were found to be significantly reduced due to the fact that a Wagner cone femoral stem can be directly fixed to the femur in the lower segment of the osteotomy. Furthermore, the rotational stability between the prosthesis and the distal end of the osteotomy can be easily controlled. Due to this, the Wagner cone femoral stem could go deeper into the femur than other types of stem used in subtrochanteric TSO, granting better initial stability.
Non-union of the greater trochanter after TSO in THR is another issue that needs to be addressed. In the present study, 96.8% of the reattached osteotomy sites healed within 6 months of surgery, and non-union was observed in only one case. However, there was no gluteus medius gait in this case. This may have been due to the fibrous healing not affecting, or even interfering with, the abductor muscle group, especially the gluteus medius. Despite this, the patient was satisfied with the resulting hip function.
The incidence of nonunion at the osteotomy site has been reported as ranging from 0% to 22%, which can lead to varus angulation, unstable rotation, pain, and loosening of the prosthesis [17, 18]. The following three factors are considered to be the most important factors for instability of the osteotomy site [3]: lower rotational stability, fixation method, and morphology of the femoral stem. Transverse subtrochanteric femoral shortening osteotomy has been reported as having lower rotational stability than other techniques, such as oblique, step-cut, and chevron osteotomies [3, 4]. However, a comprehensive meta-analysis reported no significant difference between transverse subtrochanteric femoral shortening osteotomy and modified methods in terms of complications and survival rates [19]. TSO is a simple technique to adjust the tension of the gluteus medius. It was therefore combined with a shortening osteotomy of the proximal femur in the present study as a feasible mechanism to shorten the femur, control the length of the limb, and adjust the abductor muscle. Regarding fixation method, TSO can preserve the integrity and continuity of the femoral medullary cavity. Compared with most modified subtrochanteric femoral shortening osteotomy techniques, it is easy to control rotation instability during TSO. It differs from subtrochanteric osteotomy in that the distal of the femur is treated as a whole, so the lower femur can be directly polished and tested following TSO. Furthermore, it is more convenient and comfortable to place the femoral stem prosthesis via TSO. Finally, regarding the morphology of the femoral stem, a cylindrical stem can allow the surgeon to create the optimal anteversion for stability, so a cementless femoral conical stem is recommended.
Although these three aspects were taken into consideration during the surgeries performed in the present study, fibrous union and non-union were still observed. However, during follow-up it was found that the fibrous scar connection of the osteotomy did not cause pain in the osteotomy area when walking and did not affect post-operative hip function (see Fig. 4). These results are consistent with the research of Lee et al. However, long-term follow-up results need to be sought for further clarification of these results.
This study also has some other limitations, the number of cases is relatively limited, the follow-up time may not be long enough, and for some cases that require more proximal femoral osteotomy, how to ensure the initial stability of the prosthesis, or perhaps to choose some other customized personalized prosthesis, all these are we need to face and further think about in the future.
Conclusion
TSO combined with a cementless femoral conical stem is a suitable option for THR in patients with Crowe type IV DDH. The occurrence of complications should be paid more attention, the correct operative technique and the appropriate selection of prosthesis implantation are the important guarantee for the success of the operation.
Ethics approval and consent to participate
Approval was obtained from the Ethics Committee of First People’s Hospital of Wenling (KY-2015-1012-01). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
The study was funded by the Medical Science and Technology Program of Zhejiang Province (2022KY447).
Footnotes
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.