
Abstract
BACKGROUND:
The gait ability of stroke patients is highly related with trunk control. Studies that addressed the effects of trunk control training using visual feedback on gait parameters of stroke patients are lacking.
OBJECTIVE:
The purpose of this study was to investigate the role of smartphone-based visual feedback trunk control training for improvement of trunk control and spatio-temporal gait parameter in stroke patients.
METHODS:
Twenty-four stroke patients participated in this study. Participants were randomly allocated to the experimental and control groups. Both groups completed conventional rehabilitation over 4 weeks. The experimental group additionally received smartphone-based visual feedback trunk control training for 4 weeks. The primary outcome of this study was evaluated by trunk impairment scale and spatio-temporal gait parameters.
RESULTS:
The trunk impairment scale in the experimental group was significantly improved compared to the control group (
CONCLUSIONS:
Additional smartphone-based visual feedback trunk control training may improve trunk control and spatio-temporal gait parameter in chronic stroke patients.
Introduction
The majority of stroke patients have limited gait abilities including an increased double support phase, abnormal movement of the hips, knee, ankle and pelvis, and a decreased walking speed [1, 2, 3, 4]. The significantly reduced gait abilities of stroke patients represent a large barrier to independently performing daily activities [5]. Therefore, the restoration of efficient and independent gait ability is a primary therapeutic goal for stroke patients [6].
Gait ability is strongly related to trunk control [7], defined as the ability of the trunk muscles to allow the body to remain upright and to adjust to weight shifts after a stroke. In order to maintain balance while walking, the pelvis and upper body normally move from side to side in time with the weight-bearing limb. Trunk control is an important factor in gait training, and trunk kinematics [8] and trunk muscles [9] are related to gait speed, and a greater pelvic range of motion has also been linked to longer stride lengths [8]. In addition, trunk control function is an important early predictor of activities of daily living in stroke patients [7]. In particular, decreased trunk control is observed in stroke patients compared to healthy people [10]. In stroke patients, trunk control is reduced by trunk muscle weakness and proprioceptive sensory deficits. This reduction in trunk control also affects the gait ability of these patients [11, 12]. Although trunk control after a stroke is an important factor in rehabilitation, most previous studies have focused on limb rehabilitation only [11, 13].
Several training methods regarding trunk control have been researched, these include weight-shift training on an unstable surface [14], trunk muscle strengthening exercises [15], and task-related trunk training [16]. However, most of these studies investigated the effect of trunk control training on trunk performance, and studies investigating the effect of trunk control training on spatio-temporal gait variables of stroke patients are limited.
There has been a recent worldwide increase in the use of smartphones with substantial computing function and built-in sensors, such as accelerometers and gyroscopes, as well as the use of smartphones in healthcare settings [17, 18]. A previous study reported that a smartphone can provide a guideline for the treatment of acute stroke and facilitate the diagnosis of stroke [19]. In another previous study, a smartphone was shown to help to determine neurological damage via a built-in smartphone sensor [20]. Smartphones can also be used to remotely diagnose acute stroke [21]. Although the applications of smartphones for stroke have gradually increased, most previous studies have focused on delivering information on the diagnosis, symptoms, and pre-hospital care elements of stroke.
Visual feedback is provided as postural change information for the patients in real time during postural training, and patients can control and maintain their posture in this manner [22, 23]. In addition, most smartphones can recognize changes in user motion using built-in sensors such as accelerometers and gyroscopes. Therefore, we developed a smartphone-based visual feedback trunk control training system for trunk control training in stroke patients. Hence, the purpose of this study was to introduce a smartphone-based trunk control training system for stroke patients and to investigate the role of a smartphone-based visual feedback trunk control training (SPVFTCT) system for the improvement of trunk control and spatio-temporal gait parameters in stroke patients.
Materials and methods
Subjects
Twenty-seven patients who had experienced a chronic stroke were recruited for this study from the O-Memorial Hospital in Seoul, Korea. Participants were screened according to the inclusion and exclusion criteria. The inclusion criteria were as follows: hemiparesis for more than 6 months, resulting from a single stroke; the ability to walk with and without the use of an assistive device for 10 m; the ability to understand and follow simple verbal instructions (Korean version of Mini-Mental State Examination score
Procedure
This study was designed as a single-blind randomized controlled trial. The sample size of this study was calculated by G-Power 3.19 software. The alpha error probability and power were set as 0.05 and 0.8, respectively, and the effect size was set at 1.05, based on a prior pilot test; as a result, the sample size was 12 patients per group. Twenty-four participants were randomly allocated, by random allocation software, to either the SPVFTCT (
Flow diagram of experimental procedure.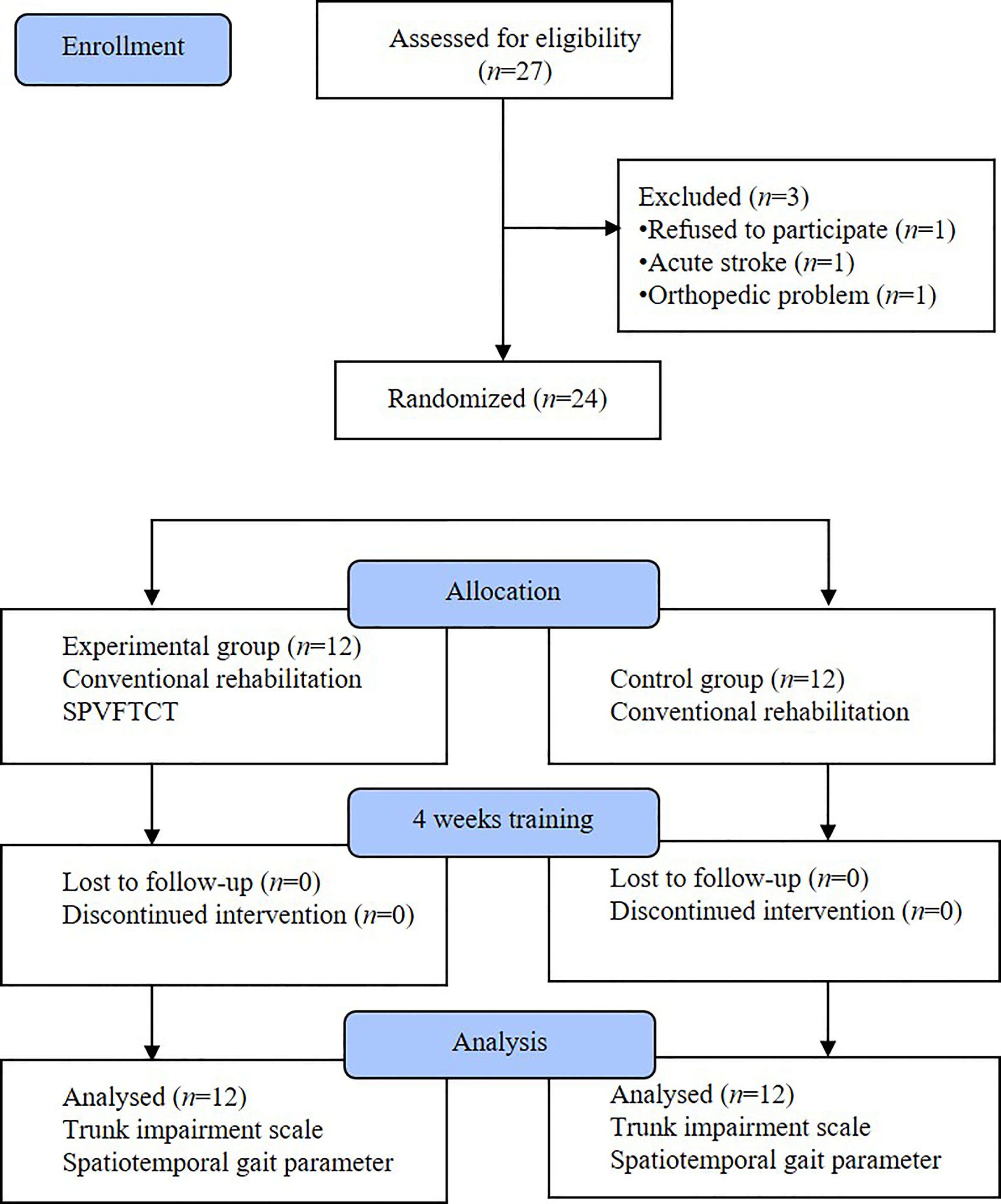
Smartphone inserted balance board.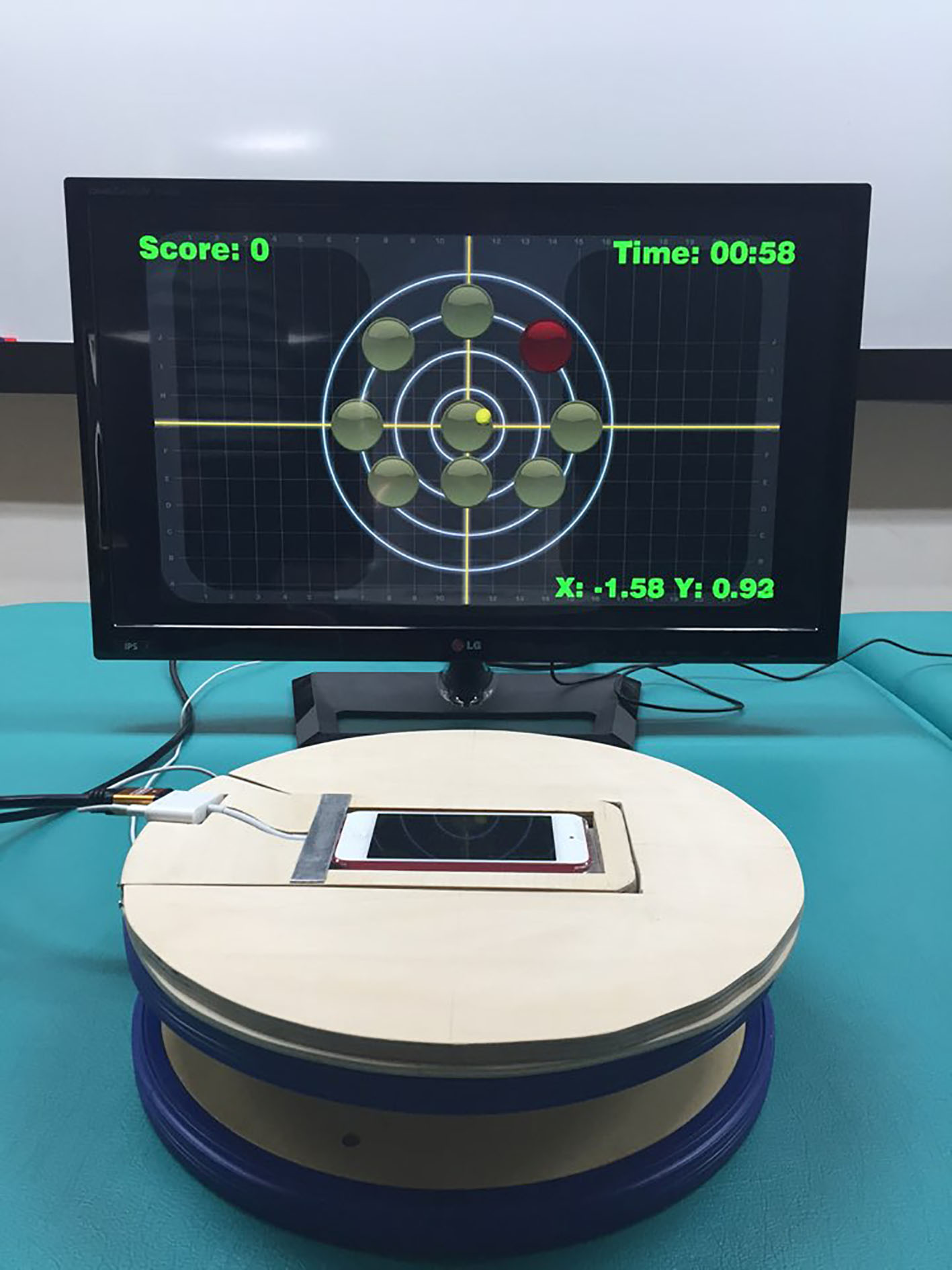
Smartphone-based visual feedback trunk control training.
Smartphone application.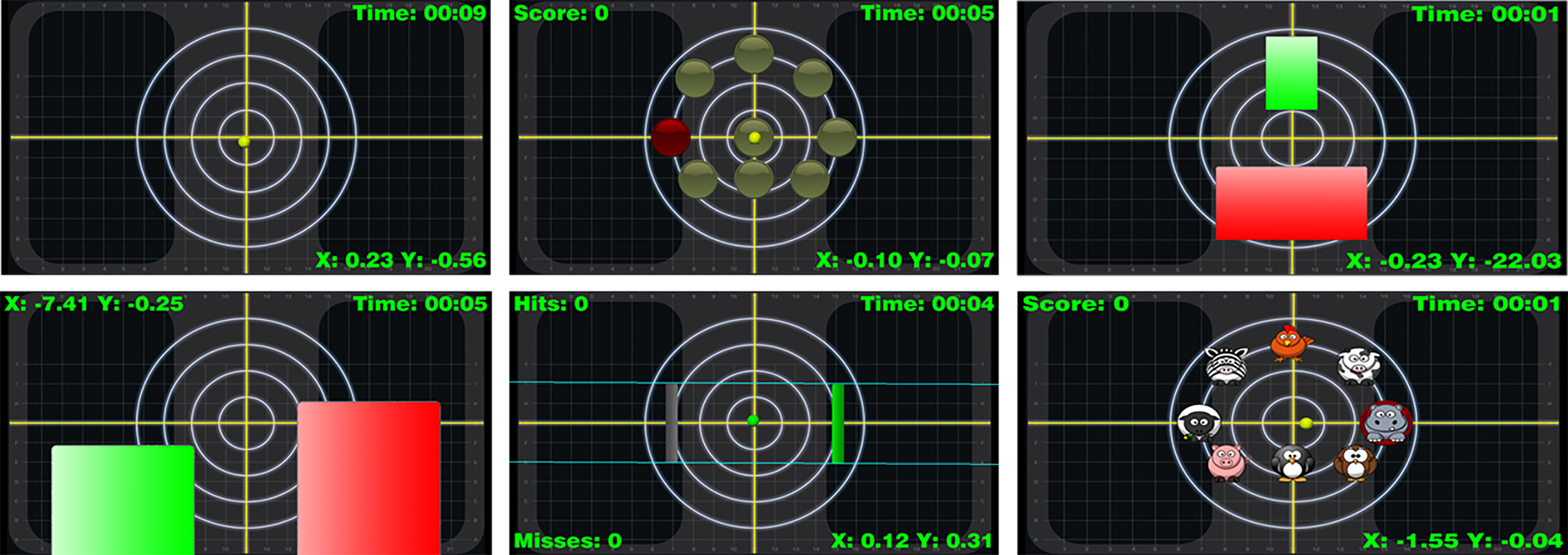
In this study, a SPVFTCT system was developed for visual feedback trunk control training of stroke patients. The SPVFTCT system consisted of a smartphone (iPhone 5, Apple, USA, 2013) inserted balance board (Pedalo balance top), monitor, speaker, and smartphone applications (Fig. 2). The smartphone in the balance board was connected with the monitor and speakers. During trunk control training, the smartphone transferred video and audio data from the smartphone application to the monitor and speakers, respectively, using mirroring technology. For trunk control training, the participants sat 1–1.5 m away from the monitor on a smartphone-inserted balance board. The participant’s hip and knee joints were flexed at 90
Smartphone applications were used to train trunk control in stroke patients; the inbuilt gyroscope allowed these applications to recognize the changes in trunk movements. The smartphone applications were as follows: CSMi Center of Pressure, CSMi Limits Of Stability, CSMi Weight Bearing Front-Back, CSMi Weight Bearing Left-Right, CSMi Weight Shift, and CSMi Animal Adventure (Computer Sports Medicine, Inc., Apple App store) (Fig. 4). These applications measure the center of pressure, and the static and dynamic stability of the trunk movements of the participants in various directions. In addition, these applications encourage the participants to move their trunk in various directions. For each patient, the smartphone applications were applied by adjusting the level of difficulty according to his or her trunk control ability. To prevent loss of concentration as a result of external interference, the trunk control training was performed in a dedicated room.
Conventional rehabilitation program
The conventional rehabilitation program consisted of patient-specific physical and occupational therapy, and functional electrical stimulation (FES). Neurodevelopmental treatment and proprioceptive neuromuscular facilitation were performed during each physical therapy session. Occupational therapy, or functional exercise of the upper extremities with the intention to improve the activities of daily living, was also performed. FES was applied to the lower extremities each day. Neurodevelopmental treatment, proprioceptive neuromuscular facilitation, and occupational therapy were conducted for 30 min, and FES therapy was conducted for 20 min. The conventional rehabilitation programs were conducted five times a week for 4 weeks.
Measurements
The trunk impairment scale (TIS) was used to measure the trunk control ability of chronic stroke patients. The TIS consists of three subscales: static sitting balance (3 items), dynamic sitting balance (10 items), and coordination (4 items). The TIS scores range from a minimum of 0 to a maximum of 23, with lower scores indicating a worse trunk performance. Subjects were asked to sit on the treatment table in order to evaluate the TIS score.
To evaluate gait ability, subjects were asked to walk on a walkway at a self-selected comfortable velocity. The subjects were instructed to walk from 3 m in front of the walkway until 2 m beyond its end, after which they were instructed to turn around and walk back to the starting point. The spatio-temporal gait variables of the subjects were evaluated using the OPTOGait system (Microgate S.r.I, Italy), which allows the quantification of spatio-temporal gait parameters on basically all flat surfaces. The OPTOGait system uses transmitting and receiving bars placed in parallel; when a subject passes between the transmitting bar and the receiving bar, the system detects any interruption in the light signal as a result of the presence of feet within the recording area, and automatically calculates the spatio-temporal gait parameter. The method has high concurrent validity and test-retest reliability compared to the GAITRite system, a conventional instrumented walkway system for over-ground walking [25]. Data were extracted at 1000 Hz and saved on a PC using OPTOGait Version 1.6.4.0 software (Microgate S.r.I).
Statistical analysis
The Shapiro-Wilk test was used to test variables for normality, and an independent
Results
In total, 27 participants were recruited for this study, and all participants completed 4 weeks of training without drop-off. No significant difference was found in the general characteristics of participants between the SPVFTCT group and control group (Table 1).
Characteristics of subjects in the experimental and control groups
Characteristics of subjects in the experimental and control groups
Values are expressed as mean (standard deviation).
The TIS was significantly higher in the SPVFTCT group after 4 weeks intervention (
Comparison of trunk performance within and between groups
Values are expressed as mean (standard deviation). SPVFTCT: smartphone-based visual feedback trunk control training, TIS: trunk impairment scale.
Comparison of spatial gait parameters within and between groups
Values are expressed as mean (standard deviation).
Comparison of temporal gait parameters within and between groups
Values are expressed as mean (standard deviation).
After training, spatial gait parameters, including stride length and step length, were significantly higher in the SPVFTCT group than the control group. In addition, the step width was significantly lower in the SPVFTCT group than the control group following training (Table 3). The temporal gait parameters, including velocity and cadence, were significantly higher in the SPVFTCT group than the control group. On the contrary, the stride time, step time, and the duration of double-limb support were significantly lower in the SPVFTCT group compared to the control group (Table 4).
In this study, we developed a visual feedback trunk control training system in order to improve the trunk control ability and spatio-temporal gait parameters of stroke patients using a smartphone, mirroring technology, and smartphone applications. After 4 weeks of training, the SPVFTCT group demonstrated improvements in trunk control ability and spatio-temporal gait parameters.
At the end of the 4 week training, patients in the SPVFTCT group demonstrated improved TIS scores. The improvement in the TIS score was considered to be associated with the improved trunk mobility of subjects in the SPVFTCT group, as the smartphone-based visual feedback trunk control training provided information about the center of pressure in the sitting position. The awareness of the center of pressure by this SPVFTCT system has the potential to improve proprioception in the sitting position. The subjects in the SPVFTCT group were asked to sit on a smartphone inserted balance board and either move or maintain the center of their body pressure using their trunk and pelvic movement in various directions, including the affected and non-affected side, during SPVFTCT. These movements may have contributed to the improved trunk control ability of the subjects in the SPVFTCT group. The smartphone applications used in this study induced patients to maintain the center of their body pressure and move their trunk and pelvis during SPVFTCT. The results of this study are similar to those of previous studies [14, 26].
The improvements of temporal gait parameters, including velocity, cadence, step time, stride time, and the duration of double-limb support, were associated with increases in the gait speed of stroke patients. Verheyden et al. [7] reported that trunk performance was significantly correlated with gait speed. Furthermore, Tyson [27] reported that lateral trunk movements were significantly correlated with gait speed, and Jung et al. [14] reported that trunk control training for 4 weeks improved the gait speed in stroke patients. Similarly, in this study, the improvements in temporal gait parameters were considered to be associated with the improvement in trunk performance caused by SPVFTCT. In addition, SPVFTCT was performed in various directions, including lateral movements; the improvement in lateral trunk movement, which is significantly correlated with gait speed, was considered to improve the temporal gait parameters of stroke patients.
In this study, spatial gait parameters, including step length and stride length, were significantly increased in the SPVFTCT group. Saeys et al. [28] reported that additional trunk exercises have a beneficial effect on trunk function and lower extremity mobility in people after a stroke. Trunk muscle activity is best described as the pre-programmed integration of local single- and multi-joint muscles to provide stability and produce motion; this results in proximal stability for distal mobility and a proximal-to-distal pattern of force generation [29]. Likewise, improvements in trunk control and stability following SPVFTCT may result in increased lower limb mobility. The increases in step length and stride length in this study may be associated with the improved lower limb mobility of stroke patients, as a result of improved trunk control and stability following SPVFTCT.
Trunk exercises significantly improve the standing balance of stroke patients [28, 30]. Gabell and Nayak [31] reported that step width is related to balance control and that an increase in step width is related to a compensation for instability. In this study, the step width was significantly lower in the SPVFTCT group compared to the control group; this may indicate that the improvements in standing balance following SPVFTCT may facilitate a decrease in step width in stroke patients.
The results of this study indicate that the SPVFTCT system may effectively improve the trunk control ability and spatio-temporal gait parameters of chronic stroke patients. The force-plate system and commercial videogame system, such as Nintendo Wii and PlayStation, have been used to provide visual feedback information to the stroke patients [32, 33, 34]. However, the force-plate system is expensive to build, and commercial videogame systems are not easy to use in stroke patients. However, the visual feedback trunk control training system in this study is easily equipped with a smartphone, monitor, and balance board. In addition, there are no additional costs involved in equipping the trunk control system due to the use of the patients own smartphones and monitors. Furthermore, the smartphone applications used in this study are intuitively designed and are easy to operate. Due to the characteristics mentioned above, the smartphone-based visual feedback trunk control training system using smartphones may be appropriate for use in stroke patients. This study successfully identified the effects of visual feedback training to improve the trunk control ability of stroke patients. Trunk control ability in stroke patients is not easy to recognize due to the difficulty in seeing and feeling their trunk movement. In this situation, the smartphone-based visual feedback training could help to improve the trunk control ability of stroke patients. In addition, we found that the improvement in the trunk control ability also lead to an improvement in the gait ability of stroke patients. Therefore, in clinical practice, it may be helpful to provide visual feedback trunk control training to improve the gait ability of stroke patients.
In this study, the control group showed no significant changes in trunk control and gait ability. This may be because 4 week training time was not enough to improve their trunk control and gait ability compared to the SPVFTCT group, which additionally received visual feedback trunk control training. Taken together, these results suggest that additional visual feedback trunk control training may reduce the treatment time required to improve trunk control and gait ability compared to the conventional rehabilitation program alone.
Although, the SPVFTCT system effectively improved the trunk control ability and spatio-temporal gait parameters in chronic stroke patients, there are some limitations in generalizing the effects of the SPVFTCT system. First, the sample size was small, and second, the total training times of the SPVFTCT and control groups were not equal. Therefore, further studies including large sample sizes and equal total training times are needed to generalize the effects of the SPVFTCT system on the spatio-temporal gait parameters in stroke patients.
Conclusion
The purpose of this study was to introduce a SPVFTCT system for use in stroke patients, and to investigate the role of the SPVFTCT system for the improvement of trunk control and spatio-temporal gait parameters in stroke patients. The results of this study indicate that the SPVFTCT system is effective in improving the trunk control ability and spatio-temporal gait parameters of chronic stroke patients. The advantage of this SPVFTCT system is that it can be easily used, in combination with a smartphone, to build a visual feedback training environment to help trunk control and gait of stroke patients. Furthermore, additional visual feedback trunk control training may reduce the treatment time needed to improve the trunk control and gait ability of stroke patients. Further studies, including larger sample sizes and equal total training times between the SPVFTCT and control group, are required in order to generalize the effects of the SPVFTCT system.
Footnotes
Acknowledgments
This work was supported by the Kyungnam University Foundation Grant 2018.
Conflict of interest
The authors have no conflict of interest to declare.