
Abstract
BACKGROUND:
Severe acetabular bone loss in revision total hip arthroplasty (RTHA), both with or without pelvic discontinuity, remains a great challenge in orthopaedic surgery.
OBJECTIVE:
The aim of this study was to evaluate risk factors for failure of custom-made acetabular implants in RTHA.
METHODS:
Seventy patients with severe acetabular bone loss (Paprosky Type III) and pelvic discontinuity, who required RTHA, were included in our study. All prostheses were constructed based on a thin-layer computed-tomography (CT) scan of the pelvis. The treatment was considered unsuccessful in the event of periprosthetic joint infection (PJI) or aseptic loosening (AL) with need for explantation of the custom-made acetabular implant.
RESULTS:
The average follow-up was 41.9
CONCLUSION:
Risk factors for treatment failure were a previous PJI, additional revision of femoral component, rheumatoid disease, elevated preoperative CRP and low preoperative haemoglobin. Awareness of these risk factors will help to improve future treatment standards.
Keywords
Introduction
Total hip arthroplasty (THA) is currently the most successful and frequent performed orthopaedic joint replacement surgery in patients with osteoarthritis of the hip and failed conservative treatment. Worldwide, over 1 million total hip arthroplasties are performed per year [1]. Nevertheless, a major complication after THA is loosening of the acetabular component with need for revision surgery. The subsequent loss of periacetabular bone stock remains the main problem in acetabular revision surgery [2, 3]. In severe cases implantation of a custom-made implant as an individualized treatment strategy is necessary. Treatment failure might necessitate a permanent girdlestone arthroplasty, especially in old and multimorbid patients.
To date, several studies have analysed risk factors for treatment failure after primary or revision total hip arthroplasty (RTHA) and could outline several factors e.g. previous PJI as indication for revision arthroplasty, age, obesity, preoperative anaemia or rheumatoid arthritis as host related factors [4, 5, 6]. Knowledge of these factors is essential, not only to inform the patient, but to optimize treatment in RTHA.
Although previous studies have described the use of custom-made implants, data analysing the specific risk factors for treatment failure in patients with need for a custom-made acetabular reconstruction are not described in literature [7, 8, 9]. The aim of this study was to identify possible risk factors that increase the risk of treatment failure. Our hypothesis was that treatment failure often occurs in patients with need for a custom-made implant due to a PJI, need for revision/implantation of the femoral component, a previous polymicrobial PJI (with or without detection of “difficult-to-treat” (dtt) pathogens [10, 11]) and that in addition certain (patient-specific) risk factors, such as age, a high BMI, an elevated C-reactive protein (CRP) and a low haemoglobin prior to surgery or rheumatoid arthritis (RA) favour treatment failure.
Material and methods
We performed a single-center, retrospective study including 70 consecutive patients between December 2008 and December 2018 with a Paprosky III periacetabular defect. Seventy patients were included in our study. See Table 1 for descriptive data of all patients.
In 30 of the patients, only the acetabular component was replaced during revision surgery, while in 40 of the patients, both the femoral and acetabular components had to be revised.
For 41 (58.6%) of the hips, the reason for revision surgery had been aseptic loosening of the previous acetabular component. In the other 29 (41.4%) hips, revision surgery had been due to PJI that had necessitated a two- or multi-staged procedure. In total, the mean number of previous hip surgeries for any reason before implantation of the custom-made implants had been 4.8 (range 1–43; 95% CI 3.5–6.5).
Inclusion criteria were the need for revision surgery in cases of severe periacetabular bone defects and the unfeasibility of biological downsizing or the use of standard implants, such as a cranial sockets or a modular revision system. The study was approved by our local institutional review board (Institutional Ethics Committee, No. 226/13). Patients with a severe periacetabular bone defect after explantation of the inlying prostheses due to a PJI were treated according to Wimmer et al. [12]. To exclude a persisting PJI, reimplantation was only performed after open revision with sampling and negative histopathological and microbiological evaluation. In patients with an aseptic loosening and removal of the acetabular component the remaining bone stock was protected by a large liner on the femoral component in between until replantation of the custom-made acetabular implant.
Descriptive summary of the clinical and laboratory data at admission (
) and, for haemoglobin only, also postoperatively (
)
Descriptive summary of the clinical and laboratory data at admission (
A thin-layer CT scan was performed preoperatively to acquire detailed planning shots. The custom-made implants used in this study were manufactured by Peter Brehm (
Clinical and radiographic follow-up assessments were performed postoperatively at six weeks, six months, one year, and thereafter in 1-year intervals. The Harrison Hip Score (HHS) and the Visual Analogue Scale (VAS) were assessed preoperatively and again postoperatively at six weeks and at final follow-up [13]. The evaluation of the pre- and postoperative radiological imaging was carried out by three independent examiners in respect to new osteolysis, significant or progressive radiolucent lines in comparison with previous images, changes of the Center of rotation (COR) and migration of the acetabular or femoral prosthesis component.
The definitions of the THA complications workgroup were used to evaluate postoperative complications [14]. Treatment failure was defined as an increasing change of the COR (
Our endpoint was a successful implantation of the custom-made implant with absent of signs of implant dislocation, respectively migration as described by Roessler et al. or signs of infection at last follow-up [15]. According to our outcome analysis we defined two groups (“treatment success group” vs. “treatment failure group”) to determine risk factors for a failed procedure in terms of treatment failure with need for explantation of the inlying custom-made implant.
Statistical analysis
Data was collected in Microsoft Excel 2016 (Microsoft Corporation, Richmond, USA). Statistical analysis was carried out with SPSS statistics 25 for Windows (SPSS Inc, Chicago, IL, USA). Descriptive statistics, including arithmetic mean value and standard deviation were calculated. Data are given as means
For statistical analysis, the nonparametric Mann-Whitney U test was performed for metric, not normally distributed, whereas Student
The phi coefficient was used to measure the association for two binary variables. Effect size (r; small effect:
Results
The mean follow-up was 41.9
Summary of the clinical and laboratory data including Visual Analogue Scale (VAS), Harrison Hip Score (HHS) preoperative and at last follow-up (PJI: periprosthetic joint infection; AL: aseptic loosening)
Summary of the clinical and laboratory data including Visual Analogue Scale (VAS), Harrison Hip Score (HHS) preoperative and at last follow-up (PJI: periprosthetic joint infection; AL: aseptic loosening)
ROC analysis revealed a cut-off value of 15.2 mg/l [AUC: 0.7; Sensitivity: 86.8%, Specificity 64.7%; reference:
Scatterplots of the patient-specific risk factors age, Body Mass Index, C-reactive protein (CRP) and preoperative haemoglobin.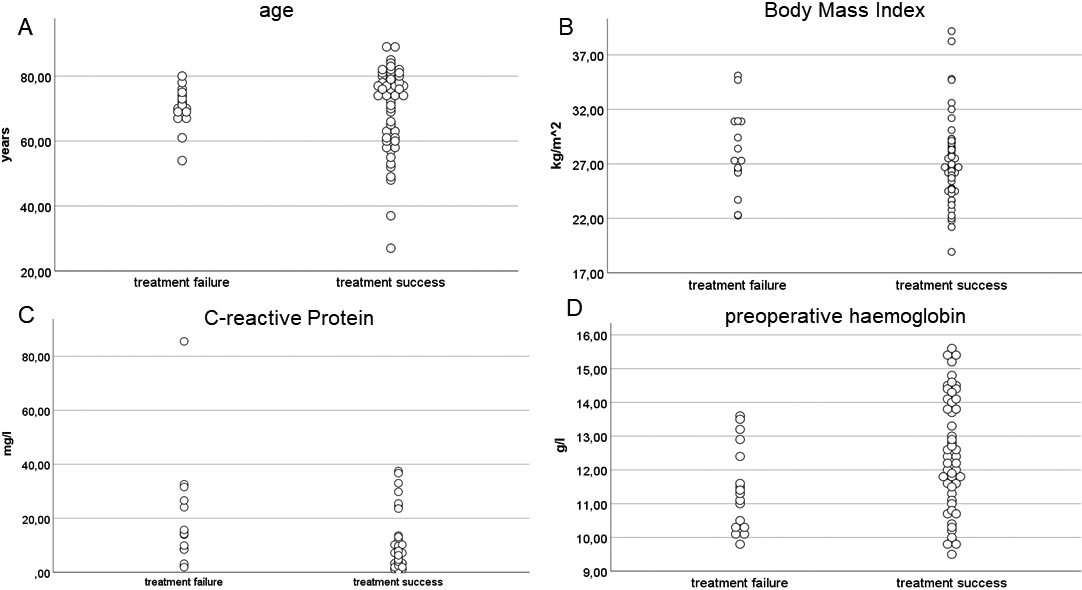
Failed RTHA. Radiological follow-up before implantation of a custom-made acetabular component (A), before explantation due to a chronic PJI with consecutive loosening (B) and after explantation at last follow-up (C).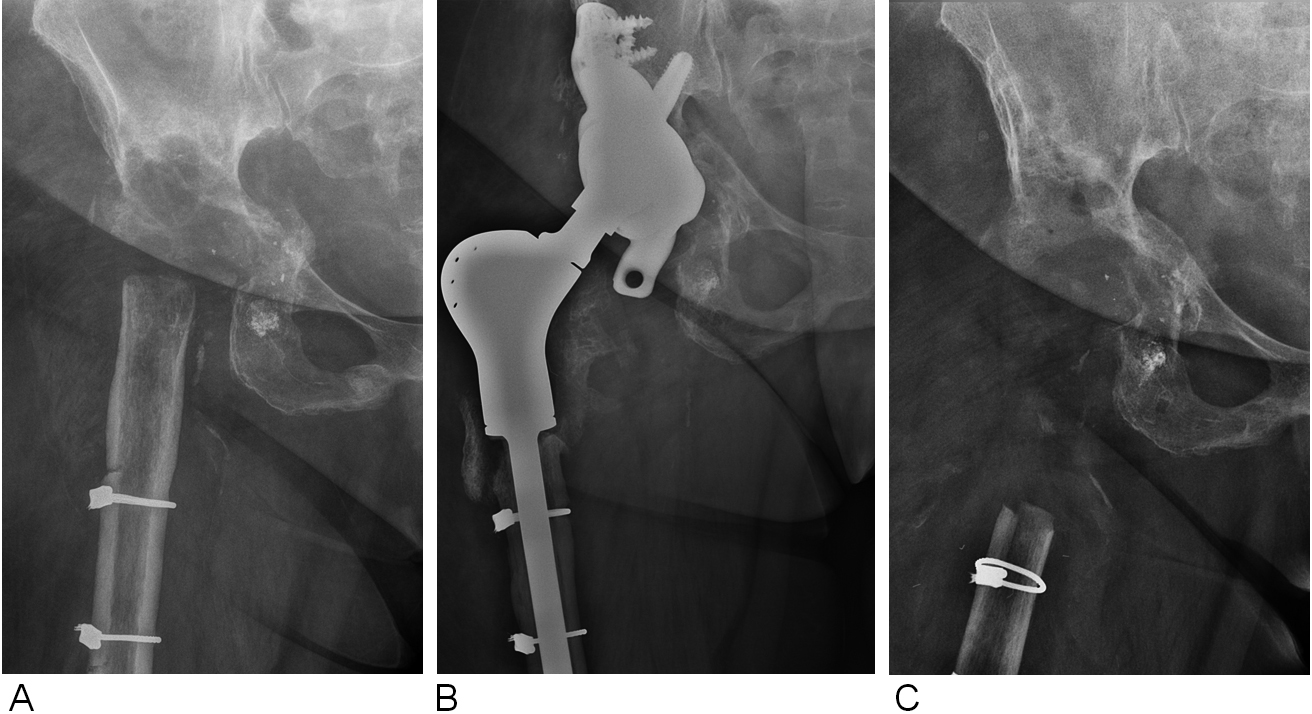
Among the included 70 patients explantation was necessary in 17 cases (24.3%), whereas in 53 cases (75.7%) clinical and radiological follow-up showed a good clinical function and a stable inlying protheses without vertical or horizontal migration, screw breakage or signs of infection. Figure 2 depicts exemplary the situation before RTHA and after explantation.
Fifteen patients out of these 17 cases needed explantation of the custom-made implant because of PJI, and the remaining 2 patients needed explantation because of aseptic loosening of the implant.
Ten out of these 15 patients presented themselves after dismission with a chronic PJI (duration of symptoms
On average, explantation due to PJI had been performed after 40.2
Table 3 shows the analysed categorial variables for treatment failure. Significant potential risk factors for treatment failure were the following: PJI as reason for RTHA [
Statistical evaluation of categorial variables for treatment failure after revision total hip arthroplasty with custom-made acetabular implants (OR: odds ratio; CI: confidence interval; R: effect size; CMAI: custom-made acetabular implant; PJI: periprosthetic joint infection; dtt: “difficult-to-treat” pathogen according to the criteria published by Zimmerli et al. and Renz et al. [10, 11])
In our study, we investigated relevant risk factors for treatment failure in patients with need for a custom-made acetabular reconstruction after RTHA. The treatment failure rate with need for explantation of the custom-made implants was 24.3%. Our failure rates were thus higher than those published in comparable studies, which have described failure rates of 0% (Christie et al.), 11% (Wind et al.), and 12% (Taunton et al.) for custom-made implants [17, 18, 19, 20].
It is difficult to identify precisely why the failure rates in these studies were lower than in our study. A possible explanation might be that there was a selection bias in our study due to the relatively high percentage of patients (41.4%) who needed a custom-made implant after PJI in a two or multiple stage procedure after septic loosening of the previously inlying implant, although open revision with sampling did not show signs of a persisting infection.
Statistically significant risk factors in our study for treatment failure were a previous PJI as reason for RTHA, an additional revision of femoral component during implantation and rheumatoid disease. An elevated CRP and a low haemoglobin at admission as host related factors were additional risk factors for treatment failure. In contrast age, BMI, the number of previous surgeries, a previous polymicrobial PJI or a previous PJI with detection of “difficult-to-treat” pathogen as defined by Zimmerli et al. [10] and Renz et al. [11] did not differ significantly between our two groups (Tables 2 and 3).
Previous studies tried to define risk factors for PJI and subsequent treatment failure after THA, with partly inhomogeneous results [4, 6]. Described risk factors for PJI with subsequent treatment failure could not always be confirmed by others [4]. Fagotti et al. reported PJI as treatment indication for a RTHA as a risk factor for reinfection with treatment failure, which is in accordance with our results [21]. In this context there are no data available if revision of the femoral and acetabular component has a higher risk of PJI than the sole revision of one component. But it can be assumed that extended RTHA might be associated with a higher risk for treatment failure as reports for megaprostheses have indicated [22, 23]. Interestingly surgery times did not differ between our two groups. In contrast Hoberg et al. reported similar outcomes between two-stage revision for infection and aseptic hip revision arthroplasty [24].
In literature, an additional high risk factor for development of a PJI and subsequent failure is RA [25], which supports our results as 7 out of 17 (41.2%) were patients with RA. Due to our low number of patients with RA we did not investigate the influence of the different perioperative immunosuppressive medications such as steroids or biologic response modifiers.
Logroscino et al. reported an lower preoperative CRP in patients with a successful two-stage RTHA after PJI [5], which is supported by our results as those patients with a successful treatment showed a significant lower preoperative CRP than those with treatment failure after surgery.
An important factor in RTHA is the blood loss and thus the preoperative hemoglobin. In our study patients with treatment failure had a significant lower preoperative hemoglobin. In this context we must admit that an exact calculation of the total blood loss (intraoperative and postoperative over wound drainage) was not possible. Sharqzah et al. could show that blood loss and transfusion rates were higher in patients with need for a two-stage procedure than those undergoing a one-stage procedure [26]. This is relevant as Tornero et al. and Everhart et al. could demonstrate a dose dependent relationship between allogenic red blood-cell transfusion and risk of PJI after arthroplasty. Therefore best possible patient blood management might be a low risk but nevertheless effective option to alter this risk factor.
Tan et al. reported that RTHA after polymicrobial PJI or detection of a “difficult-to-treat” pathogen is associated with a higher treatment failure rate and need for explantation [27]. Our data support the fact that a previous PJI as reason for a custom-made RTHA is a related to a worse outcome in comparison. Nevertheless, we could not confirm that patients with a previous polymicrobial infection or detection of a “difficult-to-treat” pathogen have a higher risk of treatment failure and a potentially worse acetabular defect situation [28]. It has been described previously that number of revisions in patients undergoing RTHA by custom-made implants increases risk of failure exponentially [29].
Age and obesity have been described as independent risk factors for treatment failure after PJI in THA and RTHA [4, 5, 6]. Although we could not report an association between treatment failure and the BMI in our study. Obesity remains a challenging situation as higher surgical times and increased surgical incisions to gain the needed exposure have been reported [6]. Yet, altering this in contrast to the patients age modifiable factor could be helpful.
Our study does, however, have several potential limitations. The first limitation of our study is its retrospective design. A second limitation is that the sample size in our study was relatively small for a retrospective study, although we included all patients, who underwent RTHA over the course of 10 years in our tertiary endoprosthetic referral center. Nonetheless, our sample size easily equals that of comparable studies, so, to our best knowledge, our study still remains one of the largest studies in this thematic field to date. However, the study was intended to cover a reality-based patient selection without strong restrictions due to inclusion criteria or comorbidities.
Conclusion
The main complication of RTHA remains PJI with need for explantation. Previous PJI, additional revision of femoral component, rheumatoid disease, elevated preoperative CRP and low preoperative haemoglobin are risk factors for failure. Knowing these factors responsible for failure of custom-made acetabular implants could lead to a closer monitoring postoperatively and may, if possible, allow preoperative optimization.
Footnotes
Conflict of interest
None to report.