
Abstract
BACKGROUND:
Surgeons still face difficulties when performing aseptic acetabular revision on patients with extensive defects. Advances in three-dimensional printing technology (3DP) have afforded to the surgeons to create a patient-specific implant matching the morphology and topography of the defect.
OBJECTIVE:
The aim of the current research was to determine the survivorship in the treatment of acetabular bone defects with pelvic discontinuity (PD).
METHODS:
In order to reconstruct Paprosky type III defects with PD, twenty-three patients underwent revision total hip arthroplasty (THA) utilizing 3D-printed implants (Mobelife). The primary outcomes were the implant-associated failure rate correlated with survivorship. As secondary variables, complications and the effect of age, sex, comorbidities, history of infections and the presence of other lower limb arthroplasties on a new revision were analyzed.
RESULTS:
Patients were followed out to a mean of 67.22
CONCLUSION:
The use of 3DP patient-specific acetabular components has shown encouraging results and it is a viable treatment option for addressing acetabular defects with combined PD in aseptic THA revision.
Keywords
Background
Over six hundred thousand total hip arthroplasties (THA) are conducted every year in Europe and 1.4 million worldwide. These numbers are anticipated to grow considerably by 2030, and subsequently, the frequency of revision hip arthroplasty is also expected to rise [1, 2].
The Paprosky classification is a well-known system for categorizing acetabular bone loss in revision THA [3, 4]. Paprosky type III defects pose the greatest challenges in reconstruction. Effective management of such defects with associated pelvic discontinuity calls for meticulous surgical planning. The main goals entail reconstructing the anatomical hip centre and maintaining the continuity between the ischium and the ileum. Numerous options are available, and the optimal method will depend on the severity of the bone loss. These include the use of metal augments and antiprotrusio cages, oblong acetabular components, reconstruction cages with ischial or ilial screw fixation, structural allograft with plating, jumbo cups and triflange revision acetabular components [5, 6, 7, 8, 9, 10, 11, 12, 13, 14]. The range of surgical treatments that are available is indicative of how challenging this issue is to address. Currently, there is little evidence that any of these methods can consistently produce favourable outcomes, due to high failure rates and unsatisfactory survivorship [11, 15, 16, 17].
There are two main issues with using non-custom acetabular components in massive acetabular defects. First, the standard sizes of the implant may not conform to the defect shape. Second, the implant-defect mismatch increases the fatigue failure [18]. The use of patient-specific implants eliminates these concerns to improve fit of the implant in the acetabular defect [19, 20, 21, 22]. The utilization of medical 3D-printing technology has accelerated over the past several years, and the application of 3D-printed implants in orthopedic surgery has become more usual [23, 24]. The main clinical rationale for the use of 3D printed implants is the customization afforded to the surgeons to create a patient-specific implant matching the morphology and topography of the defect. Additional benefits include the capacity to precisely regulate the orientation of the acetabular component and restore the hip center of rotation, as well as the incorporation of several bearing alternatives, including constrained components and dual mobility. However, there remains a lack of evidence on the survivorship of these implants in acetabular revision with severe bone loss. On that account, we have conducted the current study with the main purpose of assessing the survivorship of 3D-printed acetabular implants in Paprosky type III defects with pelvic discontinuity. In addition, we have assessed postoperative complications and the influence of the patient’s age, sex, comorbidities, history of infections, and the presence of other lower limb arthroplasties on implant failure.
Materials and methods
The present research was a single-center observational study. In order to identify all sequential patients who underwent acetabular reconstruction for the treatment of a Paprosky III defect with PD, we retrospectively evaluated our database. From November 2012, 32 patients with failed THA and Paprosky III acetabular bone defects received revision arthroplasty utilizing the 3D printed custom acetabular component (aMace Acetabular Revision System, Mobelife, Materialise, Leuven, Belgium). The three requirements for inclusion were: (1) a failed acetabular implant after one or more prior revisions, or after a primary THA, (2) aseptic loosening as cause of failure and (3) a Paprosky type III defect with PD. In the final analysis, 23 patients were included (Fig. 1).
Patient flowchart for the study cohort.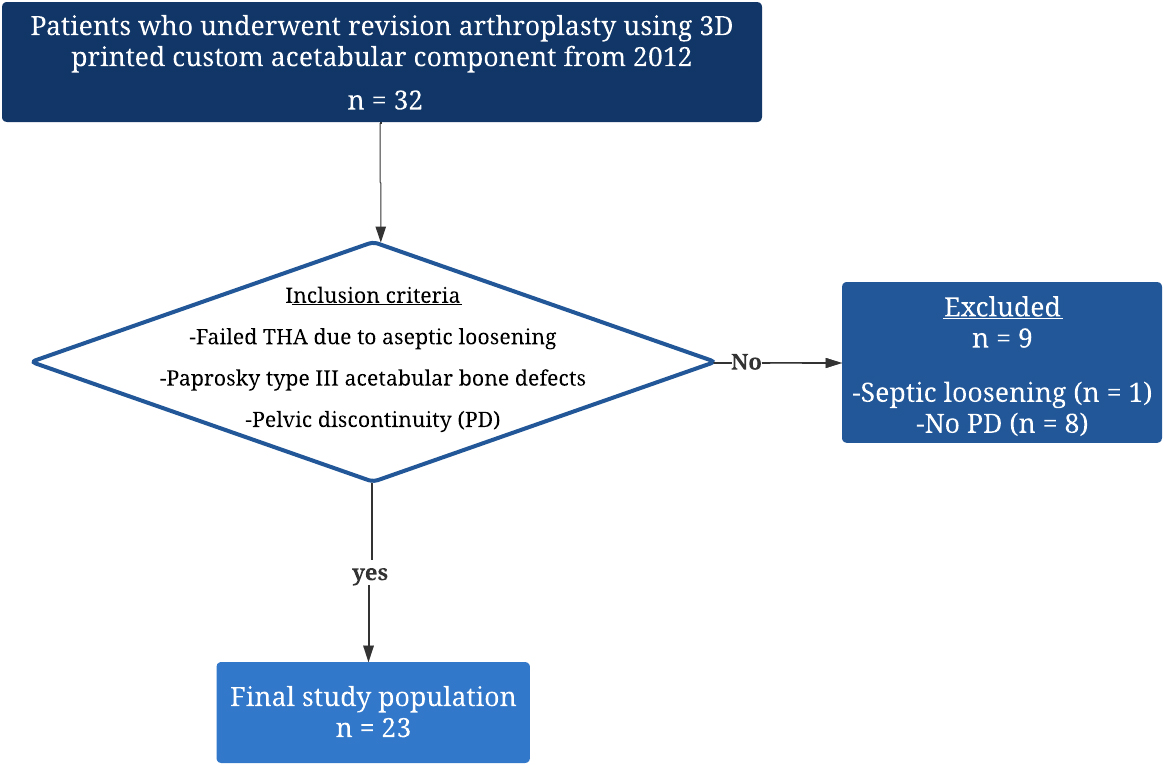
Data on patient demographics, underlying health conditions, primary indications for THA, total of previous revisions and infections, cause of failure, type of last implant, and presence of other arthroplasties were gathered. The Paprosky, D’Antonio (AAOS), and Charnley classification systems were assessed for all patients.
The ultimate bone defect measured by the software with the 3DP custom acetabular component (aMace Acetabular Revision System, Mobelife).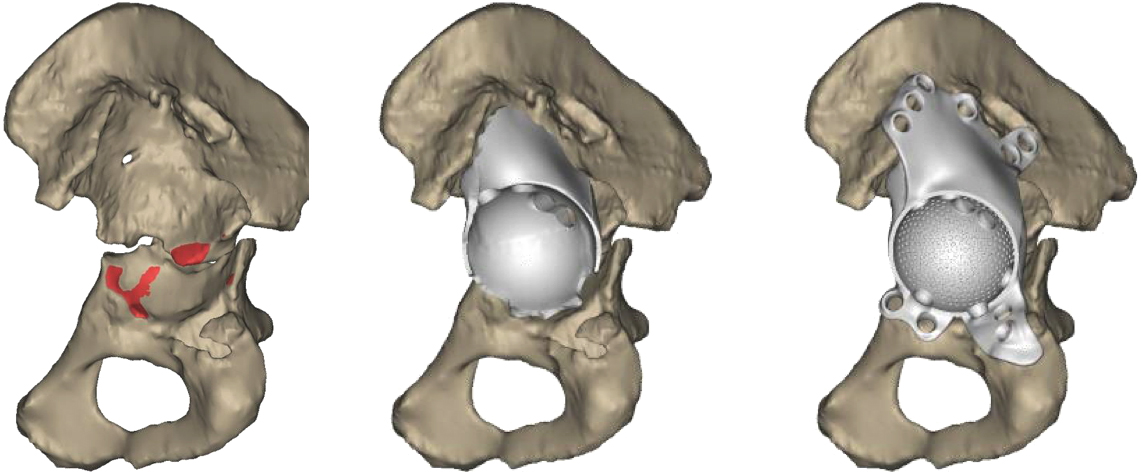
Prior to revision surgery, all patients underwent computed tomography (CT) scans of the pelvis to assess the morphology of the defect. The company that produced the implant analyzed the data to determine the location of the center of rotation of the failed hip joint and examined the remaining bone tissue to create a customized implant design and to develope a precise plan for implantation. The data was presented in a Digital Imaging and Communications in Medicine (DICOM) format, and specialized image processing software (Mimics, Materialise NV) (Fig. 2) was used to estimate the size of the bone defect guided by the method described by Gelaude [25]. Before the final 3D implant was manufactured, the surgeon carefully examined the surgical blueprints and offered suggestions to confirm that the final 3D implant’s design would facilitate proper screw placement and component integration (Fig. 3). The operative surgery was executed via a posterior approach in the lateral decubitus position by nine experienced orthopaedic surgeons, who used 3D-printed plastic anatomical models to guide surgical exposure and bone preparation (Fig. 4). After surgery, patients were allowed to gradually resume bearing weight, starting with 30 kg for the first six weeks, and then gradually increasing to full weight-bearing capacity over the subsequent eight to twelve weeks. Pelvic anteroposterior radiographs were obtained periodically (Fig. 5).
The planned acetabular component with length, placement, and trajectory of the screws.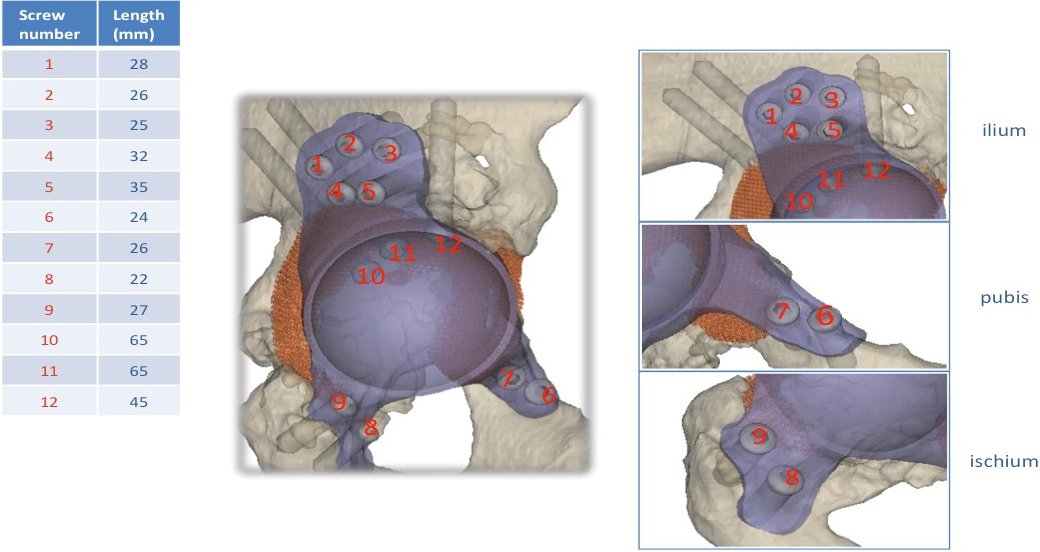
3D-printed plastic anatomical model of the hemipelvis with trial implant.
Preoperative and at final follow-up x-rays of two cases.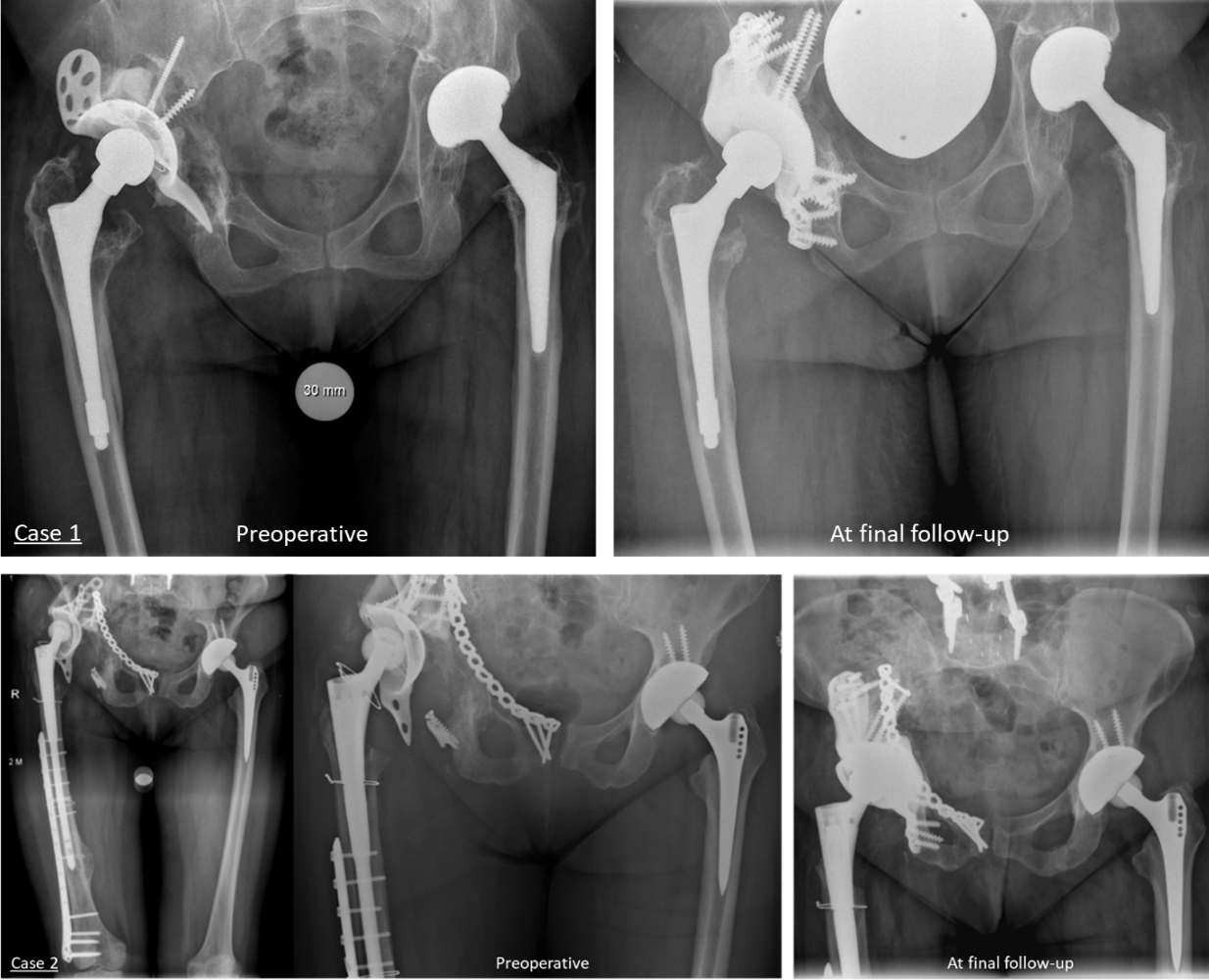
Continuous data were presented as mean
Ethical considerations
All aspects of the study were approved by our Institutional Review Board (PV No: PV5376-3690_1-BO-ff).
Results
Patient characteristics
23 patients were analyzed. There were 22 females and one male. The mean age was 63.9
We observed 3 cases with femoral stem loosening intraoperatively. The breakdown of the classification of each patient’s defect are shown in Table 2. The majority of acetabular defects were found in the posterior superior region, accounting for 82% of cases, as shown in Table 3.
Implant survival outcomes
Patients were followed a mean of 67.22
Postoperative complications
There were nine documented complications in the postoperative setting. Besides the implant failures noted above, four patients sustained a hip dislocation, and two patients had medical complications relating to underlying vascular disease. A bigger head was employed in two cases of hip dislocation and a larger head with neck adapter was used in the other two cases. Regarding the medical complications, one patient had surgical site hematoma and another case had postoperative anemia, but not clinically relevant and the patients were fully recovered without further intervention.
Patient data variables
Patient data variables
THA
Classification outcomes
Total radial Acetabular Bone Loss (TrABL) (Gelaude) (%)
Kaplan-Meier survival analysis.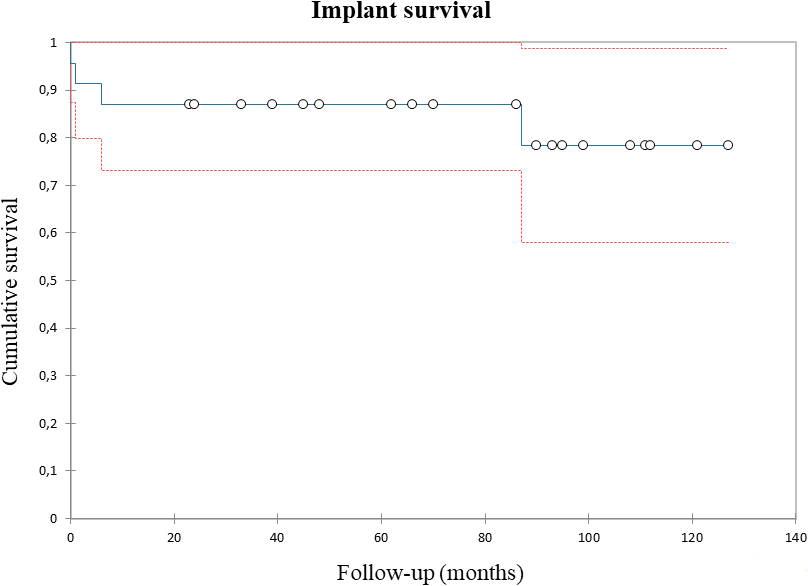
Cox regression analysis
The current research demonstrated ten-year survivorship of 78.3% in patients undergoing revision total hip arthroplasty using patient-specific 3D-printed acetabular components to deal with pelvic discontinuity secondary to severe acetabular defects.
In revision total hip replacement, managing extensive acetabular defects can be challenging, especially when they involve pelvic discontinuity [26]. Several implant options, such as jumbo cups, acetabular cages, adjunctive plating, augments, cup-cage combinations, and allografts, have been proposed for treating these complex defects [11, 12, 13, 20, 27]. While porous metal cup-cage constructs and custom acetabular components have shown promising results [28, 29], long-term follow-up studies are scarce in the literature [29, 30].
Using standard acetabular implants to reconstruct extensive acetabular defects may result in early aseptic loosening and the need for additional surgery. Custom-made acetabular cups have demonstrated a lower risk of early aseptic loosening and re-revision surgery [31]. Long-term studies have demonstrated that 20–35% of patients with custom implants require subsequent revision surgery [28, 30, 32, 33], which are slightly higher than the rate observed in the present study at ten years.
In the context of complex acetabular defect reconstructions, periprosthetic joint infection (PJI) stands out as a particularly worrisome complication. Although studies generally report an incidence of around 8% for PJI [17, 28], this study observed a slightly higher frequency (13%,
This study has several limitations owing to the retrospective nature and small cohort size. These limitations may affect the generalizability of the results. Moreover, the absence of complete follow-up clinical scores presents a limitation that should be addressed in future research to provide a comprehensive view of patient outcomes post-implantation. Furthermore, there is no comparison group in the study and surgeries were performed by multiple surgeons; however, the surgeons involved in the study had extensive level of expertise in arthroplasty, each conducting more than four hundred total hip and knee arthroplasty procedures annually.
Conclusion
Custom-made 3D-printed acetabular components offer several benefits over traditional options, despite its limitations. It is a viable solution for treating acetabular defects with concomitant pelvic discontinuity in revision total hip arthroplasty. The long-term follow-up results show low complication rates and acceptable long-term survivorship, making 3D-printed patient-specific acetabular implants a valuable treatment option for combined PD cases. As technology advances and production costs decrease, the demand for this implant is expected to rise, leading to increased adoption in the future.
Footnotes
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
The authors declare that they have no competing interests.
Funding
The authors report that no financial support was received for conducting this study.