
Abstract
BACKGROUND:
The advances in experimental psychology in the last decade have led to a greater understanding of cognitive bias, and the investigation of cognitive bias modifications as a therapeutic option. Whilst conventionally such interventions are delivered in a laboratory, technological advances are changing the potential modes of delivery of these interventions. Whereas mobile delivery of interventions might seem to increase accessibility and encourage compliance, this might not be the case for cognitive bias modification interventions. To reduce boredom, researchers have investigated whether gamification of the task could help reduce repetitiveness, and the diminished motivation that participants had over time. In a prior review of cognitive bias modification interventions, a collaboration between academics and developers was recommended to ensure that the developed product is evidence-based. With the increased recognition of the importance of participatory action research, participants could better help conventional intervention to meet their needs.
OBJECTIVE:
The aim of this article was to describe the iterative steps in the conceptualization of the co-designed gamified cognitive bias modification intervention for individuals with opioid use disorders.
METHODS AND RESULTS:
A multidisciplinary team worked through the differences in the perspectives offered by healthcare professionals and patient participants, and jointly worked with a developer to conceptualize a new co-designed gamified attention bias modification intervention. The methods shared in this article could be considered and applied to future conceptualization of co-designed interventions.
Keywords
Introduction
The advances in experimental psychology in the last decade have led to a greater understanding of cognitive bias, and the investigation of cognitive bias modifications as a therapeutic option. In a recent meta-analytical review, Boffo et al. [1] considered 14 studies involving 2425 participants, which highlighted that the effect size of bias modification was small (0.23), and that bias modification had an effect of
In a review of mobile-based cognitive bias interventions, Zhang et al. [2] recommended joint collaborations between academics and developers, recognizing that academics can advise on the evidence base of the conceptualized product. However, opportunities for the end-users to contribute to the design are also needed, as they are the eventual users of the product. Zhang et al. [4, 5, 6] recognized the importance of participatory action research and co-design when undertaking a series of workshops to refine a conventional mobile-based cognitive bias modification intervention. They explored participants’ perspectives with regards to the limitations of the existing application and provided recommendations to overcome these limitations and the possibility of adopting gamification strategies [6]. Since the conclusion of the prior co-design workshops [6], the authors have conceptualized the co-designed application, and tested the application by means of a pilot study. The protocol of the pilot study has been recently published by Zhang et al. [7].
In this article, we seek to describe the iterative steps that we used in the conceptualization of the co-designed gamified cognitive bias modification intervention for individuals with opioid use disorders. We attempted to describe in as much detail as possible the setup and design of the system for the new co-designed application, to allow for reproducibility of the results. We decided to specifically target these individuals, given that they routinely present for treatment at the inpatient unit at the National Addictions Management Service (NAMS), and also because opioid abuse and dependency remains to be a significant problem in Singapore [8].
Methods
To conceptualize the application, in each of the workshops described in Zhang et al. (6), participants were separated into two teams. This resulted in the generation of six different prototype sketches. Following the workshops, the sketches of the conceptualizations were reviewed by a multidisciplinary team, which included two addiction psychiatrists (with varying years of experiences), a psychologist who was actively involved in treating individuals with addictive disorders and had experience in cognitive bias modification research, a child and adolescent psychiatrist with experience in developing a gamified intervention for children with attention deficit hyperactivity disorder (with anger issues), a professor in family medicine with vast experience in qualitative research and patient and public involvement in research, and a software developer with vast experience in game development.
Overview of timings of the images by the days of intervention
Overview of timings of the images by the days of intervention
Overview of the instructional video and set of practice trials.
The team identified and systematically worked through (a) resolution of the differences in the conceptualized sketches between healthcare professionals and patient participants, (b) identification of commonalities in the sketches, and (c) identification of a common set of gamification strategies that could be incorporated into the conventional visual probe task. The team considered and prioritized the perspectives of patient participants over healthcare professionals, given that the aim of the co-design workshop was the conceptualization of an application that could meet the needs of patients. The team then worked with the developer to identify the most appropriate method in implementing the new gamified cognitive bias modification intervention.
Figures 1–3 provides an overview of the conceptualized application based on the agreed upon perspectives of the multidisciplinary team. Figure 1 provides an overview of the instructional video as well as the set of five practice trials that individuals could undertake prior to their participation in the actual intervention. Figure 2 summarizes the new visual probe task that individuals would undertake. In the new co-designed variant, a progress bar is included, which is an indicator of the number of trials completed thus far and provides feedback following the completion of each individual trial.
Taking into consideration the feedback of participants in terms of the visual probe paradigm, the team has implemented massive changes. Across the intervention, the percentage of image sets that were presented for a short stimulus interval (i.e. of 200 milliseconds) would gradually increase, whilst the percentage of image sets that are presented for a short stimulus interval (i.e. of 2000 milliseconds) gradually decreases. This corresponds to participants’ perspectives on having stimulus intervals presented for longer duration when they first undertake the task, and with the gradual speeding up of the stimulus intervals. Table 1 provides an overview of the timings of the stimulus intervals by the days of the intervention. Figure 3provides an overview of all gamification features implemented into the newly designed application, which includes feedback (in terms of progress time bar, scores, and immediate feedback after each trial). The gamification strategy of having ‘levels’ in the game has been implemented as shown in Fig. 4, whereby the different days of the intervention could only be unlocked when the task for the prior day was completed.
Overview of the new visual probe task.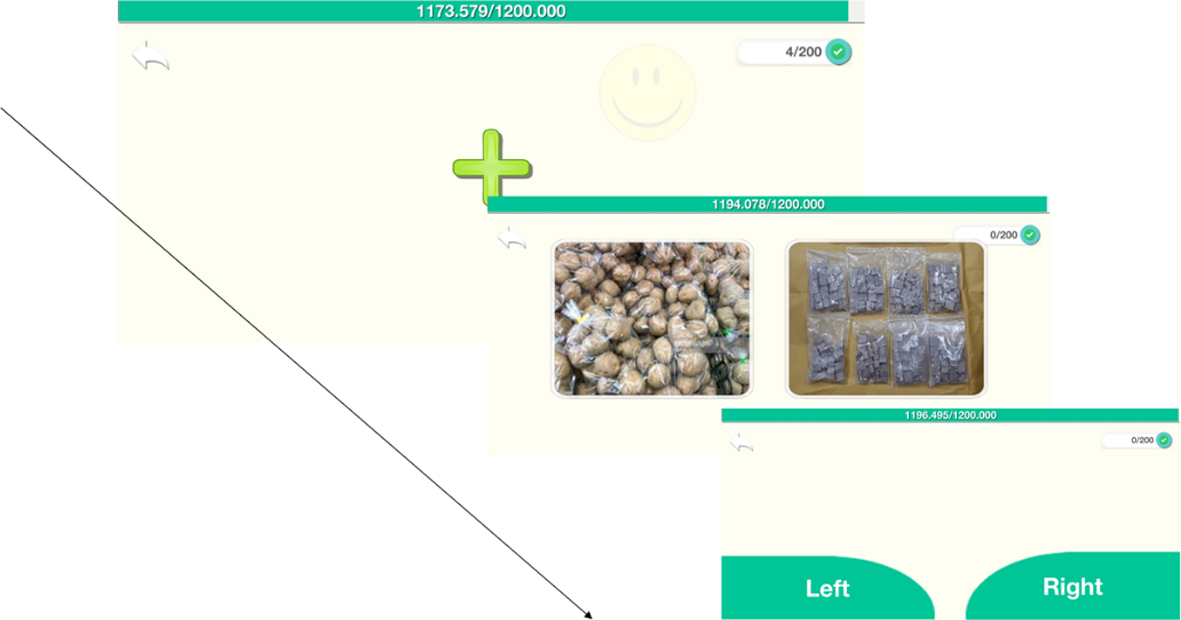
Overview of the gamification elements.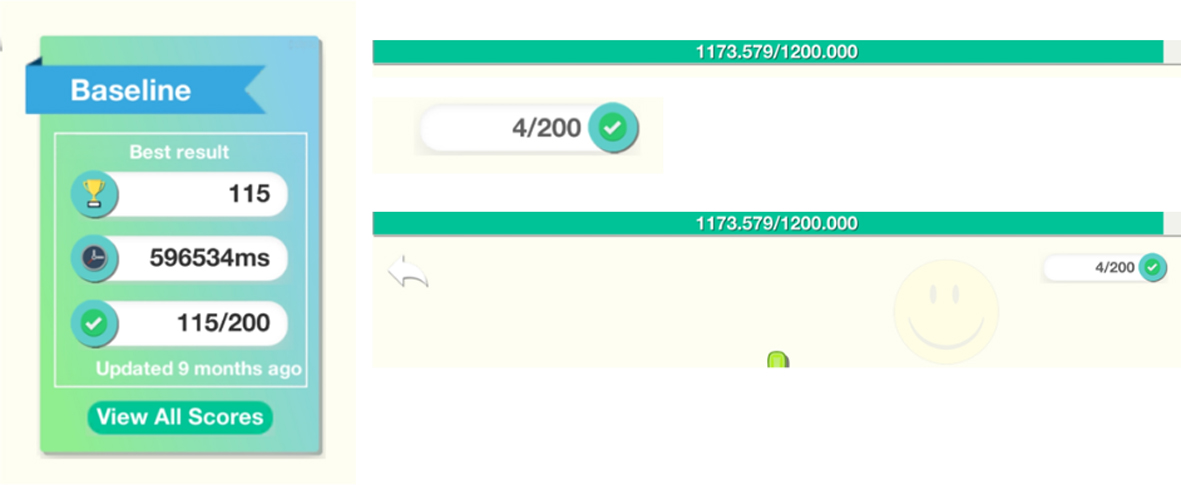
Overview of ‘levels’ in the gamified task.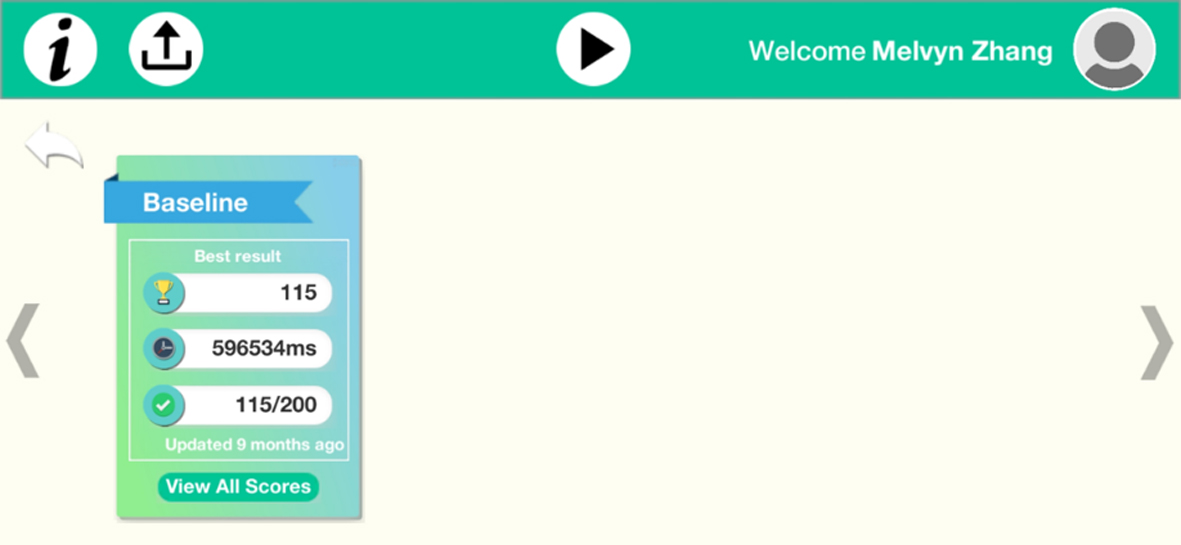
Following the discussion with the software developer, the characteristics that supported the application architecture were:
The mobile application would request resources, such as the set of stimulus images, tutorial videos and task data for the visual probe paradigm from the server. Once the server receives the mobile application’s request, the data is then requested from the storage database. The database storage would verify the request and return the necessary information to the server, which would in turn channel the information to the individual’s mobile application. Figure 5 provides an overview of the overall architecture of the newly developed system. The server that was developed to support the mobile application was built on a Digital Ocean Cloud Service.
An open source operating system (Ubuntu 18.04.1 LTS) was chosen to run the server. PHP, VueJS, JavaScript, HTML and CSS were used in the programming of the server. MySQL was used in the programming of the database for the application. For the mobile application, we decided to make use of Unity3D for the development of the application. This is a cross-platform game engine developed by Unity Technologies that allows the rapid building of a gamified application that could be implemented across platforms.
Overall architecture of the co-designed application (Sobriety360).
To the best of our knowledge, this is the first article that describes how a co-designed attention bias modification intervention has been developed based on the joint inputs of both healthcare professionals and patients. This article demonstrates the first attempt in the application of participatory research methods for attention bias modification research, and also demonstrates that it is feasible and appropriate to seek participants’ ideas and experiences in order to improve the conventional task which has numerous intrinsic limitations. This article demonstrates how a multidisciplinary team worked through the differences in the perspectives and in the identification of common elements, and how they cooperated with a developer in the joint conceptualization of the new application. There were several challenges in the conceptualization of the co-designed application which had to be resolved with the developer. The most important challenge was ensuring that the mobile application could support gaming features and would be able to run across several different smartphone platforms. To resolve this, a gaming platform (Unity 3D) was used, as that platform not only allows the implementation of gaming techniques within the application, but the co-developed application would also be able to run across different platforms and devices. The other challenge was the implementation of the varying stimulus timings for each of the different days of the interventions. To allow this, the server database was set up in such a way that it would allow the independent control of the task parameters for each of the days of the interventions.
Conclusion
This article describes the technical development and conceptualization of a co-designed mobile attention bias modification for individuals with opioid use disorders. The methods shared could be considered and applied to future conceptualization of co-designed interventions.
Footnotes
Acknowledgments
MWZ is supported by a grant under the Singapore Ministry of Health’s National Medical Research Council (grant number NMRC/Fellowship/0048/2017) for PhD training. The funding source was not involved in any part of this project.
Conflict of interest
None of the authors have any competing interests.