
Abstract
BACKGROUND:
Children with cerebral palsy (CP) have disorders of posture and movement and which can limit physical activities such as walking
OBJECTIVE:
This study aims to investigate the effectiveness of virtual reality (VR) combined with robot-assisted gait training (RAGT) on walking ability in children with CP and clarify the most effective degree of weight reduction.
METHODS:
Sixty CP children were recruited and randomly allocated into four different groups. The control group received conventional physical therapy (
RESULTS:
All indicators had improved significantly in each group after the intervention (
CONCLUSIONS:
VR combined RAGT can effectively improve walking ability in children with CP, especially when the weight loss is 30%.
Introduction
Cerebral palsy (CP) is the most prevalent neurodevelopmental disorder caused by non-progressive brain injury in fetuses and infants [1]. Children with CP have disorders of posture and movement and which can limit physical activities such as walking [2]. Since the limitation of lower limb function directly affects the activities of daily living (ADL), how to improve the gait ability in children with CP is of great significance.
Currently, the conventional methods for CP include physical therapy, occupational therapy [3], as well as traditional Chinese therapy like acupuncture and massage [4, 5]. These interventions are often concurrently used and consume numerous amounts of energy, cost, and time [6]. More importantly, few studies have proven that these conventional therapies are effective in gait recovery in CP children [7].
Besides the conventional therapies, technology-based treatments have been recently proposed for improving walking ability [8, 9]. Among others, robot-assisted gait training (RAGT) has been widely used in gait rehabilitation of adults with different diseases such as stroke, spinal cord injury, as well as children with CP [10]. RAGT is composed of a body weight support (BWS) system and two actuated orthoses that drive the patients’ legs on a treadmill. Based on the principles of motor learning and neuroplasticity, the effectiveness of RAGT relies on repeated input of the correct gait pattern and goal-oriented tasks. Jin et al. showed that RAGT was effective in improving gross motor function in CP children [11]. Similarly, Cherni et al. also confirmed the role of RAGT in enhancing the walking speed and endurance in children with CP [12]. The rationale of VR is also grounded on some theories of neuroplasticity, including goal-oriented, repetitive, and intensive training [13, 14, 15]. It can provide real-time feedback by allowing users to interact with virtual objects, which makes VR a funnier and playful approach especially for children [16] Moreover, children have higher neuroplasticity and better motor learning ability than adults, so it is more effective to improve motor function in children’s training [17].
Nevertheless, VR combined with RAGT is often applied in the treatment of stroke patients rather than in pediatric CP [18, 19]. Although it has been shown that the level of BWS can alter gait parameters such as stride length, stride speed, and standing time, thus affecting the recovery of gait in patients [20, 21], there have been no reports to determine the optimal level of BWS for children with CP. Therefore, the present work aimed to investigate the effect of VR combined GRAT with different (15%/30%/45%/) levels of BWS in improving the walking ability of CP children and to determine the most valid level of BWS.
Methods
Participants
We recruited 60 children (28 males and 32 females, 6 to 11 years old) from the Rehabilitation Department of Shanxi Provincial Rehabilitation Research Center who met the diagnosis of spastic CP. Participants were selected in line with the inclusion and exclusion criteria.
The inclusion criteria were: (1) height suitable for walking robots; (2) rate in Level II-III on the Gross Motor Function Classification System (GMFCS); (3) able to follow instructions and cooperate with trainers.
The exclusion criteria were: (1) epilepsy, severe heart, lung, liver, and kidney disease; (2) other neuromuscular and osteoarticular diseases; (3) Botox injection or orthopedic surgery and muscle release within 6 months; (4) vision or hearing impairment.
This study was approved by the Ethics Committee of our hospital. All parents/caregivers of each child have been informed of the purpose and procedures of the study and signed informed consent. Rehabilitation programs were subsidized by the government, and all children received half-year treatment in outpatient visits.
Interventions
This research was a randomized controlled trial. Random allocation software was used to divided children into 4 groups. All participants completed 48 treatment sessions for 3 months, each session was conducted for 50 min (30 min basic physical therapy followed by 20 min different kinds of walking training), 4 times per week. The control group underwent conventional walking training, whereas the task groups underwent the VR combined RAGT at different levels of weight support:15% for group A, 30% for group B, 45% for group C. The flow diagram for experimental procedures is shown in Fig. 1.
Flow diagram for experimental procedures.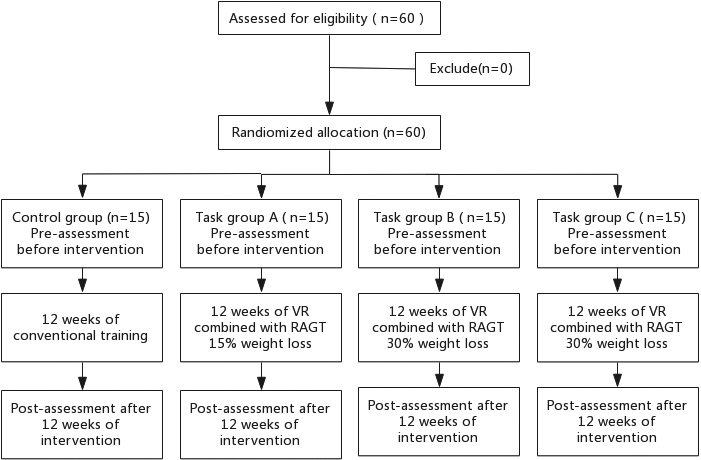
The detailed procedures of basic training are as follows:
Warm-up (5 min): Stretching all the lower limb joints and major muscles to relieve muscles tension and improve the joints’ range of motion. Strength Training (5 min): Standing on one foot, double bridge training to build the muscle strength of lower limbs. Balance Training (10 min): Weight shift training, kneel training, throw and catch ball training in standing, balance board standing training to improve the load-bearing ability of affected lower limbs and to increase dynamic balance. Coordination Training (5 min): Alternating the lower limb flexion and extension training, alternating step-up training to improve the coordination of the lower limb.
For 20 min different kinds of walking training: the control group was assisted with walking training in parallel bars or on a flat surface, according to the condition of the child. The task groups wore VR throughout the training process. GRAT BWS was set for each group (Group A 15%, Group B 30%, Group C 45%). Walking speed was adjusted to the patient’s ability to participate actively during therapy. The guidance force was maintained at 100% during training. A physical therapist monitored the lower limbs, prompted the experimental procedure, and provided verbal encouragement when necessary [22, 23].
The Lokomat (Hocoma AG, Volketswil, Switzerland) was used for RAGT in task groups. This device comprises two robotic-orthosis, each equipped with motor drives in hip and knee joints which guide the patients’ legs moved along the physiological walking pattern on a treadmill. Children’s limbs were fixed into the orthosis with suspenders tied to a BWS system to bear subjects’ body weight. The orthosis is adjusted to the width of the child’s hips and the length of the lower limbs to ensure that walking with the device is as natural and comfortable as possible. The hip and knee joints of the Lokomat orthosis are computer-controlled, moving in the sagittal plane through the gait cycle and ensuring that the walking speed is synchronized with that of a treadmill [24]. The Lokomat’s orthosis with kids legs was chosen for children whose femur lengths were between 210 and 350 mm. In both groups, patients were encouraged to behave actively during RAGT.
VR was applied in task groups while they are training on Lokomat, the scenario of VR took place in the field, where subjects had to walk along a straight path in the middle of the screen. The Lokomat can both input and output the children’s movements. It sensed the steps of the children and transferred the signal into the movement of the virtual character’s legs in real-time. Consequentially, the character in VR walked along the path according to the children’s own steps. The training was supervised by a trained therapist.
Outcomes measures
There were four pre- and post-testing outcome measures: the EMG, the Modified Ashworth Scale, GMFM88 dimension E, and D as well as the 6-MWT.
Surface electromyography (EMG) was used to evaluate the strength and tension of the gastrocnemius muscle. Its evaluation index consists of EMG median frequency(MF), integrated EMG (iEMG) and co-contraction ratio (CR) [25]. CR
The Modified Ashworth Scale scores the level of muscular tension between 0 (lack of spasticity) and ? (severe rigidity) is used to provide the evaluation of the ankle spasm. Evidence indicates that the Modified Ashworth Scale is a valid and reliable measurement tool [27].
The Gross Motor Function Measure 88 (GMFM88) dimension D (standing) and E (walking) were applied by a GMFM-certified therapist to evaluate subjects’ gross motor ability. Dimension D includes 13 items with a total score of 39 points, while E includes 24 items with a total score of 72 points. The GMFM88 was developed and validated by Engelen in 2007 [28].
Children’s gait ability and endurance were assessed by the Six-Minute Walking Test (6-MWT) [29]. During the test, children with CP were allowed to are required to walk as fast as possible.
All participants were allowed to wear their orthoses or footwear during the assessments of GMFM88 and 6-MWT,
Statistical analysis
Data were evaluated for normality and symmetry to ensure that the use of parametric statistics as appropriate. A paired t-test was applied to compare the changes in the data pre- and post-test. An analysis of variance (ANOVA) was used for comparisons of the values at different levels of body weight reduction between 4 groups All statistical analyses were performed using SPSS Statistical Package, version 26.0.
Characteristics of all participants
Characteristics of all participants
Values are expressed as mean
In total, all 60 participants completed the 12-week training without a drop-off. As shown in Table 2, compared to the baseline, the post-test level of iEMG, MF, CR, the Modified Ashworth, GMFM dimension D, and E, as well as 6-MWT were improved significantly in all groups (
Discussion
The current study investigated the effects of VR combined with GRAT at different levels of BWS on gait ability in CP children. According to the results of the EMG, the Modified Ashworth Scale, the GMFM dimension E, and D, and 6-MWT, comparing to the control group, the greater changes were the observed in task groups, among which 30% weight reduction registered the most remarkable improvements in walking ability.
To the best of our knowledge, this is the first study to determine the most valid level of BWS when applying RAGT to improve gait ability in children with CP.
A study suggested that varying degrees of BWS may influence the size of steps and the shift of weight during walking, which in turn affects the recovery of patients’ walking ability [20, 21]. For adult patients with stroke on treadmills, the most applied level of BWS is 30% [30, 31], and the effectiveness has been proved on gait training [32, 33]. Yet the optimal level of weight support provided by walking-assisted robots for children with CP has not been clearly investigated. Current studies also vary greatly in the level of BWS taken for CP children. In the study by Jin, et al., RAGT BWS was adapted to the condition of the knee of the children with CP, and the results showed that RAGT improved the motor ability of the children [11]. Pool et al. found that, compared to conventional ground training, RAGT had no significant effect on indoor walking speed and gross motor ability in children with cerebral palsy when 60% of BWS was taken [34].
Our results indicated that the walking robot works best when the level of BWS was set at 30%. Possible reasons are as follows: On the one hand, excessive weight loss reduces the load-bearing of the lower limbs of children with CP, which is detrimental to both the improvement of lower limb muscle strength and the proactive engagement of active movement in children with CP. In response, the walking robot has to increases the driving force to ensure a certain walking speed, which will further affect the muscular endurance of the lower limb. On the other hand, insufficient weight loss will pose a strong stimulation on
Results for outcome measures
Results for outcome measures
Values are expressed as mean
gastrocnemius muscle strength, which will worsen the gastrocnemius muscle tension growth and in turn, restrict the growth of strength.
A previous study has reported that lower limb muscular effort measured by surface electromyography in children with CP was significantly improved after RAGT combined with VR [16]. The repetitive and symmetrical movements provided by the walking robot relieve muscular tension in children with CP and helps them to better control the lower limb joints, improving the stability and coordination of joint movements [20]. In the study by Kenichi Yoshikawa et al. walking assist device can increase the ankle range of motion and musculus gastrocnemius activity function [35]. Also, Cherng et al. reported that the gait and gross motor function was significantly improved after gait training with a BWS in CP children [36]. Specifically, during RAGT, the ambulation ability in stroke patients could be improved more significantly when VR is applied. This may attribute to the fact that patients in the VR augmented RAGT group have higher acceptability and motivation to undergo therapy [19]. Besides that, VR increases the fun of training, thus activates brain regions related to motor learning, and promote functional reconstruction [37]. Consistent with the above studies, our work shows that VR combined with RAGT was effective in relieving ankle spasm, balance, gross motor ability, as well as gait function in CP children, and this may be attributed to the fact that combination therapy is more effective than RAAT alone.
Some limitations in the current study should be considered in the future study, first, the insufficient samples in this study may reduce the generalization of the outcome. Second objective tests are required to confirm the underlying mechanism of these improvements. Thus, a larger sample size as well as laboratory examination, brain functional imaging, and biomechanical analysis is required in future studies.
Our results suggested that when weight loss is at 30%, the VR combined with RAGT can be most effective in reducing gastrocnemius and ankle spasm, improving gastrocnemius strength, and can further improve balance and gait in children with CP.
Footnotes
Acknowledgments
This study was supported by Shanxi University and Shanxi Rehabilitation Research Center.
Conflict of interest
The authors have no conflict of interest to report.