
Abstract
BACKGROUND:
Grip force estimation is highly required in realizing flexible and accurate prosthetic control.
OBJECTIVE:
This study presents a method to accurately estimate continuous grip force from surface electromyography (sEMG) under three forearm postures for unilateral amputees.
METHODS:
Ten able-bodied subjects and a transradial amputee were recruited. sEMG signals were recorded from six forearm muscles on the dominant side of each able-bodied subject and the stump of amputee. Meanwhile, grip force was synchronously measured from the ipsilateral hands of able-bodied subjects and contralateral hand of amputee. Three force profiles (triangle, trapezoid, and fast triangle) were tested under three forearm postures (supination, neutral and pronation). Two algorithms (Generalized Regression Neural Network (GRNN) and Multilinear Regression Model (MLR)) were compared using several EMG features. The estimation performance was evaluated by coefficient of determination (
RESULTS:
The optimal regressor combining TD and GRNN achieved
CONCLUSIONS:
The proposed method has the potential for precise force control of prosthetic hands.
Introduction
Myoelectric prosthetic hands generally use sEMG signals from amputees’ stumps as control signals. By processing and decoding sEMG signals, prosthetic hands can realize pre-defined gestures or simple force control. Since the first myoelectric prosthetic hand in 1948 [1], for decades the goal of control strategies has always been to restore the lost hand motor function of limb amputees. Human hands can control different gestures with different force levels easily in daily life, and therefore an ideal myoelectric prosthetic hand should also be natural and intuitive in both gesture and force control. Since the first application of pattern recognition algorithms for simple prosthetic grippers, significant efforts were made for decoding the user’s gesture intention, and different online and offline classification methods for hand gestures have been reported [2, 3]. However, control strategies related to decoding grip strength are less investigated and reported, although grip is one of the main functions of hand which is highly used in daily life. As a result, the grip force control of current prosthetic hands is neither intuitive nor natural.
It is known that the force exerted by human hand can be indirectly estimated with sEMG from forearm muscles. In the 1960s, Bottomly [4] proposed a proportional control strategy, which set the grasp force proportional to the envelope of recorded sEMG signals. This simple control strategy has been widely applied in clinical scenarios and even some advanced prosthetic products like Ottobock’s Sensor Hand and DMC plus [5]. However, the relationship between EMG amplitude and grasp force is actually not necessarily linear. It is affected by many factors such as technical conditions and muscle types [6, 7]. Moreover, due to the complexity of EMG signals, it is difficult to obtain the same signal for the same force level, even from the same person [8]. Therefore, the current force estimation method can only achieve a rough approximation.
Until now, researchers have estimated discrete levels [9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21] or continuous profiles [22, 23, 24, 25, 26, 27, 28] of grasp force from EMG signals using either classifiers [9, 10, 11, 12, 13] or regressors [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28]. In general, EMG signals and corresponding grip force signals should be synchronously acquired, and then both signals are processed to train a learning model which can predict the corresponding force from the newly acquired EMG signals in subsequent prosthetic control. To estimate discrete force levels, the subjects are usually asked to exert forces with different levels and then artificial neural networks, or regression models are trained to estimate the force levels. However, the natural force exertion of an intact hand is continuous, and thus the aforementioned approach can only enable a discrete approximation and cannot accurately predict the fine changes of grasp force in practical applications, where an adjustment of force is required while grasping. Compared with discrete force estimation, the continuous force estimation can fully reflect the user’s grasp intention, and it does not require subjects to maintain different muscle contraction levels, and so it is relatively easier to implement. For this purpose, researchers have estimated continuous grasp force from either intramuscular electromyography (iEMG) [22, 23] or sEMG [24, 25, 26, 27, 28] recordings. Different regression algorithms, such as MLR [22, 23, 24], Artificial Neural Network (ANN) [22, 23], Extreme Learning Machine (ELM) [25], GRNN [26], Support Vector Regression (SVR) [27] and logarithmic model [28], have been used to map EMG features to grasp force, and many features, such as root mean square (RMS), mean absolute value (MAV), waveform length (WL), zero crossing (ZC), variance (VAR) and Willison amplitude (WAMP), have been investigated [23, 26]. However, most of the approaches are limited to a single calibration posture, which cannot realize prosthetic grasp with various forearm and wrist postures like intact human hands.
In another aspect, it is found that mirrored bilateral training can be used to associate EMG of one limb with the force of contralateral one [27]. Recently, the continuous mirrored force has been successfully estimated for intact subjects and a subject with congenital malformations [29]. However, there is little literature about continuous grasp force estimation of transradial amputees, despite the confirmed fact that subjects with amputations decades ago can still produce distinct and stable signals for various force levels [27]. Kamavuako et al. [22] successfully estimated mirrored force from iEMG for intact subjects, and the estimation accuracy
In order to realize a possible precise estimation of continuous grip force for prosthetic applications, in this work, we proposed an approach that used GRNN to associate sEMG signals recorded from six forearm muscles with grip force under three forearm postures. The regression model was optimized in intact subjects using ipsilateral training, then validated by a unilateral amputee using mirrored bilateral training. The results were discussed in detail and further work related to clinical application was proposed.
Data and method
Experimental protocol
Ten intact subjects (six males; age range: 22–35 years, all right-handed, referenced S1-S10) without any musculoskeletal disorders, participated in the experiments. Additionally, one left transradial amputee (male, age 43, years by amputation: 2 years, remaining forearm: 60%, right-handed) also participated. No history of phantom limb pain was reported from this amputee. Besides, he had more than half a year’s experience of using simple myoelectric grippers since amputation. Referring to Atzori et al. [2], the remaining forearm percentage was computed as the ratio between the amputated forearm length and the contralateral forearm length (from the elbow to the wrist). The characteristics of the intact subjects and the amputee are listed in Tables 1 and 2, respectively. This study was approved by the Institutional Review Board of Shenzhen Institute of Advanced Technology, Chinese Academy of Sciences (IRB number SIAT-IRB-210415-H0560). Written informed consent was provided before the experimental procedures, and permission to publish photographs for scientific and educational purposes was obtained from all subjects.
The characteristics of intact subjects
The characteristics of intact subjects
The characteristics of the amputee
The primary device for signal acquisition is a Portable System DataLOG PS850 (Biometrics Ltd.), which consists of a portable data acquisition unit, eight active EMG sensors and analysis software. The DataLOG has a 14-bit front end ADC giving a full-scale input of
The sEMG signals were recorded from six forearm muscles: flexor digitorum superficialis (FDS), flexor carpi ulnar (FCU), extensor digitorum (ED), extensor carpi ulnar (ECU), extensor carpi radialis brevis (ECRB), and extensor carpi radialis longus (ECRL). We selected these muscles because flexor muscles and extensor muscles were both highly associated with grip force according to Hoozemans and van Dieen [24] and since they are still available for most transradial amputees. The location of the muscles was found by palpation. The electrodes were placed in the center of the muscle belly away from tendons and the edge of the muscle, parallel to the muscle fibers. First, the participants’ skin was carefully cleaned with alcohol cotton pads, and then the EMG sensors were attached to the skin with adhesive tapes. Afterwards, the EMG sensors were fixed with self-adhesive bandages to prevent displacement or even detachment during the experiment. In addition, a reference electrode was placed on the olecranon of the elbow.
The experiment setup for (a) intact subjects and (b) transradial amputee.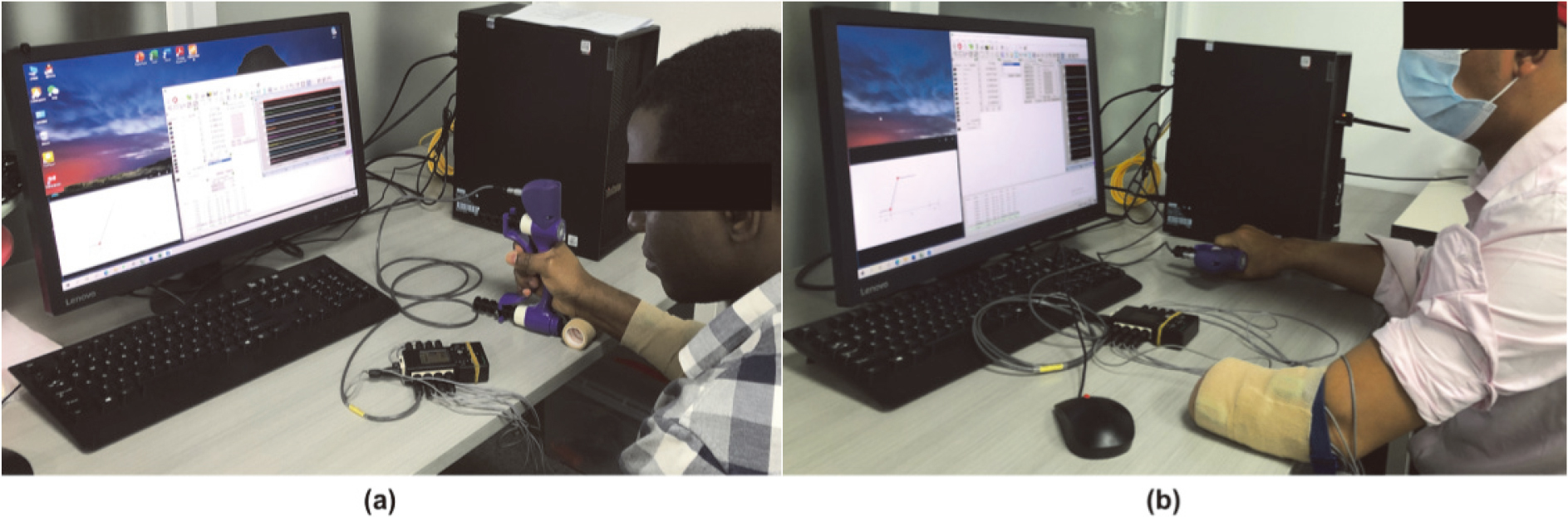
During the experiments, the participants were seated at a desk with their arms comfortably placed on the desktop (see Fig. 1). Referring to Gijsberts et al. [32], the participant’s forearm was not constrained to increase comfort and encourage natural movements. The participants were asked to exert continuous grip force under three forearm postures: supination, neutral and pronation, as shown in Fig. 2. In the supination posture, the palm was facing up; in the neutral posture, the palm was facing inward, orthogonal to the plane of the table; in the pronation posture, the palm was facing down. When the subjects changed postures, they were asked to just turn their forearm and keep their elbow and shoulder relaxed and still. The intact subjects were asked to exert grip forces with their right hand, and the sEMG singles were recorded from the ipsilateral forearm. While the amputee performed mirrored bilateral contractions, including mirrored forearm posture and grip strength. Myoelectric signals were recorded from the left stump, and grip force was measured from the contralateral hand.
Grip force at maximum voluntary contraction (
The participants were then instructed to perform three trials of isometric contraction under each posture following three types of force profile (triangle, trapezoid, and fast triangle), resulting in a total of nine trials, with a length of about 9 min. The intact subjects were asked to exert force to their medium force level (about 60% MVC). While for the amputee, considering it is more difficult for the residual limb to exert force, he was asked to exert force to a comfort level, about 35% MVC. During the trials of the triangle and trapezoid profiles, subjects were asked to produce a continuous and dynamic force profile in 7 s. During the trials of fast triangle profile, subjects were asked to produce a continuous and dynamic force profile in 2 s, nearly as fast as possible. Detailed explanations of the three types of force profiles and relevant references are provided in Table 3. Each profile was repeated six times, separated by 4 s of rest. Trials were conducted at an interval of 2 min. The order of the postures and profiles were randomized across the participants. The three force profiles were designed to simulate the common slow and fast forces that human hands experienced in daily life.
Description of contractions performed by subjects
Three forearm postures: (a) supination, (b) neutral, and (c) pronation.
The computer in front of the participants provided visual stimuli of profile videos and feedback of measured grip force value while simultaneously acquiring data from the electrodes and hand dynamometer. The participants were instructed to exert grip force following the force profiles while at the same time noticing the measured force value.
The myoelectric signals were offline bandpass filtered (sixth-order zero-lag Butterworth filter, cut off frequency 20–450 Hz) to reduce direct current (DC) noise, high-frequency noise, and motion artifacts, then notch filtered at 50 Hz (second-order zero-lag IIR filter) to attenuate the power line interference. In addition, the grip force signals were super-sampled to 1 kHz and filtered using the same type of notch filter.
The sEMG signals were then segmented into signal windows of 100 ms, with no overlap. The window size was optimized based on preliminary experiments. In total six features were subsequently extracted from these windows including five separate features and one feature set combined by four time-domain features. They were:
(1) MAV: It is one of the most popular EMG features. MAV is the average of the absolute value of the EMG signal. Because it has much information on muscular contraction strength, it is advantageous to estimate grip force. The definition of its equation can be expressed as
Where
(2) RMS: Maybe, RMS is the most used feature in myoelectric control applications. It has been proved that there is a quasi-linear relationship between the RMS value and the force exerted by a muscle (under ideal conditions). It can be defined as
(3) WL: It is defined as the cumulative length of the EMG waveform over the signal windows. WL is a power index; it can measure the complexity of the EMG signal. It can be formulated as
(4) VAR: It is calculated by taking the average of square values of the deviation of the EMG signal. Because the mean value of the EMG signal is close to zero, VAR can be computed as
(5) Marginal discrete wavelet transform (mDWT): Discrete Wavelet Transform (DWT) can be used to decompose the EMG signal in terms of a wavelet function at different levels of resolution. mDWT is obtained by preserving only the marginals at each level of the decomposition. Thus, it is referred to as marginal Discrete Wavelet Transform (mDWT). As a more advanced feature representation, mDWT is a time-frequency feature that has been proven effective in posture classification and finger force regression. The calculation of mDWT is based on Gijsberts et al. [32].
(6) Time-domain feature set (TD): Proposed by Hudgins et al. in 1993, TD has become one of the most used features in the sEMG literature. It includes four time-domain features, i.e., MAV, WL, ZC, and slope sign change (SSC). ZC can defined as
Where
SSC is defined as
Where
The calculation formulas of MAV, RMS, WL, VAR, ZC and SSC are based on Phinyomark, Phukpattaranont and Limsakul [33]. We selected these features because they have been commonly used in the literature related to EMG-force [23, 26, 32, 34]. We also calculated the mean value of grip force (MV
The data (including the rest periods) for each subject was split into training sets and test sets based on repetitions. For each profile trial, repetitions 2, 4 and 6 were used as the training set, and repetitions 3 and 5 were used as the test set. The first repetition was discarded, as subjects usually need an adaption of the force exertion [35]. Previous literature has shown higher estimation performance when combining multiple training trials into one longer training set [36]. Therefore, to improve the model’s prediction accuracy and ability under different forearm postures, we sequentially connected the training sets from three profiles and three postures to train the regression models.
Regression models were used to learn the association between EMG features and the grip force. We built regression models for each feature type and each subject. As known to all, regression algorithms have an important influence on estimation accuracy. As previous literature shows a linear or nonlinear relationship between the amplitude of EMG signal and force exerted by human muscles [6, 7, 37]; therefore, we compared a linear algorithm and a nonlinear neural network. They were:
(1) MLR: It is a traditional method in force estimation from EMG signals. Since Bottomley [4] applied a linear model to the EMG-force relationship for hand prostheses in the 1960s, this control strategy has been widely used in clinical applications. MLR finds the best combination of parameters by minimizing the loss function (i.e., the residual sum of squares).
(2) GRNN: It was proposed by Specht in 1991 [38]. It is a one-pass learning algorithm with a highly parallel structure; thus, it features fast learning and high robustness. Therefore, GRNN has been widely applied in many nonlinear regression problems. Furthermore, GRNN has also been successfully employed in grip force estimation from EMG [26]. GRNN estimates values for continuous dependent variables using nonparametric estimators of probability density functions. In addition, by adjusting the value of smoothing factor
Training and testing strategy
By convention, both inputs and targets in the training and test data sets were scaled between
Like most research related to myoelectric control, we first optimized the EMG-force model in intact subjects. Then, we implemented the optimal model for the amputee.
Evaluation metrics
The performance of the regression models was evaluated using
Where
MAE is calculated as a percentage of
Paired
Results
We compared the grip force estimation results of the two regression algorithms using each feature in intact subjects to select the optimal algorithm and feature. Then, regression models built by different muscle combinations were assessed. Finally, we show the results of the amputee using the optimal model.
Results for intact subjects
The estimation performance of all combinations of six features and two algorithms measured in terms of
(a) 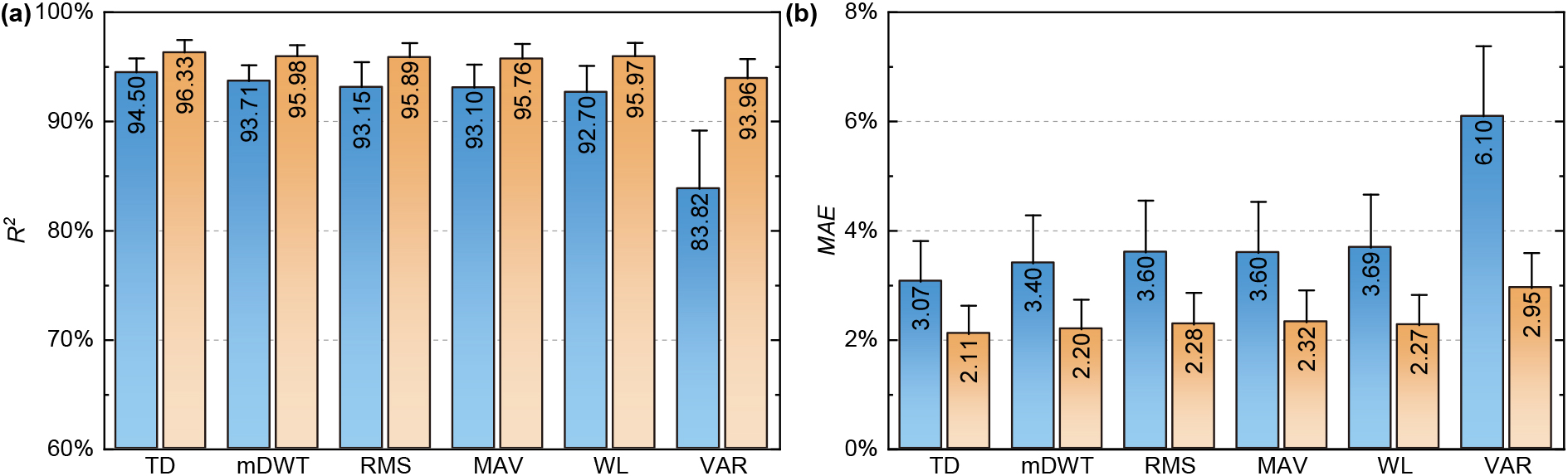
Estimation results under three forearm postures of the first intact subject. For each posture, from left to right are two triangles, two trapezoids, and two fast triangles, respectively. The black solid lines denote the measured forces, and the red dashed lines denote the estimated forces.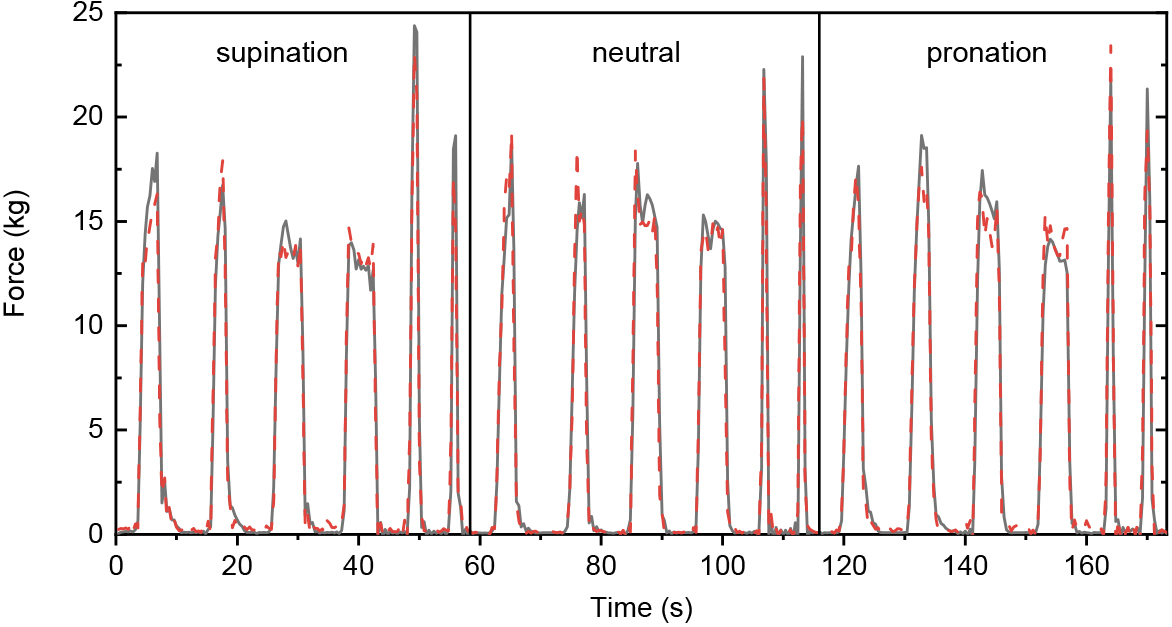
The extracted true and estimated forces under three forearm postures of a typical subject (S1) using the final regression model are illustrated in Fig. 4. For each posture, from left to right are test sets of triangle profiles, trapezoid profiles, and fast triangle profiles, respectively. Subsampling is applied to all profiles to improve visualization. The dynamic force prediction results using the TD/GRNN regressor were excellent, as proved by the fact that time histories of the predicted force agreed well with those of the measured force.
To investigate whether grip force profiles can be estimated with sEMG signals recorded from fewer muscles, we compared the estimation performance of sEMG signals recorded from different combinations of forearm muscles. There was a total of 63 combinations for 6 investigated muscles.
(a) 
Estimation results under three forearm postures of the amputee. For each posture, from left to right are two triangles, two trapezoids, and two fast triangles, respectively. The black solid lines denote the measured forces, and the red dashed lines denote the estimated forces.
(a) 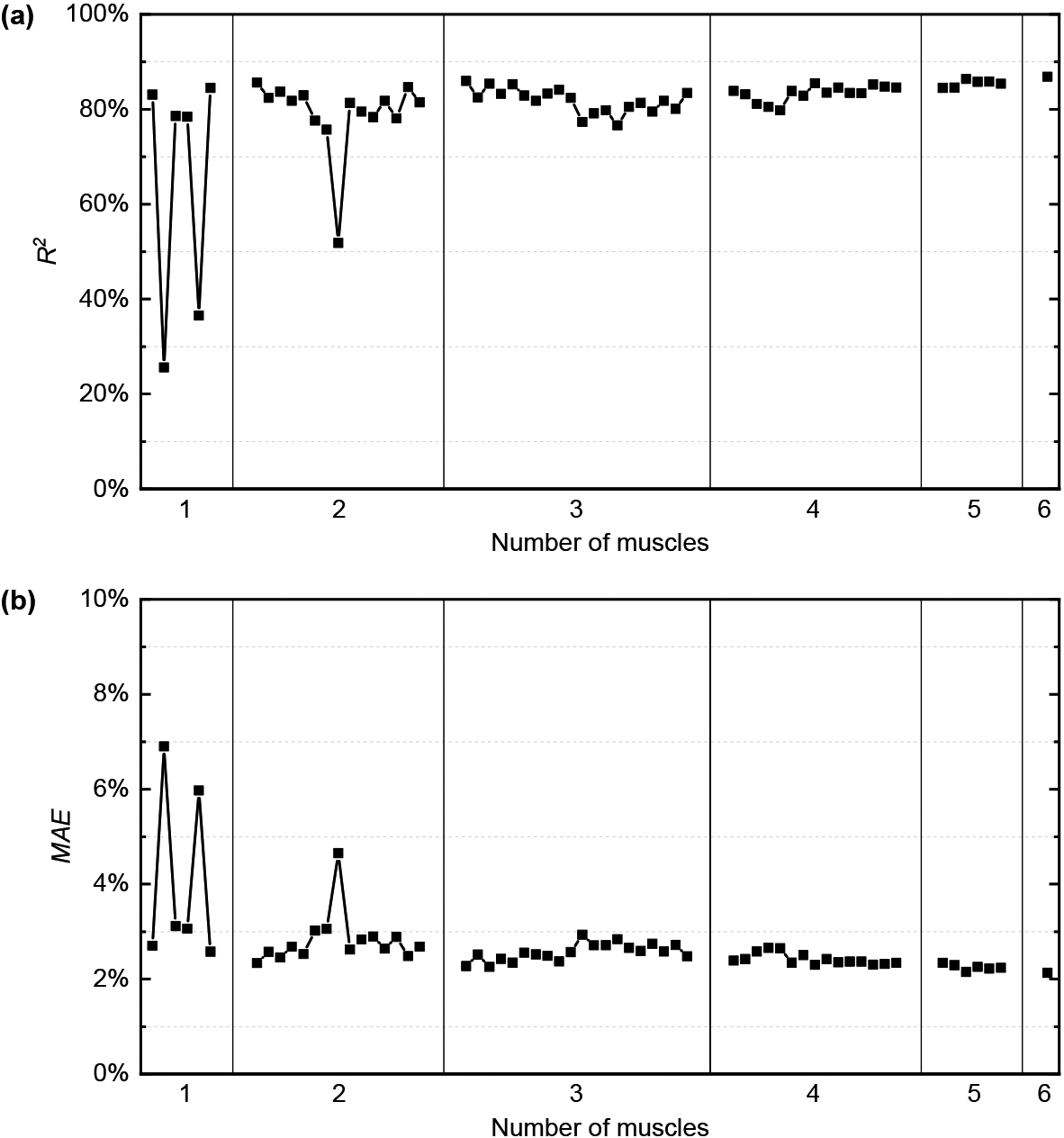
Figure 5 shows the estimation performance of all muscle combinations, averaged across 10 intact subjects. In general, the estimation performance was improved when the number of muscles increased. The best model included EMG signals from all muscles. Among all muscle combinations, ED, ECRB and their combination obviously resulted in the worst performance. One-way ANOVA results revealed that estimation performance of five combinations (ED, ECRL, ECRB, ED&ECRB and ECRL&ECRB) were significantly different from that of using six muscles (in both two metrics,
The optimal regressor was applied to data of the amputee. The estimation performance was
The encouraging results perfectly proved that the surface EMG recorded from the remaining forearm could be used to estimate the continuous force profiles produced by the contralateral limb in the case of bilateral, symmetric contractions of unilateral amputees. According to Kamavuako et al. [22], as amputees lack sensory feedback, it is more difficult for them to match force between the intact and phantom hand during bilateral grasping. Here, this amputated subject obviously tended to overestimate the force produce by his phantom limb, especially in the fast triangle trials, as evident in Fig. 6. As previously mentioned by Gijsberts et al. [32], the residuals might depend on the force magnitude; therefore, the MAE value was relatively small compared with the intact subjects, because the amputee was asked to exerted grip force much smaller than the intact subjects to reduce difficulty.
Figure 7 displays the estimation performance of all combinations of EMG signals recorded from the 6 forearm muscles for the amputee. The results of the amputee revealed a high degree of consistency with the intact subjects in terms of curve tendency. Increasing the number of muscles increased the estimation accuracy. In addition, the three combinations: ED, ECRB, and ED&ECRB, also resulted in the lowest performance.
Discussion
There has been a continuous debate on the EMG-force relationship. Most early studies have shown a simple linear or non-linear relationship between integrated EMG and force exerted by the muscle during isometric contraction [6, 7], and so did the EMG envelope and feature MAV, as their computation was similar. With the advent of myoelectric control, various EMG features have been proposed, such as time-domain, frequency-domain, time-frequency domain, and nonlinear-domain features, and their calculation was different. Thus, the relationship between a certain EMG feature and force may be complex. Besides, the EMG-force relationship is affected by the muscle’s instantaneous length and contraction speed under dynamic contraction conditions. Therefore, the relationship between a particular EMG feature and dynamic force may be highly nonlinear. This can be evidenced by the fact that the linear model MLR can somewhat estimate the grip force; however, the accuracy was largely affected by the feature type. In comparison, GRNN was able to capture the nonlinearity of the EMG-force relationship; therefore, it can be used as a better alternative. Other suitable algorithms such as Artificial Neural Networks (ANNs) which has been confirmed in healthcare institutions [39, 40], can also be used to build the EMG-force model. The benefit of using machine learning technology is that grip force could be excellent predicted without the complex modelling process.
The estimation results of the regression models using different combinations of muscles in intact subjects were similar to Hoozemans and van Dieen [24], where six muscles, including flexor carpi radialis (FCR), FDS, ECU, EDI, ECRB and ECRL, were investigated. When grip force was predicted using an individual muscle, the low performance of ED was consistent with Hoozemans and van Dieen [24]. However, we found the performance of using ECRB appeared to be the worst. In general, when using more than two muscles, the estimation performance of the regression model became stable, and the grip force was predicted well. However, choosing a combination as a common setting in grip force prediction is difficult because no clear difference was found when more than two muscles were included. Therefore, we recommend that three or more forearm muscles are used in continuous force estimation to achieve higher accuracy.
As we cannot measure grip force from the amputee’s phantom limb, the usual method is to measure force from the contralateral hand during mirrored bilateral training and associate it with EMG signals of the amputated side. The estimation performance of the amputee was a little inferior to intact subjects. This may be partially attributed to that EMG signals are largely affected by amputation, so the performance usually degrades when the approach is applied to amputees. Besides, the mirrored bilateral contractions might not be completely systematic, and the timing inconsistency between the input EMG and target force would also affect the GRNN training phase. Nevertheless, the results were comparable with some other studies related to estimating force from the contralateral limb for amputees. Martínez et al. [15] reported
We performed a pilot study to explore an approach to realize continuous grip force estimation under three forearm postures and obtained satisfactory results for the amputee. The results in the present study did not reach statistical significance in the amputees because we only recruited one amputee in the experiment. Actually, it is more difficult to recruit amputees than intact subjects. However, the promising results of this amputee in mirrored force estimation demonstrated the proposed method is worth further study; therefore, we plan to recruit more transradial amputees in the next step. We also hope to implement our approach in online tasks for further validation, where amputees can grip objects using a myoelectric prosthetic hand.
Conclusions
This paper successfully estimated multiple grip force curves under three forearm postures in intact subjects as well as a transradial amputee. By comparing the performance of two algorithms and six EMG features, a combination of GRNN and TD was finally chosen as the optimal regressor. The final estimation performance was
Footnotes
Acknowledgments
This work was supported in part by National Key Research & Development Program of China (2017YFA0701103), the National Natural Science Foundation of China (U21A20479), the CAS Youth Innovation Promotion Association (2018395), the Shenzhen Basic Research Program (JCYJ20200109114805984), and the Shenzhen Engineering Laboratory of Neural Rehabilitation Technology.
Conflict of interest
The authors have all agreed to the submission of this manuscript for publication and declare no conflict of interest.