
Abstract
BACKGROUND:
Bone fracture is the main consequence of osteoporosis, which may become a neglected disease.
OBJECTIVE:
This study aims to fabricate bovine hydroxyapatite-gelatine (BHA-GEL) based bone-implant with alendronate (ALE) in vivo.
METHODS:
Wistar rats were used for an osteoporotic animal model induced by ovariectomy. There were three groups: negative control, BHA-GEL implant, and BHA-GEL-ALE implant. Each group performed a defect by drilling the femur (diameter of 2.2 mm and depth of 2 mm). Observations on the closure of bone defects were performed by X-ray radiography at the second and sixth week after surgery. The mechanism of bone healing was observed by using hematoxylin-eosin (HE) staining and immunohistochemical technique with anti-vascular endothelial growth factor (VEGF) and anti-alkaline phosphatase (ALP) antibodies.
RESULTS:
The radiograph examination showed the implanted group had accelerated bone growth. In addition, the osteoblast, osteoclast and osteocyte had accelerated migration to the defect area. Moreover, the immunoreactive score (IRS) of VEGF at the sixth week in the BHA-GEL-ALE group was lower than the other groups. Meanwhile, the IRS of ALP in BHA-GEL-ALE was higher compared to other groups.
CONCLUSION:
The BHA-GEL-ALE implant accelerates the healing of bone defect in the osteoporotic rat by increasing the ALP expression and the total number of cells.
Introduction
Osteoporosis is a bone disorder caused by reduced bone mass strength, lowering bone quality and strength [1]. This disease occurs because of the exceeds demineralization of bone tissue. The resorption activity of osteoclasts in bone tissue is higher than the ability of osteoblasts to form a new bone matrix [2]. One of the clinical signs of the disease is a bone fracture. If it is not appropriately treated, the fracture may cause substantial disability and mortality [1].
Bisphosphonate has become a trend in osteoporosis therapy in the last two decades. This is because the selectivity of biphosphonate suppresses osteoclast activity to resorb the bone matric [3]. However, oral drug therapy for a long period may become toxic and cause side effects [4]. Because of this, biomaterials are developed as a component of drug delivery systems [5], and as direct bone implants for fracture healing [6]. Moreover, bisphosphonates have a solid affinity to hydroxyapatite crystals in the bone tissue [7].
Hydroxyapatite is a compound that induces bone regeneration due to its biocompatible, bioactive, osteoconductive, non-toxic, non-inflammatory, and non-immunogenic properties [6, 8, 9]. One of the hydroxyapatite that can be obtained from natural sources is bovine hydroxyapatite (BHA). BHA is superior when compared to synthetic hydroxyapatite [9]. This is because BHA has high porosity, leading to the recruitment and differentiation of bone cells in vivo, thereby making bone matrix synthesis faster [10, 11]. However, BHA is a material that may become easily brittle. Because of this, it is necessary to add a stabilizer polymer in its formulation. Gelatin (GEL) is a polymer with the same polypeptide complex structure as collagen’s amino acids. This material is a mild bonding agent and readily absorbed by the bone tissue microenvironment [12, 13]. Besides, GEL can be used as a membrane where the drug is dispersed in a microencapsulated form, thereby controlling drug release. Because of these properties, GEL is potentially used to deliver osteoporotic drug, such as alendronate (ALE) to the bone tissue [5]. BHA-GEL matrix with local antibiotic gentamicin has been used in a prior study as a drug delivery system. Gentamicin and BHA-GEL as the bone implant were able to inhibit the growth of Staphylococcus aureus in vitro. In addition, this matrix also accelerated bone defect repair in vivo [14, 15].
The ALE treatment promotes bone formation by stimulating the proliferation and differentiation of bone-forming cells and inhibiting osteoclast function [16]. Previous research showed the systemic ALE application using the intraperitoneal region where the subcutaneous did not show a significant difference in bone fracture healing [17]. In addition, oral administration of ALE is overcome with some adverse effects such as the upper gastrointestinal disorder, musculoskeletal pain, hypocalcemia and osteonecrosis [4]. Direct application may be a viable option for securely using ALE. Moreover, there is a lack of information about bone healing therapy of ALE in the BHA-GEL matrix as a bone implant. Therefore, this study aimed to determine the performance of BHA-GEL-ALE bone implant as direct fracture healing agent in vivo.
Materials and methods
The fabrication of BHA-GEL-ALE implant
Implants were made using 10 grams extracted bovine hydroxyapatite (BHA, Universitas Airlangga, Indonesia). The BHA was extracted from bovine bone with high temperature at 1000
Animals
A total of 48 female Wistar rats weighing 200–250 grams were adapted for a week. The rats were randomly divided into 6 groups: group of negative control with the defect without an implant in weeks 2 and 6, group of BHA-GEL implant in weeks 2 and 6, and group with BHA-GEL-ALE implant in weeks 2 and 6. Rats were obtained from the Faculty of Veterinary Medicine, Universitas Airlangga, Surabaya. All rats were placed under a controlled environment, with a temperature of 22.5
All animal experiments in this study were performed according to animal ethics committee guidelines from the Faculty of Veterinary Medicine, Universitas Airlangga, Indonesia. Ovariectomy was performed to obtain the bone model of osteoporosis. Before ovariectomy, rats were anesthetized using a combination of ketamine (25 mg/kg weight) and xylazine (8 mg/kg weight). After that, the hair at the pubic area, arcus costae, and mammary glands were shaved and disinfected the surface area with betadine. Then, an incision was made in the abdomen through the linea alba. A search of the left and right ovaries was followed with the removal of both of them.
Moreover, the ligation procedure was undertaken using an absorbable suture (chromic gut cat) and assured no internal bleeding. The irrigation of the abdominal cavity was undertaken with 0.9% NaCl, then the wound in the peritoneum and the skin were closed with catgut. The suture area was swabbed with betadine and covered with hypafix plaster. For post-op medication, 0.2 ml ampicillin (50 mg/2 ml) was given by injection to avoid infection. The wound care was treated regularly with smearing betadine and changing the plaster every day.
On the 8th week after the ovariectomy procedure, surgery was performed for bone defects and implants. Before surgery, anesthesia was performed with the same method as before, using a combination of ketamine-xylazine and ampicillin injection for infection prevention. After that, the hair on the femur surface was shaved and disinfected with 70% alcohol. The incision was made about 1.5 cm in length until the femur bone was visible. Drilling was carried out at the distal area of the femur with a diameter of 2.2 mm and a depth of 2 mm defect. After that, the cavity was irrigated with normal saline, and the wound was sutured with catgut. The suture area was cleaned with betadine and covered with hypafix plaster. Wound care was given regularly with betadine swabs and changing of the plaster.
At weeks 2 and 6 after surgery, rats were terminated with a lethal dose of ketamine-xylazine (3 times anesthetic dose). Moreover, the femur bone was taken and soaked in 10% formalin buffer. Furthermore, bone decalcification was done by soaking in 10% EDTA solution pH 7.4 at room temperature until the bones become soft.
Radiology examination
Observations of the bone integrity and closure of the defect were conducted by X-ray radiography and clarified using ImageJ 1.52a (Wayne Rasband National Institutes of Health, USA).
Immunohistochemistry
Histological examination was performed by making paraffin blocks for each bone sample, starting with dehydration the samples using graded alcohol (30% to absolute) for 60 minutes each. Clearing using xylol three times for 15 minutes each. Infiltration with liquid paraffin three times for 60 minutes in an incubator at 60
Immunohistochemistry performance was conducted to stain VEGF and ALP immunopositive cells based on the procedure by Budiatin et al. [14]. Briefly, the tissue slides were deparaffinated with xylol three times for 5 minutes each, hydrated with serial alcohol (absolute to 70%) for 4 minutes each, and then rinsed in running water for 5 minutes. Then, the slides were dripped with endogenous peroxidase 0.3% H
Haematoxylin-Eosin staining
Haematoxylin-Eosin staining on tissue slides was performed based on Budiatin et al. [14]. Briefly, the slide was dipped with xylol 3 times for 5 minutes each and hydration with serial alcohol (absolute to 70%) for 2 minutes each. Washed with distilled water for 3 minutes, then put in Mayer’s haematoxylin for 15 minutes. Wash under running water and examine under a microscope. After that, the slides were immersed in a 1% eosin solution for 30 seconds, dehydrated, and cleared, followed by mounting with the EZ mount. This method was used to perform the amount of osteoblast, osteocyte, and osteoclast.
Observation of each cell was carried out by morphological identification. To illustrate, osteoblast generally has a round shape and line on the bone surfaces. The osteocytes have flattened shape buried in the bone matrix. The osteoclast has typically larger in size than other cells and the shape is dendritic.
Statistical analysis
Saphiro-Wilk test was used to determine the normality of data distribution. Then, Levene’s test was used to determine the homogeneity of data variance. One-Way ANOVA was used to assess the significance of ALP immunoreactive score and histological staining with haematoxylin-eosin. Kruskal-Wallis test was used to analyze the significance of VEGF immunoreactive score. All statistical tests were performed using SPSS version 21.0 software (IBM Corp., Armonk, NY, USA).
Results
The in vivo performance of BHA-GEL-ALE implant was conducted on the osteoporotic rat. The observations were made on the three groups: negative control, BHA-GEL, and BHA-GEL-ALE. Evaluations were performed with X-ray radiographs, histological staining, and immunohistochemistry technique. This study showed that the application of bone implant accelerated bone growth at the defect site compared to the negative control group. Moreover, in the 6th week, the implant has begun to fuse with the surrounding bone. However, the defect has not closed completely (Fig. 1).
Radiograph of femur rats in each group. The orange arrow represents the location of the defect. The implanted group showed the implant has begun to fuse with the surrounding tissue of the bone.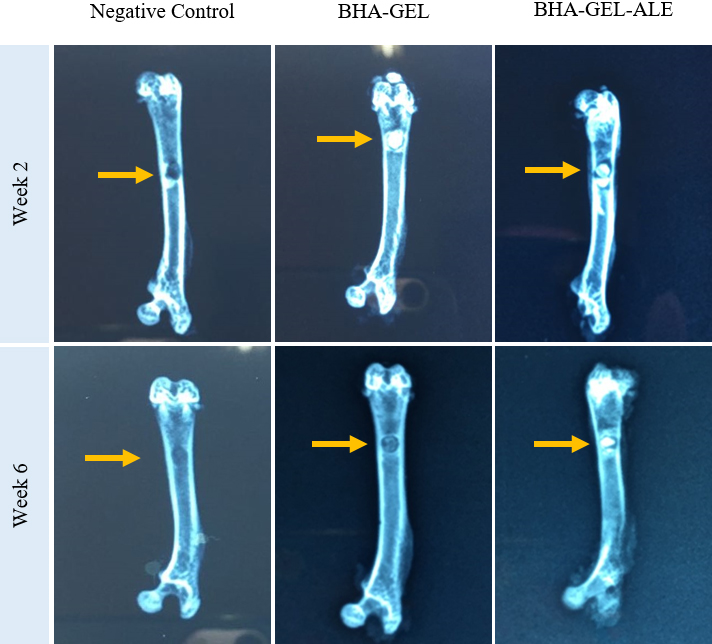
Immunopositive cell with anti-VEGF shown brown color cell in femur tissue (Fig. 2a). The negative control group in the sixth postoperative week showed a higher IRS value than the other groups. Meanwhile, VEGF expression of BHA-GEL-ALE showed a lower IRS value than the other groups (Fig. 2b). Like VEGF, the brown cell in the femur section indicated positive anti-ALP immunostaining (Fig. 3a).
(a) Representative immunostaining section in the observed area. Osteoblast expressing VEGF (black arrow); (b) Immunoreactive score (IRS) of VEGF in each group. Each bar represents the mean IRS 
(a) Representative immunostaining section in the observed area. Osteoblast expressing ALP (red arrow); (b) Immunoreactive score (IRS) of ALP in each group. Each bar represents the mean IRS 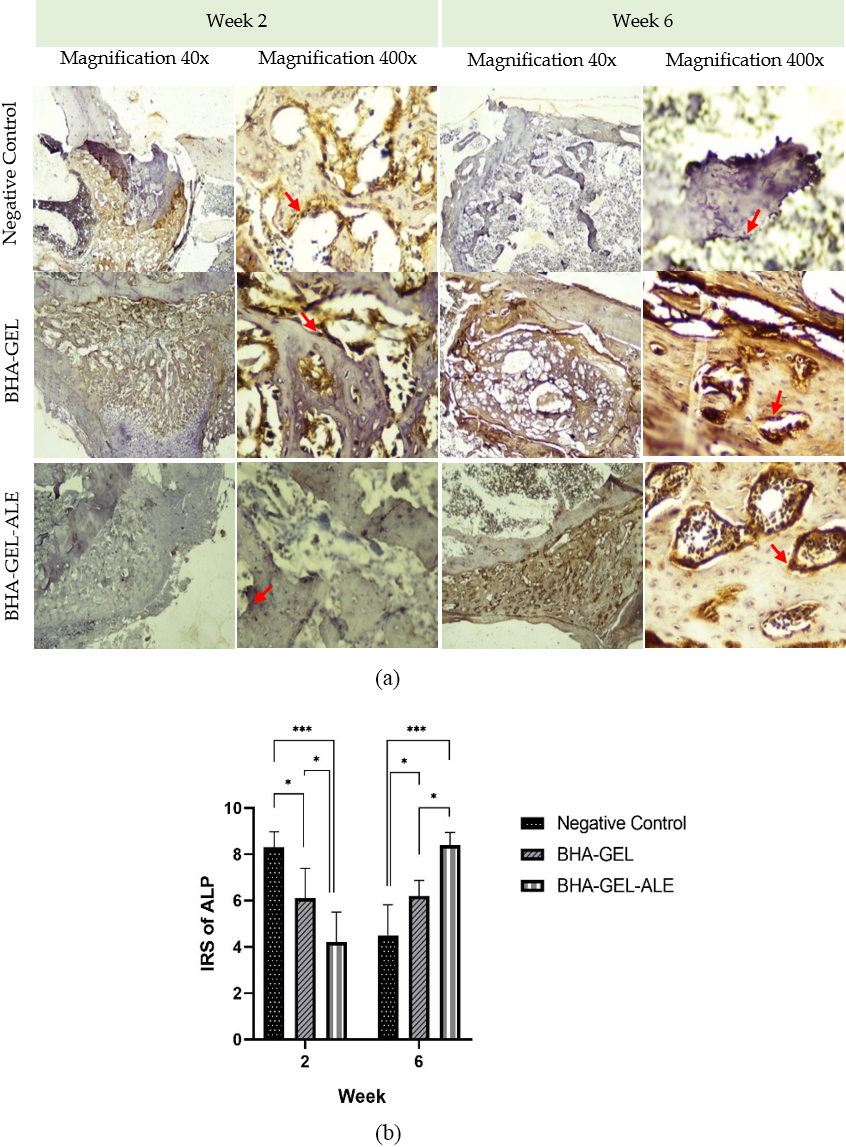
Examination with anti-ALP in each group showed a significant difference. On the one hand, the negative control group showed a higher IRS value than the other in the second week. On the other hand, the BHA-GEL-ALE group showed a higher IRS value than the other two groups (Fig. 3b).
Based on semi-quantitative morphological data, it can be seen that osteoblasts in the second week of implanted BHA-GEL-ALE had significant results. Compared to the negative control, at week 6 there was a significant difference between negative control and implanted treatment, the presence of osteoblast BHA-GEL-ALE was the highest among the others. In osteocytes at week 2, there was a significant difference between the negative control and BHA-GEL-ALE. Furthermore, in the sixth week, osteocytes in the BHA-GEL-ALE sample significantly increased compared to other treatments. The presence of osteoclasts in the 6th week of BHA-GEL-ALE treatment had a significant difference compare with BHA-GEL (Fig. 4). Thus, the application of BHA-GEL-ALE implants affect the number of bone cells during the healing process.
The number of osteoblast, osteocyte, and osteoclast in each group. Each bar represents the mean of total cell 
Osteoporosis occurs due to an imbalance in the bone remodeling process. An increase in the resorption activity by osteoclasts without the rise of osteoblast activity increases the loss and ultimately causes bone tissue loss. This imbalance occurs because of the decrease of estrogen hormone production, also known as estrogens deficiency [18, 19].
In this study, Wistar rats were used as experimental animals. To create an estrogen deficiency condition, an osteoporosis model was made by ovariectomy procedure. The previous research in rats reported that at week 8 after ovariectomy, there was a loss of bone mass or the development of osteoporosis due to an estrogen imbalance [20]. Bone tissue functions as an endocrine organ and plays a role in global minerals. Therefore, in osteoporosis conditions, removing ovaries will decrease the production of estrogen hormone and cause bone resorption and demineralization of the bone matrix [21, 22]. Observation of defect closure qualitatively by using an X-ray radiograph shows a process of bone growth in both implanted bones. In the sixth week, the bone remodeling process remains reverse or transform from the resorption process to the formation process [23]. This is because the combination of organic and inorganic components in BHA-GEL makes it suitable for drug delivery. Moreover, those materials are biocompatible, osteoconductive, and synthesized bone matrix and bone mineral substitutes [14, 22, 24].
Bone remodeling begins when clotted blood caused by inflammation is replaced by fibrous tissue and cartilage bone formation occurs (known as soft callus) that takes time around weeks 1–2. Then, the soft callus is gradually replaced by firm bone as the healing process advances (known as a hard callus) in 4–6 weeks. A prior study reported that bone defect formation begins noticeably in weeks 2–3 [25].
Bone is a highly vascularized organ that angiogenesis plays a vital role in osteogenesis. Vascular endothelial growth factor (VEGF) is one of the most important growth factors in regulating vascular growth and angiogenesis. Angiogenesis is a substantial stage in bone healing because it can provide nutrients and components needed by osteoblasts. In addition, an adequate blood supply to bone tissue can provide the cells and cytokines needed in the fracture healing process [26, 27, 28]. In the current study, the BHA-GEL-ALE group exhibited lower VEGF expression compared to the others. This is because VEGF is widely expressed in the early phase of healing, the inflammatory phase, and soft callus formation. Moreover, in the sixth-week group, the healing process has entered a phase where VEGF is no longer expressed in large quantities. Thus the VEGF expression is difficult to observe [29, 30].
ALP is an enzyme that is important in the differentiation process of osteoblasts. This protein is widely used as a marker for bone formation. Based on the result of the current study, in the second week, BHA-GEL-ALE had the lowest expression of ALP compared to the others. However, in the sixth week, the expression increased and became the highest compared to the others. This may be influenced by high osteoblast migration in the BHA-GEL-ALE group at the sixth week, in line with the HE section. Moreover, ALP is elevated at the stage of bone mineralization in the third week after a fracture. Increased ALP expression and development lead to substantial rules on the mineralization process of bone formation and therapeutic possibilities for the treatment of bone fracture [31, 32].
Furthermore, the highest number of osteoblast and osteocytes in the sixth postoperative week influenced bone remodeling. The high osteoblasts and osteocytes in the BHA-GEL-ALE group indicate alendronate lead in bone integrity at the defect area. BHA-GEL matrix has a high porosity that eases the penetration of the surrounding cells, and the implant binding plays an important role in supporting cell migration and bone growth [10, 15]. This resulted in the bone remodeling endpoint stage in the sixth week. This is because hydroxyapatite as a biomaterial may interact with the osteoblast cell membrane and activates a particular signaling pathway that mediates the remodeling process [9]. In accordance with the previous finding reported BHA-based biomaterials developed with various ions contributed to their osteoimmunomolatory in bone regeneration [33]. There has been studied that in the early stage of bone remodeling, cells will suffer with the hypoxic condition. In this situation, hydroxyapatite bioceramics can encourage the osteoblast proliferation by elevating the level of ALP and VEGF [34].
There have been reported that both bone markers such as VEGF and ALP showed that alendronate could enhance osteogenesis [24, 35]. However, another technique to examine the osteogenic properties in advance can be undertaken by predicting the molecular mechanism. It is also necessary to undertake further research with the molecular mechanism of alendronate to provide an alendronate signaling pathway such as BMP2 that induces bone regeneration [36].
Conclusion
This study investigated the effectiveness of BHA-GEL-based implant incorporation with ALE in osteoporotic bone remodeling. The sixth week X-ray radiography revealed that the materials were beginning to fuse with the surrounding bone, forming the first signs of bone disclosure through the defect. However, the defect was not closed perfectly. VEGF expression of BHA-GEL-ALE showed a lower IRS value than the other groups in the sixth week, suggesting that the bone remodeling via vascularization was less apparent than the several early weeks of bone healing. Moreover, this recent finding showed that the BHA-GEL-ALE implant significantly accelerates bone remodeling by inducing ALP expression and bone cells differentiation. Thus, ALE can be used as a direct bone healing agent with the support of the BHA-GEL matrix. Furthermore, it is recommended to observe more than sixth week in order to demonstrate complete bone remodeling. Additionally, it is also necessary to investigate the other molecular mechanisms through signaling pathway which contributed to the bone healing process in order to discover more about the effects of ALE administration via BHA-GEL-based implant.
Funding
This study was supported by the Ministry of Research and Technology of the Republic of Indonesia, through the basic excellence research schemes (PDUPT) for fiscal year 2021 (Grant no. B/112/E3/RA.00/2021).
Data availability statement
All the data used in this study are included in this published article.
Footnotes
Acknowledgments
The author thanks the Department of Clinical Pharmacy, Faculty of Pharmacy, Universitas Airlangga for all facilities and technical support during the research.
Conflict of interest
The authors report that there are no potential conflicts of interest.