
Abstract
BACKGROUND:
Patients with tracheotomy are often monitored in the anesthesia recovery room after reoperation. During this period, oxygen therapy is necessary, and the existing tracheostomy oxygen supply device has many defects.
OBJECTIVE:
To evaluate the efficacy of a self-made tracheostomy oxygen delivery device on oxygen therapy during postoperative anesthesia recovery.
METHODS:
Patients were randomly divided into two groups, E and C, with 30 patients in each group, and admitted to the post-anesthesia care unit (PACU). Patients in group E received oxygen through a self-made tracheostomy oxygen delivery device, while patients in group C were supplied oxygen through a unilateral nasal cannula. Respiration (R), pulse oximetry (SpO2), and the number of patients on ventilators were recorded at the time of admission (T0) and one hour after admission (T1). Rapid dry blood gas analyses were performed on 0.6 ml samples of arterial blood collected at T0 and T1.
RESULTS:
Compared to group C, patients in group E had significantly higher arterial partial pressure of oxygen (PaO2), arterial oxygen saturation (SaO2), total carbon dioxide (T-CO2), and actual bicarbonate (AB), while arterial partial pressure of carbon dioxide (PaCO2) was significantly reduced (
CONCLUSION:
We found that using the self-made tracheostomy oxygen delivery device in postoperative anesthesia recovery had advantages such as a secure connection to the tracheostoma, adjustable oxygen concentration, air filtration, and the ability to switch oxygen supply between the ventilator and humidifier.
Keywords
Introduction
A tracheotomy is an emergency procedure to rescue critically ill patients or improve ventilation before laryngeal surgery [1, 2, 3]. After the procedure, patients often require the placement of long-term metal kits or disposable tracheal cannulas [4]. Post-tracheotomy, most patients are closely monitored and managed in the intensive care unit (ICU) or the post-anesthesia care unit (PACU) until relevant physiological parameters stabilize, after which they are transferred to standard care units [5]. Oxygen therapy is vital during this postoperative period. However, conventional tracheostomy oxygen delivery devices have several drawbacks, including a large interface with the skin of the neck, suboptimal sealing performance of the tracheostomy kit, a lack of adjustable oxygen concentration on demand, and the inability to seamlessly switch oxygen supply between the ventilator and humidifier (Table 1) [6]. At present, there is no latest technology about self-made tracheostomy oxygen supply equipment. In order to improve the oxygen supply conditions of such patients and overcome the above defects of the current tracheostomy oxygen supply equipment, it is necessary to develop a new oxygen supply equipment to provide oxygen for patients with tracheostomy in the recovery period of anesthesia. Consequently, we manufactured a tracheostomy oxygen delivery device for oxygen therapy during postoperative anesthesia recovery. The clinical outcomes following the use of this self-made device are reported in the sections that follow.
Comparison of different tracheotomy oxygen delivery devices
Comparison of different tracheotomy oxygen delivery devices
General information
This study was approved by the Medical Ethics Committee of the Sichuan Provincial Bayi Rehabilitation Center (Approval No. CKLL-BY2021003), with all participants giving their signed informed consent. The sample included 60 patients who underwent surgery and also had a tracheostomy procedure done at the Sichuan Provincial Bayi Rehabilitation Center between January 2022 and December 2023. There were 38 male and 22 female patients, aged 19–64 years, with a body mass index (BMI) ranging between 21.0–32.5 kg/m2. The surgeries that were performed included 28 cases of cranial repair, 14 cases of ventriculo-peritoneal shunt, 10 cases of transurethral ureteral or bladder lithotripsy, and 8 cases of laparoscopic cholecystectomy. All patients were transferred to the PACU postoperatively.
The inclusion criteria were as follows: (1) patients who were in a persistent vegetative state (PVS) or minimally conscious state (MCS); (2) those who had undergone a preoperative tracheostomy; and (3) their health status grading was American Society of Anesthesiologists (ASA) grade IV.
The exclusion criteria were as follows: (1) patients who had a fever or lung infection in the last two weeks; (2) patients postoperatively transferred to the ICU or general ward; and (3) patients whose SpO2 was
The enrolled patients were randomly divided into the following two groups: the self-made tracheostomy oxygen delivery device group (group E) and the unilateral nasal cannula group (group C), with 30 cases in each group.
There was no statistically significant difference in gender, age, BMI, or type of surgery between groups E and C (
Comparison of general information between the two groups (
30)
Comparison of general information between the two groups (
Note: ∗ Fisher’s Exact Test; R: Respiration, BMI: Body mass index.
Upon the patient’s admission to the operation room, electrocardiography, blood pressure, pulse oximetry (SpO2), and bispectral index (BIS) were monitored. A quantity of 0.3 mg of pentylenetetrazol hydrochloride was administered intravenously. Radial artery catheterization was done to enable measuring pressure under regional anesthesia.
Anesthesia induction was standardized across both groups, as detailed below: Initially, patients received 0.03 mg/kg of midazolam intravenously, followed by 0.3
Upon completion of the surgery, anesthesia drugs were discontinued. Subsequently, 1 mg of neostigmine and 0.5 mg of atropine were administered intravenously to counteract residual muscular relaxation following spontaneous respiration recovery. Tracheotomy tube replacement was then performed, and patients were transferred to the PACU for continuous monitoring of their electrocardiogram, blood pressure, and SpO2. Oxygen supplementation was provided via either the self-made tracheostomy oxygen delivery device (utilizing the small-diameter ventilation end) in group E or the unilateral nasal cannula via the tracheostoma in group C, with an oxygen flow rate of 2 L/min maintained in both groups. In cases where the SpO2 remained below 92% for 3 minutes, oxygen supplementation was done either through the self-made tracheostomy oxygen delivery device (utilizing the large-diameter vent) connected to the ventilator in group E or directly via the ventilator in group C.
Observational indexes
The R, SpO2, and number of patients on ventilators were recorded at two time points: T0 and T1. Rapid dry blood gas analyses were conducted using 0.6 ml of arterial blood collected at T0 and T1 utilizing the i15 biochemical blood gas analyzer, Edan Instruments, Inc., Shenzhen.
Statistical analysis
Analysis was performed using SPSS 25.0 statistical software. Quantitative data were expressed as the mean
Results
Process of manufacturing the tracheostomy oxygen delivery device
The tracheostomy oxygen delivery device consists of an inlet pipe, a reservoir bag, and an outlet pipe, which are interconnected. In order to enable seamless switching of oxygen supply between the ventilator and humidifier, the large-diameter vent connection of the inlet pipe is connected to the ventilator pipeline, or the small-diameter vent connection is connected to the connection pipe of the humidifier bottle. Additionally, the cone-shaped outlet pipe is attached to the tracheostomy kit. The inlet pipe and outlet pipe are connected through the reservoir bag, which is equipped with an air control valve and a filter layer (Patent No.CN2020201390782 and No.CN202020300432887) [7, 8] (Figs 1 and 2).
Diagram of the self-made tracheostoma oxygen delivery device. Note: 1: Inlet pipe, 11: Large-diameter vent connection, 12: Small-diameter vent connection, 13: Large-diameter cap, 14: Small-diameter cap, 15: Vent pipe, 2: Reservoir bag, 3: Outlet pipe, 31: Outlet cone-shaped pipe, 32: Outlet thread hose.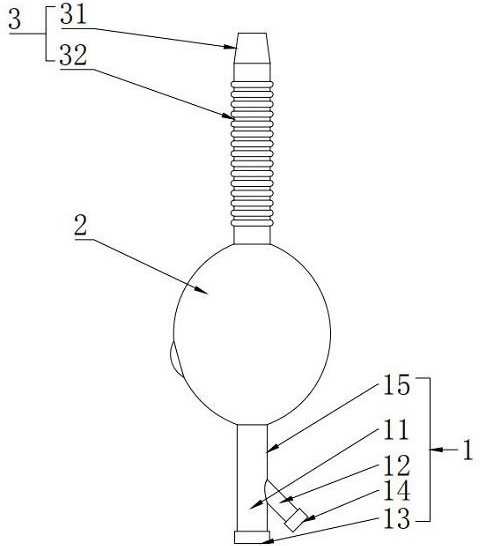
Diagram of the reservoir bag and air control valve. Note: 2: Reservoir bag, 21: Air control valve, 211: Rotatable shutter, 2111: Adjusting orifice, 2112: Adjusting knob, 212: Hole layer, 213: Filter layer.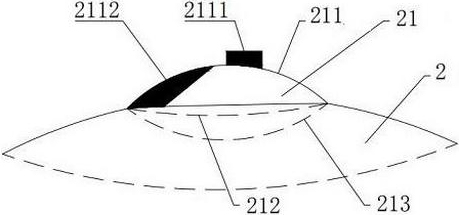
The two groups did not differ significantly with respect to R, SpO2, and the number of patients on ventilator at T0 and T1 (
Comparison of R, SpO2, and ventilator use at T0 and T1 between the two groups (
30)
Comparison of R, SpO2, and ventilator use at T0 and T1 between the two groups (
Note: ∗ Fisher’s Exact Test; R: Respiration, SpO2: Pulse oximetry.
The levels of PaO2, SaO2, T-CO2, and AB increased while PaCO2 decreased at T1 in group E compared to group C, with the difference being statistically significant (
Discussion
The tracheostomy oxygen delivery device used in this study is produced by Henan Tuoren Medical Equipment Group Co., Ltd, China. The silicone or plastic materials used comply with the relevant standards of GB/T16483-2008 and regulations, including biocompatibility, chemical stability, physical properties, antibacterial properties, toxicological information, ethylene oxide sterilization, disposable use, and disposal of medical waste after use, to ensure that there are no adverse effects on the health of patients.
In the case screening of this study, the surgical categories include cranial repair, ventriculoperitoneal shunt, transurethral ureteral or bladder lithotripsy, and laparoscopic cholecystectomy. Although the types of operations are different, they all have a common feature, that is, tracheostomy has been performed before the operation, and the operations are carried out under general anesthesia. After the operation, tracheal cannula is replaced and oxygen is given through tracheostomy, which ensures the correlation between the research and study outcomes.
In a previous study [9], we developed a PACU transfer-out assessment scale specifically designed for patients in PVS or MCS. This scale underwent rigorous reliability and validity testing. The Respiration, Circulation, Oxygenation, Bispectral index, and muscle relaxation scale (RCOBN scale) was used for the evaluation of postoperative PACU transfer-out readiness for such patients. As per the norms of this scale, only patients achieving a total score of eight points are deemed eligible for being transferred out of the PACU. Oxygenation is an important patient evaluation index. However, achieving consistent alignment between oxygen supply devices and tracheostomy kits poses a challenge with existing oxygen delivery devices. Hence, we developed a tracheostomy oxygen delivery device tailored for oxygen therapy during the postoperative anesthesia recovery in this patient population.
As seen in this study, the baseline measurements of R, SpO2, and blood gas indexes were generally comparable between the two groups, E and C, at T0, as was the number of patients on ventilators. After 1 hour of oxygen supply through different apparatuses, there was no evident change in the values of R and SpO2 in either group, and blood gas indexes also remained within the normal range. However, at time point T1, the levels of PaO2, SaO2, T-CO2, and AB in group E were elevated, while PaCO2 declined when compared with group C. Furthermore, when compared to baseline values within each group, PaO2
Comparison of blood gas analysis parameters at T0 and T1 between the two groups (
,
30)
Comparison of blood gas analysis parameters at T0 and T1 between the two groups (
Note: Compare with T0, aP < 0.01, bP < 0.05; PH: Pondus Hydrogenii, PaO2: Arterial partial pressure of oxygen, SaO2: Arterial oxygen saturation, PaCO2: Arterial partial pressure of carbon dioxide, T-CO2: Total carbon dioxide, SB: Standard bicarbonate, AB: Actual bicarbonate.
decreased in both groups at T1, PaCO2 decreased in group E, while SaO2, T-CO2, and AB decreased in group C at T1.
The traditional unilateral nasal cannula placed at the tracheostoma is an open type of oxygen supply. Despite providing constant oxygen flow, achieving an optimal oxygen concentration remains challenging in this modality due to the mixing of oxygen with ambient air at the tracheostoma [10]. Additionally, the prolonged use of disposable tracheotomy cannulas with cuffs has been associated with complications such as adhesion of the endotracheal wall and cuff, as well as granulation formation, leading to difficulties in extubation and the need for reoperation [11, 12]. While metal catheters are often used to mitigate these issues, the orifice not aligning with the respiratory circuit port hinders effective oxygen supply from the ventilator.
However, the self-made tracheostomy oxygen delivery device addresses these challenges by enabling switchable oxygen supply between the ventilator and humidifier as needed through the connection between the inlet pipe of the oxygen delivery device and the pipeline of the humidifier or ventilator. Furthermore, it facilitates compatibility with various tracheostoma catheters, thereby overcoming issues associated with cuff adhesion and granulation formation. Moreover, the device resolves the problem of a large interface between the oxygen mask and the skin of the neck by connecting the cone-shaped outlet pipe of the oxygen delivery device with the tracheostoma catheter. In addition, an air control valve and filter layer are integrated above the reservoir bag. The former allows for adjustment of the concentration of inhaled oxygen and exhaled carbon dioxide, while the latter functions similar to an artificial nose to filter out airborne dust, thus aligning with hospital infection management requirements.
As a consequence of machine-controlled respiration during surgery and the administration of high oxygen concentrations during anesthesia, the levels of PaO2 at T1 were observed to be lower than those at T0 in both groups, despite similar pH values within the normal range. Oxygen was delivered via the self-made tracheostomy oxygen delivery device for patients in Group E, which effectively mitigated air dilution through its air control valve, resulting in increased effective oxygen concentration. This led to an increase in PaO2 and SaO2 in group E, along with a decline in PaCO2 at T1 when compared with group C. Influenced by both respiration and metabolism in vivo [13], T-CO2 reflects the sum of blood carbon dioxide (CO2) and bicarbonate (HCO3ï¼). In cases of metabolic acidosis, it decreases significantly, while in cases of alkalosis, it increases significantly [14]. Therefore, in group E, T-CO2 increased as PaCO2 decreased. Additionally, reflecting the actual content of HCO3 ï¼, there was an increase in AB levels at T1 due to the respiratory influence.
It is important to note that although there were differences in the blood gas values of the two groups at T1, no significant differences were observed with respect to R or SpO2. According to the oxygen dissociation curve [15], when PaO2 is
In conclusion, the utilization of the self-made tracheostomy oxygen delivery device for oxygen supply in anesthesia recovery holds significant potential in clinical settings. This device is composed of an input pipe, an air storage bag and an output pipe, wherein the input pipe can be connected with the ventilator pipe or the humidification bottle connecting pipe, the output pipe is connected with the tracheostomy kit, and the air regulating valve and a filter layer are set on the air storage bag. This device was found to offer several advantages, including a secure connection to the tracheostoma, the ability to adjust oxygen concentration, air filtration capabilities, and the option for switchable oxygen supply between the ventilator and humidifier. This is more conducive to improving oxygenation, and these features collectively contribute to enhanced patient care and recovery outcomes, highlighting the suitability of the device for widespread clinical use and promotion.
Funding
Health Commission of Sichuan Provincial (No.: 19PJ255).
Ethics approval and consent to participate
This study was conducted with approval from the Ethics Committee of Sichuan Provincial Rehabilitation Hospital (No. CKLL-BY2021003). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Author contributions
Conception and design of the research: Yi-ying Xiong, Ze-yu Zhao.
Acquisition of data: Yi-ying Xiong, Chao-yang Chen, Xiang Li, Xin-xin Yue.
Analysis and interpretation of the data: Xiang Li, Xin-xin Yue.
Statistical analysis: Xin-xin Yue, Ze-yu Zhao.
Obtaining financing: Ze-yu Zhao.
Writing of the manuscript: Yi-ying Xiong, Chao-yang Chen.
Critical revision of the manuscript for intellectual content: Ze-yu Zhao.
All authors read and approved the final draft.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.