
Abstract
Keywords
Introduction
Vestibular implants have been successfully used experimentally to drive eye movements in primates using gyro recordings of head angular velocity coded in electrical stimulation rates of the vestibular nerve [17, 32]. The primary goal of these implants has been the restoration of vestibular-ocular reflex (VOR) function, seldom improvement of balance control [32]. The reason for this emphasis could be due to variations in electrical stimulation thresholds necessary to elicit a VOR response [17, 37], the lack of consistency between electrically elicited eye and postural movements in human subjects [36], or problems in comparing animal and human modes of postural control [3]. The predominant reason, however, could be the clinical assumption that deficits in VOR function are strongly correlated with deficits in balance control [22] to which vestibule-spinal reflexes (VSR) contribute. Recent evidence [7, 8], however, suggests that the correlation is, in fact, weak. Moreover, balance control of the elderly is more affected by peripheral vestibular loss than that of the younger despite an equal influence in the young and elderly on VOR function [39]. Therefore, it can be expected that a risk factor for elderly fallers is vestibular loss [41].
Vibro-tactile (VT) and auditory prosthetic feedback systems which aim to reduce sway during balance tasks have had more than a decade of development [11, 44]. The VT feedback is either applied at the head [15] or over muscles around the waist, where the VT simulation can also induce, via cutaneous receptors, a direct effect on body sway [27]. The emphasis in all of the aforementioned studies has been the reduction of trunk or body sway with no measurement on eye movements to determine if the VOR has also improved. Reductions in trunk sway have been shown in the elderly population [15, 28], those with vestibular loss [5, 40] as well as those with Parkinson’s disease [33] or multiple sclerosis [42]. In VT feedback studies the effect of muscle activity on the recipients movement patterns leading to reduced sway has, with one exception [23], not been studied.
A study of muscle activity during VT and/or auditory feedback or during stimulation with a balance implant would provide direct evidence that vestibular subjects are actively producing instability during specific tasks. Such active driving of instability has been established for balance corrections to perturbations of stance in humans [3, 12] and cats [30]. However, active driving of instability to quiet unperturbed stance has not been examined according to our knowledge.
One of the most common forms of testing balance control during stance is to ask test subjects to stand on a foam pad with eyes closed [35]. Under these circumstances patients with balance deficits are unstable or may fall, generally backwards [2] because the foam support surface reduces the efficacy of lower-leg proprioceptive sensory contributions to balance control and visual inputs are blocked due to eye closure. The magnitude of the increased sway is similar to that achieved by servoing-out ankle inputs to balance control during quiet stance [10]. Information on the muscle activity of bilateral vestibular loss (BVL) subjects during quiet standing eyes closed on foam (ECF) in comparison to healthy controls would increase our knowledge on the pathological mechanisms involved in instability following vestibular loss. Furthermore, a demonstration that activity patterns of BVL subjects improved, becoming similar to those of healthy controls, with VT and auditory biofeedback of trunk or head sway, would provide evidence of prosthetic device efficacy. Recordings of muscle activity under these circumstances might provide a means to compare balance implants and VT balance prostheses. Therefore, the goal of this study was to record and quantify muscle activity during the eyes closed on foam (ECF) balance task. We chose muscles to record from those known to be modulated by vestibular loss during moving support surface tests [4, 13]. Specifically we recorded from the ankle muscles tibialis anterior and soleus as well as the trunk muscles paraspinals and external obliques under the assumption both sets of muscles contribute to motion about the ankle joints and the lumbo-sacral joints during quiet stance [26].
Methods
Participants
Thirteen adult subjects (6 bilateral peripheral vestibular loss (BVL) subjects and 7 age-matched healthy control subjects) were included in this study. The BVL subjects were out-patients at the University of Basel Hospital, Switzerland. The BVL subjects ranged from 45 to 52 years of age (Mean 48.8; SD 2.2) and the controls ranged from 41 to 53.2 years (Mean age 49.2 SD 4.4). Inclusion criteria for the BVL subjects was the absence of vestibular ocular reflex responses to caloric irrigation with water temperatures of 44 and 30 deg C for both ears, rotating chair (yaw and pitch) responses less than the lower 5% bound of normal subjects. All BVL subjects had normal auditory evoked brainstem potentials and normal pure tone audiograms except one subject whose thresholds were at 70 dB hearing level. All BVL subjects had normal magnetic resonance imaging scans of the brain. The BVL subjects had no other neurological or musculoskeletal impairments that could interfere with balance control. Exclusion criteria for the healthy subjects included any self-reported sensory, neurological or musculoskeletal impairments that could interfere with balance and an inability to stand on one leg, eyes closed, for 20 seconds without falling. All subjects provided informed written consent to participate as required by the ethical committee of the University of Basel Hospital which approved the study.
Testing procedures and data recording
Two gyroscope based systems, SwayStar (Balance International Innovations GmbH, Switzerland), measuring angular velocities in the roll and pitch planes, were used. The gyroscopes typically had a bias drift of 1–2 deg/hr, less than the manufacturer’s specification of 6 deg/hr. One SwayStar system was mounted on a belt strapped around the hips in order to measure pelvis movements. The other system was mounted on a plate placed between the scapulae and held in place with a tightly fitting shoulder harness. The angular velocities were sampled at 100 Hz with 16 bit accuracy over a range of 327 deg/s and then transferred wirelessly to a PC which computed angle changes via trapezoid integration [2]. Because sensor drift was low, no correction was made for drift other than that described in data processing below. Muscle activity was measured with pairs of surface, silver-silver chloride EMG electrodes. These electrodes were placed 3 cm apart, along several muscles: left tibialis anterior and soleus, and bilaterally on external obliques, paraspinalis at L4-L5, and medial deltoid. We report on only left-sided recordings as those on the right arm and trunk yielded similar results. Symmetrical results were expected were expected in the trunk and arm muscles because instability was predominately in the pitch direction (see Figs. 1 and 2). EMG signals were recorded using a preamplifier with a gain of 1000 and a band-pass of 0.7 Hz to 2.5 kHz. These signals were analog band-pass filtered between 60 and 600 Hz, full-ware rectified and low-pass filtered at 100 Hz with a 3rd order Paynter filter prior to sampling at 1 kHz [20].

Illustration of the vibro-tactile and auditory feedback head band. The cable shown is connected into the SwayStar system mounted at the lower back and provides the trunk pitch and roll velocity signals used to actuate the 8 vibro-tactile vibrators spaced around the head and 2 auditory bone conductors mounted just above the ears.
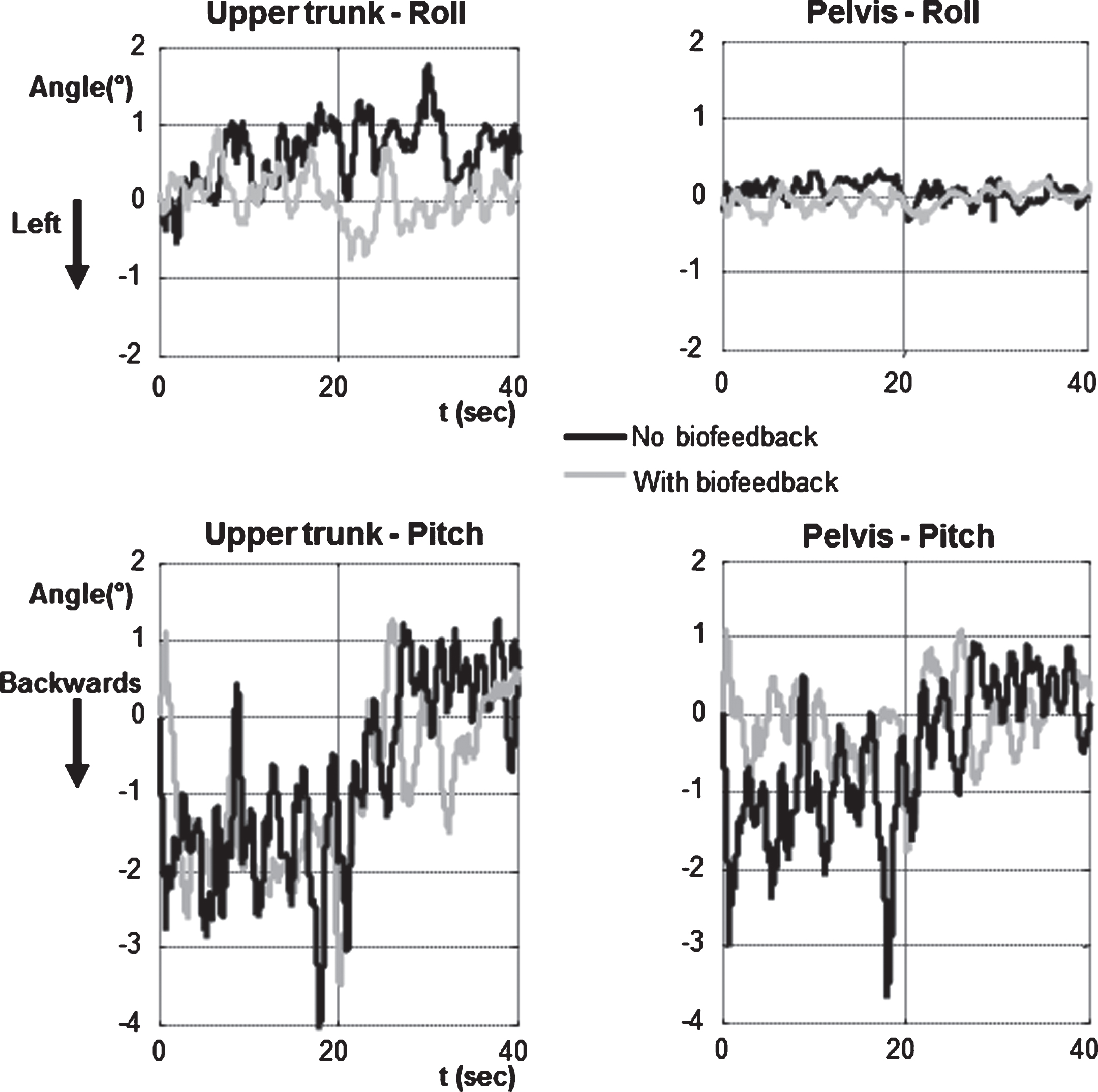
BVL subject’s upper trunk and pelvis angles recorded while standing feet shoulder width apart, eyes closed, on foam with and without feedback. The four panels show the sway angles in degrees of the pelvis (2 panels on the right) and upper trunk (2 panels on the left). The lower panels with feedback show pitch plane displacements, the upper traces roll movements. The black no feedback traces show larger peak to peak and motion compared to the grey feedback traces.
A Balance Freedom system (Balance International Innovations) provided feedback of pelvis sway angle to the participants in the form of vibro-tactile and auditory signals using as the feedback input the computed pelvis angles obtained from the pelvis gyroscopes’ angular velocity outputs. Actuators for the feedback were mounted on a head band (see Fig. 1) and were active once pelvis sway angle thresholds for activating respectively the vibro-tactile and auditory actuators were exceeded. The actuator system was placed on the head rather than around trunk muscles at the waist to avoid possible interactions with muscle and cutaneous proprioception [27]. Feedback thresholds were based on individual values of the 90% ranges of pelvis sway in the pitch and roll directions computed for the 70 sec duration (or less) of each task of the first assessment’s sequence of tasks described below. The thresholds in each direction were set at±40% of the 90% range for vibro-tactile signals (that is, a range equal to 80% of the 90% measurement), and at±80% of the 90% range for the acoustic signals. This meant that, for example, the vibro-tactile thresholds were, on average, equal to 40% of the roll and pitch mean angle values shown in Fig. 3 (no feedback or first assessment columns). Thus the values set for the BVL subjects were significantly larger for the eyes closed foam task (see below for task descriptions) than would have been set for the HCs. Once activated, each feedback signal remained active as long as its threshold was exceeded, with the acoustic feedback increasing linearly in amplitude from 50 dB until it reached 70 dB hearing level. The vibro-tactile activation signal was sent to 1 of 8 vibrators in the headband set at 45° intervals around the headband. A vibrator switched on when the sway threshold was reached in the direction of the sway and this direction had the largest sway amplitude. The frequency of vibration was 150 Hz. This is in the middle of the frequency range of maximum sensitivity of skin receptors to vibration [38]. The acoustic feedback consisted of two bone-conducting acoustic actuators placed above the ears at the level of the mastoids. The left actuator was activated at 870 Hz when the acoustic threshold was reached for sway to the left, the right actuator at 500 Hz when swaying to the right, and both conductors with a frequency of 1370 Hz and 250 Hz when swaying backwards and forwards, respectively.

Group angle and angular velocity means of 90% upper trunk and pelvis sway ranges with and without feedback. The column height represents the mean group angle and angular velocity of the upper trunk and pelvis. Values are shown for stance tasks on foam with eyes closed. The vertical lines above each column indicate the standard error of the means. BVL stands for bilateral vestibular loss group, HC for the healthy control group. BVL means with feedback which are significantly less than those without feedback are marked p < 0.05. Those with feedback having greater values than HCs without feedback are also marked p < 0.05.
For each of the two assessments first without and then with feedback, two stance tasks were performed on a foam surface, eyes open and eyes closed and one task eyes closed on a normal surface. We report here only on the eyes closed tasks for which changes in muscle synergies were most significant across sway frequency bands [23]. The foam surface had a height of 10 cm, length 250 cm, width 44 cm and a density of 25 kg/m3. We used a foam surface because this reduces the effectiveness of lower leg proprioceptive inputs controlling balance and makes it very difficult for vestibular loss subjects to avoid losing their balance, especially with eyes closed [1, 25]. Pelvis and trunk sway and EMG signals were recorded for 70 secs during each of the stance tasks. If a loss of balance occurred during a task, the task was repeated a maximum of two times and the trial with the largest duration was used. The tasks were performed without shoes, feet shoulder width apart, and with the arms hanging alongside the body. After the first assessment, subjects rested for 20 minutes. Then, 30 minutes of training was provided with biofeedback. The training tasks were the same as those of the first assessment but also included tandem stance on a firm surface, eyes open and closed so that difficult training tasks were also provided. After another short pause of 5 minutes, subjects were reassessed on the same 3 stance tasks of the first assessment with the feedback active. During all tasks, two spotters stood close behind the subjects in order to prevent a potential fall.
Sway measures for the pelvis and upper trunk were the 90% ranges of sway angle and angular velocity. To determine the histogram required to define the 90% ranges the peak-to-peak range of angle and angular velocity in the pitch and roll directions was divided into 40 bins. For this purpose, data of near falls at the end of recordings associated with large changes in pelvis and trunk sway as well as EMG activity was first excluded.
To compute mean baseline activity over each EMG recording a number of filters were applied to the 1 KHz sampled EMG data. First the data was filtered with an 11 consecutive sample median filter to remove spurious spikes. Then it was band limited by filtering forwards and backwards through the data with a 3rd order Butterworth filter with a cut-off frequency of 150 Hz. Then all local minima were searched for in the data using a running average difference filter over 3 samples forwards and backwards in time. The minima were then traced back to the data stream. The local minima points so obtained were next filtered with a 5 point median filter to narrow the range of minimum points. The samples between the resulting minima points were filled based on a cubic spline interpolation. This process of finding local minima, and cubic spline fit was repeated iteratively further twice to yield a record of baseline activity which was visually verified. The mean area of this activity per sec with respect to zero was then computed for the whole record except the first and last 500 samples (0.5 sec) that were excluded to avoid starting effects or possible falls influencing the data. The amplitude of EMG activity was then the sample per sample difference between the original EMG activity and the computed baseline activity. This amplitude was used to compute the mean area of activity per sec over the complete trial.
Differences between mean sway values were explored with the Wilcoxon signed rank test for within subject comparisons or the Wilcoxon rank sum test for between group comparisons. For all statistics p≤0.05 was defined as significant after a Bonferroni correction for 2 comparisons (BVL with vs. without feedback, BVL with feedback vs. controls without feedback), i.e. p≤0.025 before correction. Differences between population median EMG baseline and amplitude values for BVL subjects with and without feedback were also explored with the Wilcoxon signed rank test or the Wilcoxon rank sum test respectively.
Results
BVL subjects were able to reduce sway angles at the pelvis and the upper trunk using the biofeedback of pelvis sway. Figure 2 provides an example of the improvement for a typical BVL subject who had considerable difficulty to avoid falling backwards when standing eyes closed on a foam surface. This subject as well as other BVL subjects and healthy controls (HCs) had considerably more motion in the pitch compared to the roll plane. Figure 3 shows that BVL subjects achieved an approximately 50% reduction in both roll and pitch motion at the upper trunk and pelvis with biofeedback. Statistical analysis revealed that this reduction in angular motion was to levels not different from those of healthy controls (HC). However, the amplitudes of angular velocities, though significantly reduced some 50% with biofeedback, were still larger than those of HCs (Fig. 3).
In Fig. 3 the angular displacements for the pelvis (which records leg and pelvis motion) were less than those of the upper trunk, regardless of whether the BVL subjects were provided feedback or not. A similar result is observed in Fig. 3 for the HCs. If the body motion in the roll and pitch was similar to that of an inverted pendulum, then the displacements and angular velocities would be equal at the pelvis and upper trunk.
Figure 4 provides an example of the changes in muscle synergies with feedback observed in BVL subjects. Figures 5 and 6 show the median changes in baseline activity and amplitude modulation when feedback of pelvis motion is provided. Two types of changes are observed. Firstly, there is a reduction in the level of background activity which in Figs. 4 and 5 is prominent in the trunk muscles, paraspinals and external obliques. Secondly, there is less modulation of EMG activity above the level of background activity in trunk and ankle muscles (Fig. 6). In contrast, the median background levels and amplitudes of BVL subjects were not significantly reduced with feedback in the soleus muscles. Furthermore, the reduction in the tibialis anterior amplitude in BVL subjects with feedback was not to the level of HC (Fig. 6). In the trunk and arm muscles there was no difference between the levels of HC and BVL subjects with feedback. Thus the effect of feedback was more significant in the trunk and arm than in the ankle muscles.
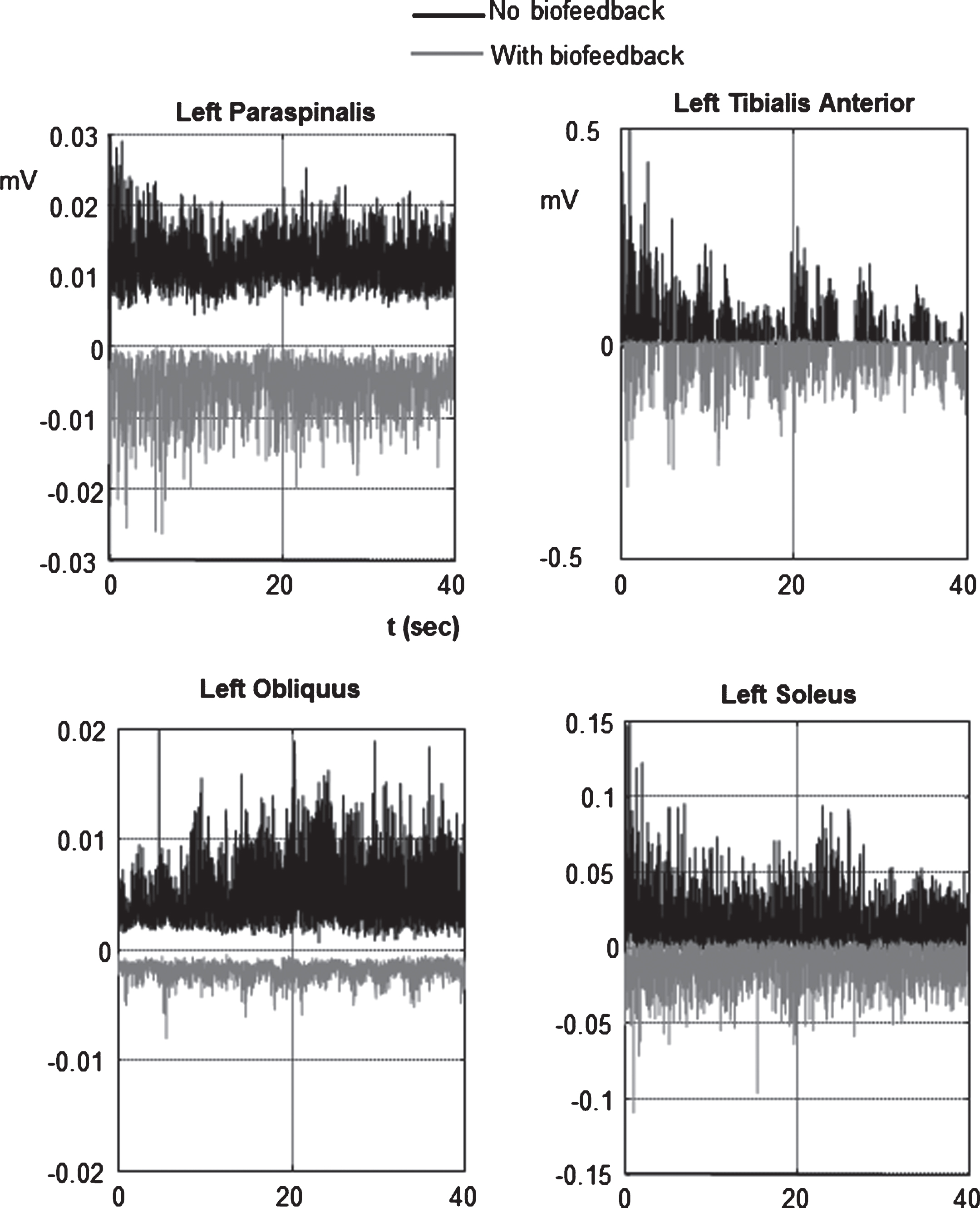
EMG activity of a BVL subject with and without feedback for the task standing eyes closed on foam. The ankle and trunk muscle activity without feedback is shown in the upper traces of each panel, the activity from the same muscles with feedback is shown inverted in each panel.
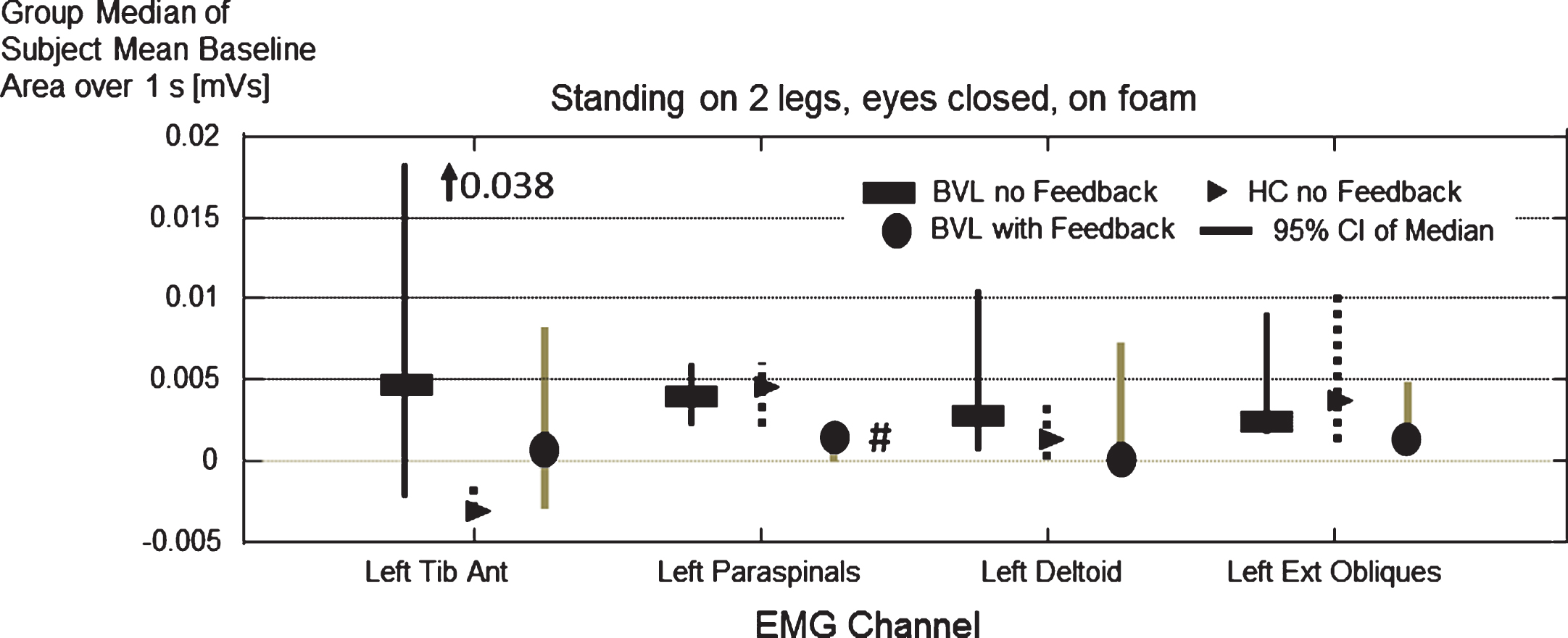
Group median of subject mean EMG baseline per second of trial (standing on 2 legs eyes closed on foam) for 4 left muscles (2 trunk muscles paraspinals and external obliques as well as deltoid and tibialis anterior). All values of the BVL subjects are significantly lower with than without pelvis feedback (p < 0.05). Soleus baseline (not shown) was not altered with feedback. BVL baseline activity with feedback different from healthy controls (HC) is marked with a # symbol (paraspinals, p = 0.02).
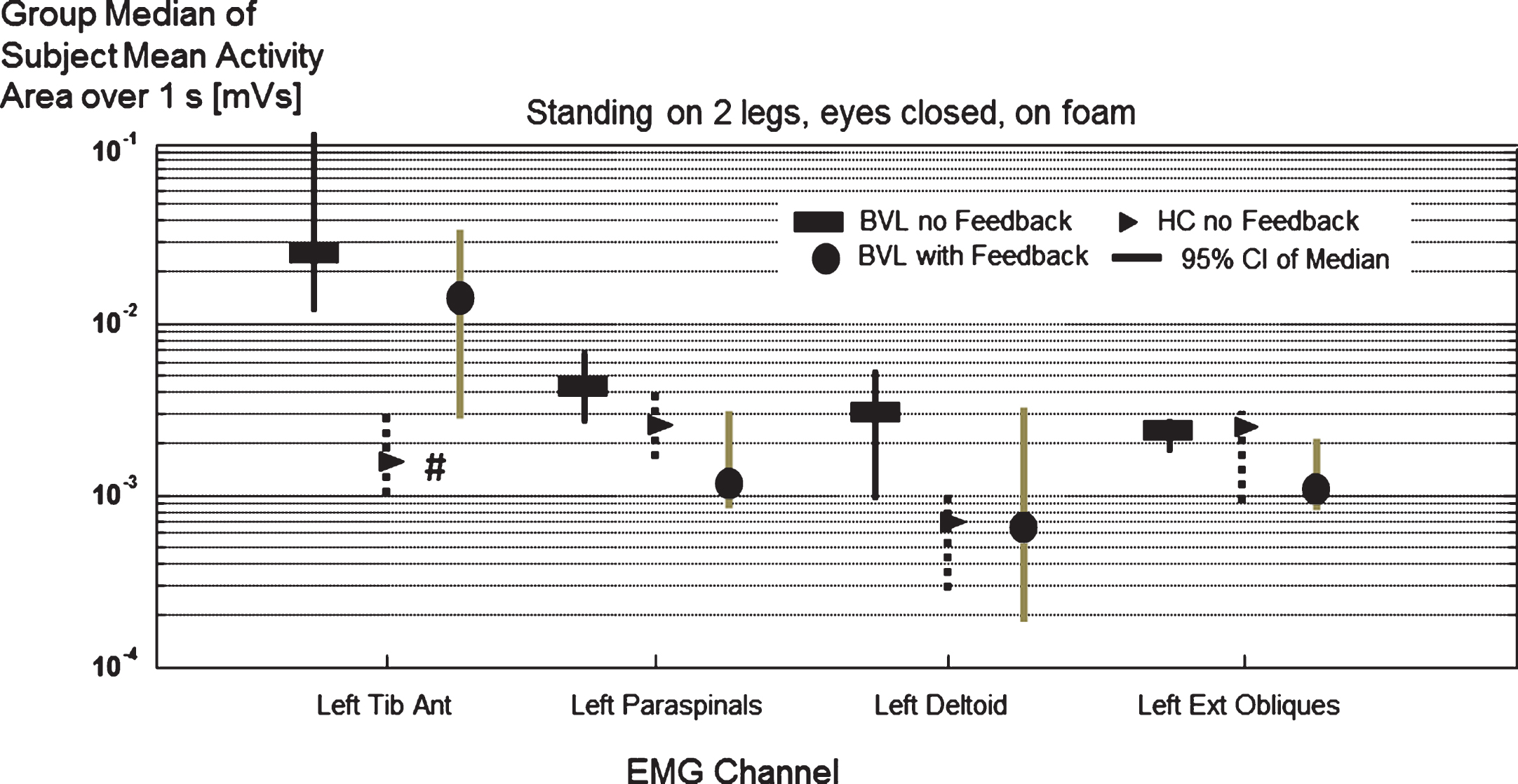
Group median of subject mean EMG amplitude (with respect to baseline) per second of trial. All amplitudes of BVL subjects with feedback are significant lower than without feedback (p < 0.03). Only tibialis anterior EMG amplitude for HC without feedback was lower than BVL subjects with feedback (p = 0.03, marked #).
The results of this study indicate that combined vibro-tactile and auditory feedback of pelvis sway angle leads to improved control of balance for BVL subjects. The improvement was present in the roll and pitch directions and both at the upper trunk and pelvis. Our previous research on the directional sensitivity of feedback on balance control during stance has indicated that improvements are generally larger in the pitch direction for healthy subjects but are dependent on the amount of sway [15]. Further, most if not all of the feedback is vibro-tactile and not auditory due to threshold differences [15, 23]. Therefore we assume that bilateral vestibular loss subjects benefit most by using the vibro-tactile feedback to reduce their pitch sway about the pelvis and upper trunk as movements without feedback are larger in this direction. We have previously shown that vestibular loss subjects overreact at the trunk in the pitch and roll directions when perturbed during stance [12], and provide insufficient pitch control about the ankle joint [6]. That is, active destabilization appears to be greater at the trunk and perhaps for this reason improvement was significant with feedback in the trunk muscles.
Movement strategies with and without biofeedback
The changes in movement amplitudes with feedback occurred without changing balance-correcting movement strategies. That is, the greater sway at the trunk than the pelvis was present with and without biofeedback. Moreover, the movement strategies used with and without feedback were the same as those used by normal subjects. Thus the healthy control subjects (HCs) also had greater motion at the upper trunk than the pelvis. We have argued elsewhere that this greater motion at the upper trunk is due to a bimodal movement strategy [25].
The question arises whether the BVL subjects would have further reduced their movement amplitudes with more training. We have not investigated whether long-term balance training with the feedback alters the amplitudes of movement strategies in BVL subjects. However, it is unlikely that amplitudes would have reduced more over time as the amplitudes of sway of BVL subjects with feedback were similar to those of controls without feedback. We assume that long-term training would have reduced the differences in angular velocity amplitudes between HCs and BVL subjects with feedback.
Changes in muscle synergies with biofeedback: Possible implications for vestibular implants
The amplitudes of both upper trunk (shoulder) and pelvis sway were reduced with pelvis sway feedback by employing two types of muscle action: reduced activity modulation and reduced background activity. Presumably reduced background activity reduces intrinsic muscle stiffness and therefore induces less extensive sway for the same muscle modulation. This effect would be reinforced by smaller muscle modulation.
The reduction in EMG activity with improvement in sway raises the interesting question whether EMG feedback would provide a better feedback parameter than pelvis angular changes as used here. EMG feedback is widely used to control upper limb prostheses. However, force control is equally as effective in controlling prosthetic limb position [14]. Here we used pelvis position as the pelvis CoM is close to that of the whole body CoM and we assumed that this latter variable is controlled by the CNS. It may well be worthwhile considering whether in future studies a dual feedback mode (CoM angular position and trunk EMG) could be used for prosthetic feedback. Such a feedback might be useful for gait tasks where excessive EMG activity may help predict gait instabilities in the next step. It could be argued that as both muscle activity and trunk sway are correlated that use of muscle activity as a feedback parameter is not necessary. The global measure that trunk sway changes represent may be sufficient to determine that an improvement had taken place. However these global measures would not indicate where changes had taken place and which muscle responses could be improved further, as, for example, the tibialis anterior and soleus muscle activity in this study. These issues could be raised for vestibular implants in two ways. Would it be more effective if the feedback signal to the vestibular nerve was based on the angular sway of the pelvis rather than the angular velocity of the head? Secondly, should the measure investigated for better balance control be muscular activity at the trunk and legs rather than eye movements?
The reduction in both movement amplitudes and EMG activity with feedback also raises the question: Is the reduction in sway brought about, by a decrease in muscle modulation or background activity? The changes we observed were similar to the response adaptation occurring with tilt responses to stance: a generalised reduction the amplitudes of the large first trial muscle responses to tilt of the support surface occurs when the stimulus is repeated, leading to smaller body displacements [34]. Probably a modelling technique would be required to show that predominantly the reduced modulation of trunk muscle activity with feedback causes reduced movements. In the absence of such modelling, our assumption that the two are associated is the most parsimonious explanation of our results. Further, we assume that the reduced arm muscle activity we observed was a reaction to increased trunk stability.
Reductions in low and high frequency sway
The reductions in sway we observed were mostly in sway angles, but also in sway angular velocity during the task of standing eyes closed on foam. Thus it would appear that both low and high frequency sway is reduced [23]. This raises the question about the best way to code sway information in a balance prosthesis in order to produce the most effective feedback. Goodworth et al. [18] indicated that vibro-tactile feedback provides only low frequency (<0.6 Hz) angular feedback information on sway. They argued that this result occurred because feedback parameters were not fitted individually, rather a group “one-fits-all” approach was used [29]. Our thresholds were determined individually. It is also possible that mainly position information is extracted by subjects from our vibro-tactile feedback signals and velocity information enhanced in higher frequency sway was obtained by the acoustic feedback which increased in volume when sway was larger. The system of Goodworth et al. [18] used a combination of pelvis angle and angular velocity [24, 43]. They investigated which combinations of position and velocity feedback improved low frequency (<0.6 Hz) sway [19]. (No improvement for high frequency sway was noted with their system of vibration at the waist) Thus it remains to be investigated which combinations a vibro-tactile can be used by patients and controls to improve high frequency sway and presumably reduce sway velocity. Assuming that in our study, patients used the acoustic information for correcting high frequency sway (>0.6 Hz), no difficulties were apparent when patients combined vibro-tactile and auditory feedback into motor commands.
Balance feedback for other patient groups
This study may have implications for other patient groups when they receive biofeedback to reduce abnormal body sway. Here we have emphasized that vestibular loss subjects use the same movement strategies with feedback as healthy controls without feedback when BVL patients received pelvis angular position feedback. We assume that the feedback substituted for the vestibular inputs that normally act to provide appropriate modulation of balance correcting strategies. Another patient group we investigated, those with Parkinson’s disease, also showed improvements in sway with velocity rather than position feedback [33]. An MS patient group also showed greater improvements in gait when velocity feedback was used, and improvements in stance with position feedback [42]. Whether the balance correcting strategies of these patients are similar to those of vestibular loss patients is not known. Lower-leg proprioceptive loss subjects use different balance correcting strategies to those of healthy controls [26]. For different patient groups, it is an open question whether these patients need to change their balance correcting strategies to those of healthy controls before they can be aided by the feedback schemes of this and other studies [16, 43] or whether the mix of angle and angular velocity feedback needs to be changed appropriately to fit the patients’ different balance correcting strategies.
Conclusions
This study demonstrated how vestibular loss subjects achieve a reduction of sway during stance with prosthetic feedback of body sway. Unchanged movement strategies but reduced movement amplitudes were achieved with reduced background and amplitude modulation of EMG activity at the lower legs and trunk. Thus we propose that body angular displacements and angular velocity as well as muscle measures should be explored as feedback variables for future prosthetic devices, including implants, which aim to reduce sway of those with a tendency to fall.
Competing interests
The authors report that J.H.J. Allum and F. Honegger worked as consultants for the company producing SwayStar™ and BalanceFreedom™, equipment used in this study.
Footnotes
Acknowledgments
This work was supported in part by a grant from the Freiwillige Akademische Gesellschaft Basel.