
Abstract
Introduction
Determining whether an individual has suffered a concussion often requires the employment of many clinical assessments including cognitive, psychological, motor, balance and gait tests, as well as symptom reports [16, 39]. Although concussions, also referred to as mild traumatic brain injury (mTBI), are commonly reported to resolve within 7–10 days, there are currently no “gold-standard” objective measures for diagnosing concussion, rather it is identified by functional deficits and clinical judgment [39]. The accuracy of the clinical diagnosis is largely dependent on the sensitivity and specificity of the tests used to detect signs and symptoms (s/s), rather than being able to detect and identify structural deficits. In the acute stage of concussion (<7 days), many of the clinical assessments have been shown to be highly sensitive to symptom detection [23, 41]. Beyond a few days post-injury, sensitivity tapers off significantly, which may lead to a premature diagnosis of “good health”. Among the objective measures that are emerging, such as methods for detecting diffuse axonal damage from the primary injury [30] or cellular damage from the secondary injuries [22], they have not yet reached a high level of diagnostic precision. Therefore an effective approach for patient management continues to depend on symptomatology and the need for better assessments of signs. Both of these can be aided by gaining further insight into the pathomechanisms underlying mTBI.
The search for reliable and valid s/s of concussion has lead to a growing body of evidence that individuals with long-lasting, unremitting impairments often report vestibular symptoms, such as dizziness, and postural and gait disturbance [1, 29]. In fact, dizziness is reported in over 50% of concussions and is associated with a greater than a six-fold increased risk for prolonged recovery [35]. Other related symptoms include sensitivity to visual motion, which can also persist beyond the acute period [9, 57]. Furthermore, there is a well-established body of research that shows oculomotor function can be impaired [14, 48], which affects not only visual control, but postural stability as well.
Postural assessment is recommended as a component of post-concussion examination in the Zurich Consensus Statement [39]. Common tests include the Balance Error Scoring System (BESS) or Neurocom’s Sensory Organization Test (SOT, Natus Medical, Inc. [42]), both of which have been shown to be sensitive to postural deficits during the first few days after injury [6, 45]. While the BESS and SOT tend to be most sensitive in the very acute stage of recovery [23, 38], many studies now suggest there are postural and motor signs and symptoms that do not resolve within a week or two [5, 29]. New balance measures using virtual reality (VR) technology similar to those used on clinical populations with visual-vestibular processing issues [33] are proving to be sensitive at detecting concussion even beyond the acute stage [44, 58]. VR technology has also been found to be beneficial for use in treatment of post-concussive dizziness and postural dysfunction [44]. The link between visual and vestibular motion processing is an integral part of spatial orientation perception and balance control [53, 54], which can be manipulated by using VR techniques. Dynamic VR inherently includes a visual-vestibular conflict in that visual motion is not accompanied by inertial forces [53, 55], which can affect normal perception of verticality and postural stabilization processes even in healthy individuals [32, 54]. The effectiveness of VR exposure-therapy and the sensitivity of VR at detecting signs of postural deficits suggests that individuals with concussion have even greater difficulty integrating and weighting visual and vestibular inputs than healthy individuals.
In addition to postural assessment, vestibular and oculomotor assessments are proving sensitive in concussion detection [27, 41]. Together these two systems are important for sensing angular and linear acceleration of the head and eyes, which enables a moving individual to maintain gaze on a stable target or a stationary individual to focus on a moving target. For example, during walking the impact of each footstep shakes the head, yet multiple vestibular reflexes stabilize the head and eyes allowing one to read a text message on their smart phone while on the go. Assessing peripheral vestibular, visual, and oculomotor function together with balance and gait is a necessary approach to understanding how these processes influence one another, especially when one or more is impaired. Their covariance likely plays a role in why they have all been found to be sensitive to brain injury.
Despite the growing number of studies that are being done to examine the multifactorial combination of sequelae following concussion [3, 41], there is no consensus criterion-measure for assessing whether an individual’s symptoms have fully resolved. Combining visual and oculomotor assessments with others that examine whole-body behavioral output of vestibular, visual, and somatosensory integration (e.g., postural balance) may provide comprehensive information and greatly improve concussion management. The purpose of this study was to evaluate the role of visual and vestibular processing deficits following concussion in the post-acute stages of recovery. We focus on post-acute because vestibular deficits have been previously identified in those who do not recover quickly from their injury [1, 5]. This study compares a number of common vestibular, oculomotor, and balance assessments as well as a novel balance assessment device that uses virtual reality visual stimulation to challenge visual-vestibular processing in persons with and without concussion. We present evidence showing that assessments relying heavily on visual and vestibular integration are most helpful in identifying deficits following concussion.
Methods
Subjects
All individuals with concussion (n = 14) were evaluated by a certified athletic trainer or physical therapist during the initial evaluation. Participants were all students recruited on a college campus. In this study, concussion was defined as sustaining an impact or high acceleration event that induced one or more concussion signs or symptoms [39]. All individuals with concussion reported that they had experienced a head impact and were included if they reported having an event within six months (time-since-injury mean = 36 days; range 10–120 days; n = 14) in addition to having one or more symptoms at the time of injury (e.g. headache, dizziness, nausea, balance problems, difficulty concentrating, drowsiness, irritability. See Zurich Consensus Statement for complete list of symptoms [39]). At the time of enrollment no concussed participants were receiving treatment or therapy, and resolution of symptoms was not an exclusion criterion. Six participants reported symptoms before testing, five of which were headache and four were dizziness compared to no reports of symptoms in the healthy cohort before testing. The healthy individuals (n = 58) were included if they reported no concussion within the last six months; only three healthy participants had any history of concussion (Lifetime concussions mean: Concussion cohort = 3.5; Healthy cohort = 0.14, p = 0.001). The ages (21.7±3.5 y.o.) and gender distribution (43% female) did not differ between groups. All subjects signed a Temple University IRB-approved consent form in accordance with the guidelines of the Helsinki Accords. All subjects received monetary compensation for participation in the study.
Protocol
All participants performed a series of balance, vestibular, and oculomotor assessments, which have been previously described in greater detail [40, 57]. Participant symptoms were collected before and after the vestibular and oculomotor assessments noted below. Although in each of these tests the experimenter also assessed the saccades and head movements for quickness, smoothness, and/or accurate fixation of the target, only the verbal rating scales symptoms are reported here. Our previous study has shown that clinical assessments of behavioral signs were less sensitive than symptom reports following concussion [40]. The verbal rating scales consists of three 7-point scales, which are subjective reports of dizziness, headache, and nausea (“No symptoms” = 0, the highest level of symptoms = 6). The within-subject change from baseline level was used for outcome measure analysis. Before and after the test, the participant was asked the level of each symptom separately. The cutoff score for a positive test occurs when the participant reports an increase of two or more on the verbal rating scales [41].
Balance assessments
Virtual reality (VR)-based balance device – this new portable postural assessment device uses custom-designed software and commercially available technology [i.e. Wii Balance Board, 60” (75 cm high×134 cm wide) television, Bluetooth USB, desktop computer]. It has previously been shown to be reliable and valid for postural assessment [57, 58]. Our visual stimulus uses a high-resolution digital snapshot taken of an immersive VR scene, which depicts a three dimensional environment of an outdoor temple with Greek columns, marble flooring, Persian rugs and a mountain range in the distance (VRCO, Virginia Beach, Virginia, USA [32]). The VR scene is passively rotated about the subject’s roll axis at 60°/s in the dynamic visual conditions, which was chosen because visual motion about the roll axis has been shown to be posturally destabilizing, especially at velocities >25°/s [17, 43]. Moreover, concussed and sub-concussed populations have been found to be more sensitive to visual roll tilt than other axes of visual tilt [25, 47]. Center-of-pressure (COP) time series data is collected at 100 Hz, and from that COP sway area, sway velocity, and standard deviation in anterior-posterior (AP) and the mediolateral (ML) direction are derived. Six balance conditions are collected in the dark with barefoot participants standing 40 cm from the television screen in a completely dark room (Field-of-view of the television screen at this distance is 62°×73°). Participants placed their feet a comfortable distance apart with an allowable heel-to-heel range of 20–25 cm. The six conditions are (1) EO-Firm: Eyes open while standing on a firm and stable support surface while viewing a static visual scene, (2) EC-Firm: Eyes closed while standing on a firm and stable support surface and dark screen, (3) DYN-Firm: Eyes open while standing on a firm and stable support surface while viewing a dynamically rotating scene, (4) EO-Foam: Eyes open while standing on a unstable support (Airex foam pad placed on top of the Wii Balance Board) and stable visual scene, (5) EC-Foam: Eyes closed on foam support, and (6) DYN-Foam: Eyes open while standing on an unstable foam support while viewing a dynamically rotating scene. These six conditions were collected in the above order three times each, making 18 trials in total, in a manner that was designed to emulate the SOT protocol.
Balance Error Scoring System (BESS) – this test provides a measure of postural stability by subjectively counting errors during a series of six balancing stances [23]. All postural conditions are tested in bare feet with eyes closed. The six conditions, always tested in the same order, are three stances (double-leg, single-leg, and tandem) on a firm surface followed by the same three stances in the same order executed on the foam pad (Alcan Airex, Sins, Switzerland). A trained rater counted the number of performance errors. The total numbers of errors were summed to determine the participant’s score, with a higher score demonstrating poorer performance.
Oculomotor tests
Rapid Horizontal Eye Saccades – this test measures the participant’s ability to quickly saccade left and right between targets. A seated participant is instructed to quickly look back and forth from one target to the next using only eye movements (without moving the head) synchronized with the sound of a metronome (Metronome, ONYX iPad App) beeping at 120 beats for 1 minute (1 Hz = full cycle back and forth). The participant was asked to report symptoms before and after this test.
Fast Smooth Pursuit – smooth pursuit tasks were used to test the participant’s ability to follow a fast moving target with their eyes. The seated participant was instructed to focus on the tip of a pen held at eye level by the experimenter while it was moved horizontally 0.5 m to the left and right (∼30° in each direction) to the beat of a metronome (100 beats per minute) for 30 sec. The participant was instructed to follow the target with their eyes only. Abnormal eye movements were recorded if the participant was unable to keep focusing on the pen tip or the experimenter noted excessive saccades in directions misaligned with the stimulus.
Optokinetic stimulation (OKS) – a normal reflexive optokinetic nystagmus (OKN) response is elicited when viewing a moving striped visual stimulus with whole or part of the visual field [15, 49]. This test was performed using an optokinetic drum iPad app, which displays a high contrast grating passing horizontally across the visual field (OKN Stripes, downloadable app; Settings: red and white drum, 0.5 cm line width, 8.6 cm/sec). Participants were instructed to hold the iPad 15–20 cm from the eyes, which covers approximately a 60° diagonal field-of-view. The participant was asked to report symptoms before and after this test.
Near Point Convergence (NPC) – this test measures the ability to adduct and accommodate the eyes to view a target without double vision as it approaches one’s nose. The near point convergence test was measured using the standardized push-up method [40].
King-Devick Test – this test evaluates oculomotor, attentional, and language processing involving a series of single-digit numbers that are read out loud as quickly and error-free as possible. The test has been shown to be sensitive to detecting brain injury symptoms [21]. The cumulative time taken for reading the three cards twice through is recorded as the total King-Devick time. Error-rate did not differ between groups, so is not included in further analyses.
Vestibular tests
Dynamic Visual Acuity Test – this test compares visual acuity when the head is static compared to when the head is moving to assess VOR function [36]. All participants stood 2.0 m from tumbling E visual chart and were instructed to read the orientation of the E (i.e., left, right, up, or down) while keeping their head stationary until they reached a line they could not read without errors in its entirety. This was then repeated while the participant actively moved their head 30° to left and right in the horizontal plane to the beat of the metronome (180 beats per min). The dependent variable is the line difference between the lowest line read with head static and head dynamic.
Horizontal Gaze Stabilization Test (GST) – the gaze stabilization test assesses vestibular ocular reflex (VOR) by testing an individual’s ability to stabilize vision on a visual target as the head is actively nodded repetitively in the left-right direction. All participants stood fixating a single visual target (i.e. an “X” on a piece of paper with Arial, bold, 48 font) at eye level, arm’s length away. Participants were instructed to turn their head horizontally approximately 30° to the left and right to the beat of the metronome (240 beat per min) for 1 min while fixating the target, and reporting if the target became blurry or bounced around (i.e. oscillopsia). The participant was asked to report symptoms before and after this test.
Head Thrust (VOR test) – this test evaluates VOR by assessing the ability to stabilize vision as the head moves. The participant was seated and asked to relax his/her head and neck as the experimenter moved the participant’s head quickly to the left or right while fixating the experimenter’s nose. The head thrust was performed in the horizontal plane randomly to the right and left three to four times ±30°. Abnormal VOR was recorded if the participant was unable to keep focused on the examiner’s nose or the experimenter noted excessive saccades in directions misaligned with the stimulus.
Statistical methods
A 2 (group)×2 (surface)×3 (visual condition) repeated-measures ANOVA was used to analyze any significant main or interaction effects. Due to large differences in group samples, violations of sphericity were checked by Mauchly’s test, and in cases where a large violation of sphericity occurred a MANOVA was used [20]. Between-group proportional differences in reporting a history of previous concussion was calculated with a chi-square test. Pearson’s correlations between balance, vestibular, oculomotor assessments, and symptom reports were examined to determine which variables were correlated. Student’s t-test for independent groups was used to analyze s/s with adjustments to degrees of freedom when Levene’s test for equality of variances was significant. A logistic regression for binary outcomes (“Enter Method” and “Forward Conditional”) was performed to examine predictive validity of the balance, vestibular, and oculomotor assessments. From the logistic regression classification table, “accuracy” was calculated as the sum of the true positives and true negatives divided by the total sample size. Logistic regression provided weighted coefficients (beta weights) for defining a regression model. The regression model was tested using receiver operating characteristic (ROC) curves. Then, area under the curve (AUC) for these ROC curves was calculated and a cutoff score was determined by choosing the value that maximized sensitivity and specificity. All statistical analyses were conducted using SPSS software (version 22.0; IBM Corporation, Armonk, NY) and significance was set at alpha equal to 0.05. Bonferroni correction was used to adjust p-values for multiple comparisons where applicable.
Results
Between-group comparisons (Table 1)
Balance data collected using the novel VR-based balance device showed a main effect of health status (F1,69 = 12.5, p = 0.001) with the concussed group showing greater COP sway area than the healthy group in all balance conditions. COP standard deviation in the mediolateral (F1,69 = 3.54, p = 0.007) and anterior-posterior (F1,69 = 3.71, p = 0.005) directions also showed a between group difference. COP sway velocity was not sensitive to health status (p = 0.061).
Means and standard deviations of concussion assessment scores
Means and standard deviations of concussion assessment scores
Note. M (mean), SE (standard error of the mean), n (number). BESS (balance error scoring system), NPC (near point convergence), HES (horizontal eye saccades), OKS (optokinetic stimulation), GST (gaze stabilization test), DVA (dynamic visual acuity), KD (King-Devick), SP (smooth pursuit), *Significance set at p < 0.05.
Significant differences were found for all symptoms scores collected following oculomotor and vestibular tests: rapid alternating horizontal eye saccades (t(70) = –2.35, p = 0.035, Student’s t-test for independent samples), optokinetic stimulation (t(70) = –2.65, p = 0.02), and the horizontal gaze stabilization test (t(70) = –2.47, p = 0.028). The near point convergence sign also showed a significant between-group difference (t(70) = –2.99, p = 0.010). No abnormalities in the VOR head thrust test were observed in either group.
Balance data collected from the BESS test showed no between-group differences for the total score (t(70) = 1.27, p = 0.21), nor did King-Devick total time (t(70) = –1.30, p = 0.22), but the dynamic visual acuity test score did (t(70) = –2.24, p = 0.029).
Health group (healthy or concussed category) correlated significantly with all six balance conditions. The highest r-values were with the two dynamic visual conditions (DYN-Firm: r = 0.33, p = 0.005; DYN-Foam: r = 0.42, p < 0.001). All s/s scores following the vestibular and oculomotor tests including the rapid alternating horizontal eye saccades (r = 0.46, p < 0.001), optokinetic stimulation (r = 0.50, p < 0.001), and the horizontal gaze stabilization test (r = 0.45, p < 0.001) were significantly correlated with categorical health status. The near-point convergence distance was also significantly correlated with health status (r = 0.42, p < 0.001). However, the King-Devick total time (r = 0.18, p = 0.13, n.s.), dynamic visual acuity test (r = 0.13, p = 0.27, n.s.), and total BESS score (r = –0.15, p = 0.21, n.s.) were not. There was no variability in the VOR head thrust or the smooth pursuit since all participants, healthy and concussed, were assessed to have normal response.
Correlation coefficients among all assessments and categorical health status
Correlation coefficients among all assessments and categorical health status
Note. BESS (balance error scoring system), DVA (dynamic visual acuity), GST (gaze stabilization test), KD (King-Devick), HES (rapid horizontal eye saccades), NPC (near point convergence), OKS (optokinetic stimulation), r (Pearson product-moment correlation coefficient), *p < 0.05, **p < 0.01.
Performance on the VR-balance test correlated most significantly with the symptoms scores following the gaze stabilization test (r max = 0.55, p < 0.001), the optokinetic stimulation (r max = 0.40, p < 0.001) and the horizontal eye saccades (r max = 0.41, p < 0.001), but did not significantly correlate with any of the objective measures of vestibular or oculomotor function, including near-point convergence distance (r max = –0.14, p = 0.24, n.s.), King-Devick total time (r max = 0.17, p = 0.16, n.s.), dynamic visual acuity test (r max = 0.12, p = 0.34, n.s.), and total BESS score (r max = 0.15, p = 0.22, n.s.).
For the VR-based balance conditions, COP sway area was analyzed using binary logistic regression because it had the highest between-group effects sizes relative to the other COP metrics. These regressions revealed that the dynamic scene conditions, i.e. DYN-Foam (p = 0.002) and DYN-Firm (p = 0.003), were the most discriminating conditions with and 85.9% and 87.3% accuracy, respectively. From the oculomotor and vestibular tests, it was found that provoked symptoms following optokinetic stimulation (p = 0.001) and the convergence test (p = 0.004) were most accurate at 93.1% while none of the other outcome measures were retained as significant in a forward conditional regression model. By combining all outcomes in a single forward conditional regression DYN-foam, optokinetic, horizontal eye saccades, and the convergence test produced the most accurate model with an accuracy of 94.4%. Using this model to calculate a receiver operating characteristic curve (Fig. 1) revealed it to have a highly significant area under the curve (AUC = 0.988, p < 0.001) with a sensitivity of 100% and a specificity of 93.1%.
Concussion assessment model – binary logistic regression results
Concussion assessment model – binary logistic regression results
Notes. CI (confidence interval), DYN-Firm (dynamic visual scene with firm surface), DYN-Foam (dynamic visual scene with foam surface), HES (rapid horizontal eye saccades), NPC (near point convergence), OKS (optokinetic stimulation), SE (standard error), S/S (sign and symptom), VR (virtual reality). *significance at p < 0.05.
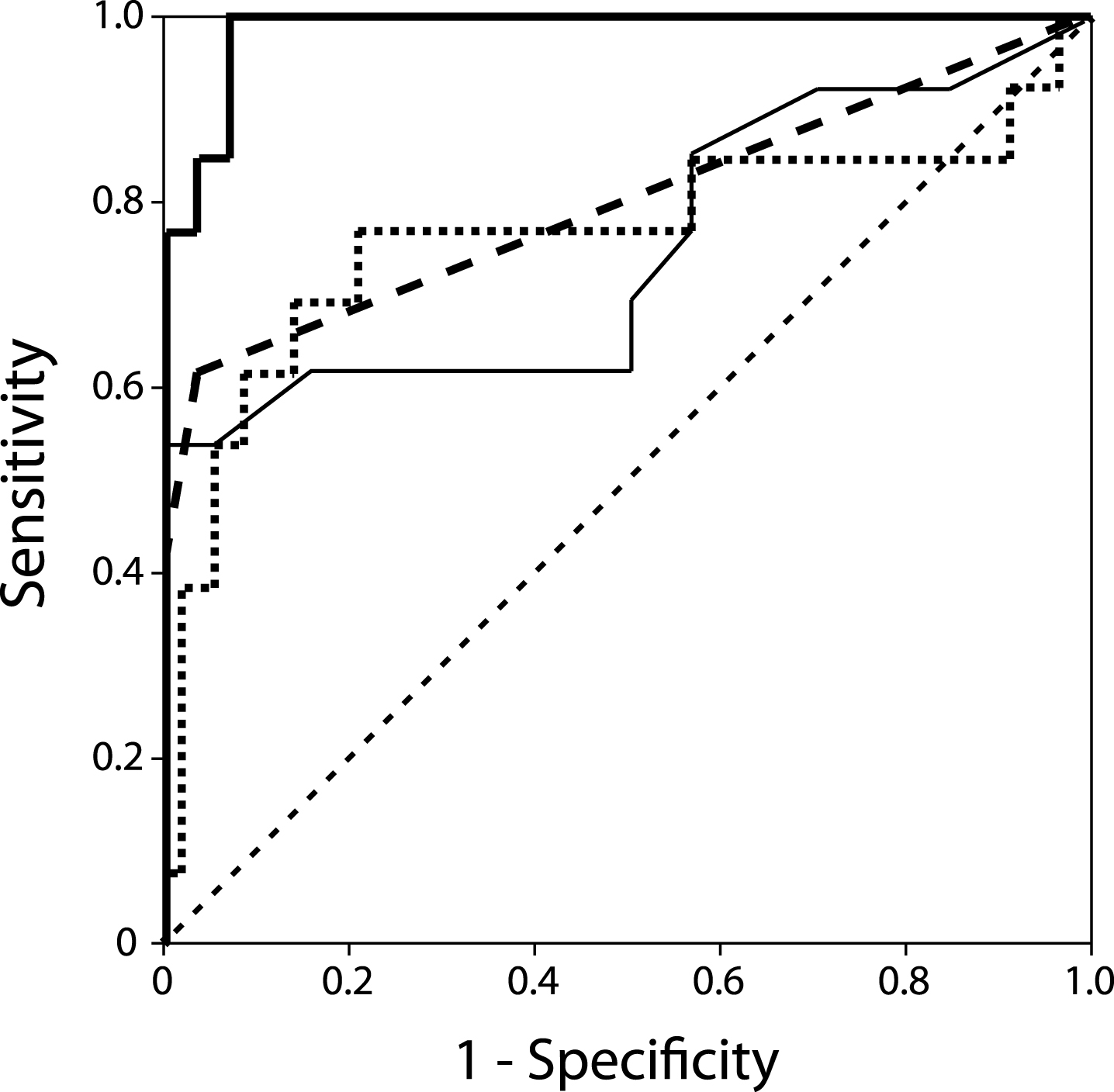
ROC curves generated using a logistic regression model. The full model (thick solid line) includes the COP sway area for DYN-Foam (dotted), OKS (thick dash) and HES symptoms, and the convergence distance (thin solid). The area under the curve (0.988) is highly significant with an excellent sensitivity and specificity well above chance (dashed diagonal line).
Discriminating individuals in the concussion cohort from the healthy cohort relied on the outcomes of a combination of vestibular and oculomotor symptom assessments together with postural tasks to achieve the greatest accuracy. Assessment with the portable VR-based balance device alone was able to discriminate between groups, with the concussed group showing greater COP sway area and COP variability than the healthy group. The specific VR condition that was most sensitive to differences involved dynamic visual motion, as has been previously shown with large field-of-view VR in concussion [46, 47], as well as in other clinical populations with visual-vestibular processing deficits [33]. The symptom reports collected after performing the oculomotor and vestibular tests (i.e. rapid alternating horizontal eye saccades, optokinetic stimulation, and the gaze stabilization test) were all sensitive to between-group differences; however, the signs did not show observable abnormalities (i.e. the observable eye movements). The BESS and King-Devick tests were also not sensitive to between-group differences. These findings, discussed below, suggest visual-vestibular processing deficits are present in subacute individuals following mild traumatic brain injury.
Vestibular processing
There are a number of clinical assessments of VOR that are commonly used and three of them were employed in this study (head thrust, dynamic visual acuity test, gaze stabilization test). Despite prior evidence that VOR abnormalities are prevalent following mild head trauma [28, 41], the visual assessment of objective signs such as asymmetrical or excessive eye saccades were not sensitive to between-group differences. Two possible reasons for this (which are also applicable to the oculomotor tests discussed later) are, first, that the protocol for eliciting oculomotor signs was not demanding enough to reveal a deficit, or second, subjectively identifying abnormal saccades or loss of target fixation falls on the clinical rater’s ability to notice minute anomalies in oculomotor behavior that would more easily detected with oculography [27]. Despite the absence of VOR signs, the dynamic visual acuity test and symptoms reported by the participants after the gaze stabilization test were found to be sensitive to brain injury, with individuals in the concussion group reporting more dizziness, headache, and nausea. Indirect measures of vestibular function, such as the balance conditions that heavily rely on vestibular input were not highly sensitivity to between group differences.
The mixed results on vestibular tests may suggest that the consequences of concussion is not a purely vestibular system deficit [1]. Specifically, the BESS test conditions performed on foam with eyes-closed provides unreliable somatosensory feedback and no visual feedback, therefore postural control is dependent on vestibular processing. Similarly, the eyes-closed balance condition while standing on foam (EC-Foam) relies heavily on vestibular contributions to balance. The vestibular system acts via the descending vestibulospinal and reticulospinal tracts to make postural corrections and maintain upright stability. However, neither of the balance conditions eyes-closed postural tests on foam (EC-Foam and BESS foam) were sensitive to group (concussed versus healthy). It should be noted that the BESS has been shown to return to normal within five days post-injury [23, 38], while the majority of our concussion group was more than two weeks post-injury. Considering these findings together suggests the symptoms being experienced in our concussion group cannot be fully described by vestibular deficits alone.
Visual and oculomotor processing
The oculomotor assessments of signs were largely insensitive to health status (i.e. smooth pursuit, King-Devick, rapid horizontal eye saccades, optokinetic test) with the exception of near-point convergence. As suggested above, this may be due to lack of a sensitive oculography, but also the extended time-since-injury of the our cohort may have allowed for compensation or recovery to occur. There was, however, evidence that convergence is negatively affected by mild TBI within our cohort, which supports previous findings [11, 48]. The sensitivity of the convergence test may speak to its ease of use; participants can reliably report when a visual target becomes blurry or doubles and the experimenters can reliably use the tool. Given the discriminant accuracy of the convergence test found in this study, various mesencephalic circuits are implicated. The ‘near-response’ neurons driving the near-reflex triad (i.e. convergence, accommodation, and pupil constriction) involve the oculomotor and parasympathetic Edinger-Westphal nuclei [37]. These oculomotor control centers and the afferent and efferent white matter tracts linked to these centers, such as the tectospinal or cortico-tectal tracts, may be highly susceptible to the biomechanical stress and strain forces following head impact due to their location in the midbrain [48, 50]. The view that diffuse axonal injury has widespread cortical and subcortical effects following mild TBI is generally accepted [7]. Given the presence of oculomotor control deficits, it appears brainstem involvement is very likely, while the presence of visual motion processing deficits, discussed below, will provide evidence that the injury is not isolated to the brainstem.
Although the signs observed in the oculomotor tests were not sensitive to between group difference, the reported symptoms following some of the oculomotor tests were (i.e. rapid horizontal eye saccades, optokinetic stimulation). This symptom sensitivity supports previous reports of symptom elicitation after observing excessive optic flow [31]. Individuals who have recently experienced a concussion or those suffering from unremitting post-concussive symptoms often report sensitivity to light and visual motion such as when watching television or playing video games. The oculomotor response during horizontal eye saccades and optokinetic stimulation requires the suppression or activation of the optokinetic reflex, respectively. The neural centers and circuitry associated with optokinetic nystagmus include many midbrain structures, such as the oculomotor and accessory optic nuclei and the nearby optic tract nuclei [10]. These centers have connectivity to the vestibulocerebellum and the visual (parietal-occipital) association cortices. Thus, although the signs were not detected, visual processing associated with the optokinetic stimulation is impaired in a manner that reliably elicits symptoms in those with concussion. This evidence points to a possible combination of cortical and subcortical regions involved in both visual and vestibular processing.
Visual-vestibular processing
Processing of visual motion is integral to self-motion perception and an individual’s ability to discern self versus environment motion involves multisensory comparison between vestibular, somatosensory, and visual inputs [53, 56]. The interplay between the neural regions involved in visual and vestibular processing has been shown in behavioral and imaging studies. Regions such as the parieto-occipital and parietal insular vestibular cortex are thought to be reciprocally innervated [8, 52] and together with bidirectional, decussating connectivity to the vestibular nuclei play an important role in postural control, self-orientation, self-motion perception [18, 34]. The oculomotor and vestibular test findings here suggest that the descending visual-vestibular centers at the brainstem level could be affected by damage, however cortical level damage cannot be ruled out when the multisensory deficits seen in the postural tests are considered.
Postural conditions tested with the VR-device provide compelling evidence that post-concussive symptoms involve visual-vestibular integration difficulties. The balance conditions most sensitive to health status were the two dynamic visual roll conditions (DYN-Foam and DYN-Firm). These conditions were designed to be destabilizing by creating a visual-vestibular conflict between subjective visual and gravitational verticals [17, 54]. This destabilizing visual-roll effect is even greater for individuals who have experienced a head impact [47], even if mild [25]. Other evidence that visual-vestibular processing is disrupted following concussion comes from a case study involving a patient suffering from severe visual and physical motion intolerance and static balance difficulties a month after the incident [44]. The patient was treated with optokinetic stimulation/habituation, visual/physical perturbations, and postural stability exercises in a large field virtual environment, which resulted in almost complete symptom resolution after six treatments [44]. The current and previous evidence indicates that difficulties in visual-vestibular integration may persist well after the typically suggested resolution period of 7–10 days.
Conclusions
Our findings suggest that visual-vestibular processing deficits are present subacutely following mild traumatic brain injury. The combination of specific postural tasks designed to assess the well-calibrated integration of visual and vestibular inputs together with specific visuomotor tests that assess spatial and self-motion perception were found to be the most sensitive tests for discriminating health status following concussion. The comprehensive evaluation of the signs and symptoms allows us to infer which neural processes may be damaged by the injury. It should be noted that assessments largely based on patient reports of symptom provocation rely on the accuracy and integrity of subjective report. Therefore, ensuring subjective measures are supplemented by objective measures such as the VR-based postural assessment described here, ensures higher fidelity in concussion assessment. Other limitations in generalizability of the current findings relate to moderating variables that may affect concussion symptomology. These include cognitive, psychogenic, emotional, cellular, and other neurophysiological processes [4, 51]. The symptoms often reported following concussion are not unique to concussion. For example, exertional heat illness and sickling [2, 19] or whiplash [13] may show overlapping symptoms. These must be considered in any comprehensive multifactorial clinical evaluation of concussion to rule out other etiologies. However, our findings may serve to focus attention in on using sensitive tools for assessing symptoms, especially chronic unremitting signs and symptoms, which can help clinical decision-making and guide treatment during the recovery process.
Footnotes
Acknowledgments
This study was funded, in part, by the Department of Defense, Army Rapid Innovation Fund Award No. W81XWH-13-C-0189 (WGW).