
Abstract
Highlights
Hypothesis: balance deficits alter mental body transformation capabilities. Subjects copied video movements, mirror-imaged, then exactly (lean left as instructor) Patients with balance deficits had lengthened onset latencies and slowed movements for both tasks. Task measures of those with only dizziness were similar to those of healthy controls. Processing of neuropsychological body representation slows when balance control is deficient.
Introduction
Cognitive abilities are receiving more attention in association with vestibular loss, because of an influence of vestibular loss on spatial navigation and internal reference frames for movements (see review Borel et al. [8]). Impairments to balance also occur during cognitive activities [12, 37], suggesting that poor balance control is often associated with cognitive disabilities, and, in addition, a higher cognitive load will yield impaired balance control.
To maintain stable balance during movements, the brain must constantly “monitor” the position and velocity of body movements as the primary cognitive task in order to avoid falling. A secondary cognitive task is to plan the position of the body for the next movement. Both cognitive tasks require an integrated neural representation or “map” of the body (body schema) and its surroundings [16, 28]. The body schema is a neuropsychological representation of the human body constructed from proprioceptive, visual, and vestibular sensory inputs [14]. During normal daily movements, many changes in body position and the surrounding environment occur. Thus, the body has to “map” the environment, build up an internal representation of where the body is and how it is oriented in the environment and use the resulting representation to move without falling. Consequently, there is a continuous process of updating the internal body representation on the basis of information received from sensory inputs [8, 36].
The internal representation could be deficient if the quality of information received from sensory inputs concerning the body and its surroundings is not optimal [21, 25]. For this reason, patients with balance deficits would be likely to have an altered internal body representation which could also have functional consequences for balance during stance and gait. This altered internal body representation could be a further, indirect, factor underlying balance disorders in vestibular loss patients, apart from the direct weakened influence of vestibular signals on balance correcting responses [4]. Indeed, as early as in the 1930 s, the psychoanalyst Schilder [41] described vestibular loss patients who reported abnormal perceptions of their bodies. Later studies demonstrated the importance of normal vestibular signals for correct integration with other sensory cues when processing the current concept of body representation [4, 27].
It is well know that humans use two movement mechanisms to preserve posture and equilibrium [26]. Firstly, there are planned movements such as those prior to the occurrence of a predictable disturbance or as result of an instruction. These are often termed proactive movements [26, 40]. Secondly, there are movements occurring as direct result of a perturbation, triggered by sensory inputs and called reactive movements or automatic balance corrections [4, 32]. Both movement types can be divided into three main phases: decision, coding and execution. The coding will aim to generate a movement program consistent with an internal neural representation of the action. Thus, the internal representation of the current body location, the ability to imagine it in a movement, and then in a new position, are important components in the balance correcting process.
Normally, the self-identification and the awareness of current body location (including the relative location of body segments), are the same [27, 44] and can be considered an embodied [48] or egocentric [18] process. An embodied process is also involved when a person is asked simply to copy proactively the movements of someone standing in front of and facing them [48]. The movements are generally mirror imaged. That is, the instructed person’s right arm would be abducted when the instructor abducts the left arm. A disembodied [48] or transformed [18] proactive process would, according to this concept, imply a person imagining herself/himself in the body of someone distant from her/his actual body location (or transforming the other person’s body into their own) and then copying that person’s movements exactly. That is the instructed person abducts the left arm when the instructor does so. The disembodied process has been termed “own body transformation” or OBT [6, 48] – the definition used here. As noted above, an alteration of the body’s internal body schema occurs if any of the sensory processes needed to update the embodied and/or disembodied representations is deficient in the instructed person. In this case, the movements would presumably be different from those of healthy controls.
Balance-oriented physical therapy is normally based on the external, visible symptoms of patients, and, for example, the effect of the balance deficit on active (proactive and reactive) movements. What is not examined is how much the patients are affected in their specific cognitive abilities necessary to perform active embodied and disembodied copying movements. Some global cognitive aspects are tested for example the ability to dual-task (walk while repeating learned numbers and maintain balance) during the “stops walking when talking” test [13]. These tests do not, however, indicate which specific aspects of cognitive processing are deficient. Based on the reasoning and evidence cited above, if it could be shown that balance deficit patients are limited in the ability to correctly imagine their own body representation in their or another person’s spatial position, it may be appropriate to include attempts to improve this ability in the rehabilitation process. Improving this ability could constitute a new basis for balance deficit rehabilitation and complement current therapies which concentrate on the external, visible symptoms of patients.
The aim of this study was to examine the ability of patients with chronic balance disorders and dizziness to perform the above defined embodied and disembodied movements. Thirioux et al. [48] developed a motor paradigm to investigate mental body transformation processes while viewing motion of an avatar which the test person was asked to mimic in 3 different ways: spontaneously, mirror imaged, and as if the person was in the body of the avatar. The concept of Thirioux et al. [48] was used in modified form for this study. We hypothesized that patients with objective balance deficits (as determined by stance and gait tests) and chronic dizziness would have problems to transform themselves into the body of others and would therefore either not mimic the avatar’s movements correctly and/or would have delayed copying movements. We also hypothesized that those who had only anxiety about falling (dizziness alone) would have less difficulty copying movements but still have abnormal transformation processing. That is, we expected a gradation of the deficit in body transformation processing of these two groups with respect to healthy controls. We assumed, based on the lack of body transformation required, that spontaneous, embodied, movements would be less affected than disembodied (OBT) movements in both groups when compared to those of healthy controls. Furthermore, that differences observed between embodied spontaneous (SPO) and disembodied (OBT) movements could help quantify the central processing deficit of those with chronic balance disorders. Other potential clinical implications, if our hypotheses were confirmed, could include training OBT movements to help improve mental transformation processes in those with balance deficits.
Methods
Subjects
32 subjects with chronic dizziness were separated in 2 groups, 16 with, and 16 without objectively verified balance deficits (obj-BD) based on pathological results for trunk sway during stance and gait tasks [3]. All patients were tested as part of a therapy course for chronic dizziness offered by the Department of Psychosomatic Medicine at the University Hospital Basel. 10 age and gender matched healthy controls (HCs) were selected post-hoc to match the ages of the patients with obj-BD. The subjects with obj-BD had a mean age of 60.6 years (sd 8.3), those with dizziness only (DO) had a mean age of 44.8 (sd 12.1). The healthy controls had a mean age of 60.2 years (sd 5). The retrospective examination of patient data and the testing of HCs was approved by the local ethical committee (EKNZ Switzerland).
To determine which patients had pathological balance control and to check that healthy controls had normal balance control, subjects were asked to perform a sequence of standard stance and gait balance control tests while trunk sway was measured at lumbar 1–3 with a SwayStar™ system (Balance International Innovations GmbH, Switzerland). The SwayStar™ system consists of two angular velocity sensors (fibre-optic gyroscopes) measuring angular velocity in the roll and pitch planes. The test sequence consisted of several two- and one-legged stance tasks, one semi-stance task and several gait tasks. The tasks were validated by Allum et al. [2] and shown to be effective to distinguish patients with balance disorders from healthy subjects [1]. The results for each subject were combined into a summary trunk sway value, the Balance Control Index – BCI [3]. The BCI values were then compared to already existing age-dependent reference values [20] to determine if an obj-BD was present.
All patients were tested with a battery of vestibulo- and visuo-ocular tests within 3 months of the currently reported tests. Details of the test battery are described in Allum et al. [5]. Nine of the 16 patients in the obj BD group had a unilateral peripheral vestibular deficit according to this test battery which was confirmed with a video head impulse test (vHIT) prior to balance testing. For this purpose a vHIT system (EyeSeeCam) from Interacoustics (Denmark) was used. The video head impulse test (vHIT) measures the relation between eye and head velocity when the head is rapidly turned in order to determine if a unilateral peripheral vestibular loss is present [19, 29]. Two patients in the obj BD group had a whiplash associated balance deficit and 5 patients had phobic postural vertigo. Patients with whiplash associated balance disorders had a pattern of balance deficits as described by Sjöström et al. and Findling et al. [15, 43]. We defined phobic vertigo based on the criteria used by Querner et al. [38] and the observation that balance on easy tasks was worse or equal to that of more difficult tasks – specifically for walking 8 tandem steps on a normal floor compared to walking 8 tandem steps on a foam pad. All patients filled out 2 multi-question questionnaires; the dizziness handicap index questionnaire (DHI – Jacobson and Newman [24]) and the brief Symptom Inventory (BSI – Franke [17]). The patient scores for these questionnaires were not in the normal range and not different between the obj-BD and DO groups (see results). Episodic and persistent dizziness was equally spread between the obj-BD and DO group (see results). All HCs were assumed to be healthy, based on self-reporting, normal BCI scores, and a DHI score of 0.
Test procedure
Based on the work of Thirioux et al. [48] concerning own body cognition, subjects were asked to replicate the movements of a gym instructor shown in a life size video 2 m in front of them. To start each set of 10 movement trials, the gymnast first raised the arms to the abducted 90° position (see Fig. 1). For the first 2 sets of 10 trials each subjects were asked to “Lean (roll) your upper body when the instructor leans!” (we called this spontaneous copying, SPO). The instructor was front facing for the first of the 2 sets of trials, back facing for the second. Each set of trials involved 10 movements with the direction (left or right) of the 10 movement trials randomized. No further specific instructions for the SPO task were given. For the second 2 sets of trials, subjects were asked to “Move as if your body was in the place of the instructor!” (we termed this a disembodied movement concept – own body transformation, OBT). The same gymnast’s movements shown for the SPO task were repeated for the OBT task. Subjects were asked to lean left when the gymnast leant left and vice versa to the right for the OBT task. It should be noted that making a non-mirror movement is intrinsically more difficult and opposite in direction to the spontaneous movement condition when the instructor is front-facing, but easier and in the same direction when the instructor is back-facing. Subjects were informed that moving as if their movements were a mirror image of the gymnast’s body for the OBT task would not be correct. Further, if they moved incorrectly they were instructed again after the 3rd and/or 6th trial, if necessary. We did not ask subjects to move as if their own movements were the mirror image of the instructors movements (self-based body percept, embodied), in yet another set of trials, because, in contrast to the observations of Thirioux et al. [48], the SPO movements were always mirror imaged. As performing the OBT first might have influenced performance in the SPO tasks, we used a fixed and not a counterbalanced presentation order. We did not counterbalance front and back facing trials in order to have a valid comparison with the results of Thiriouxet al. [48].
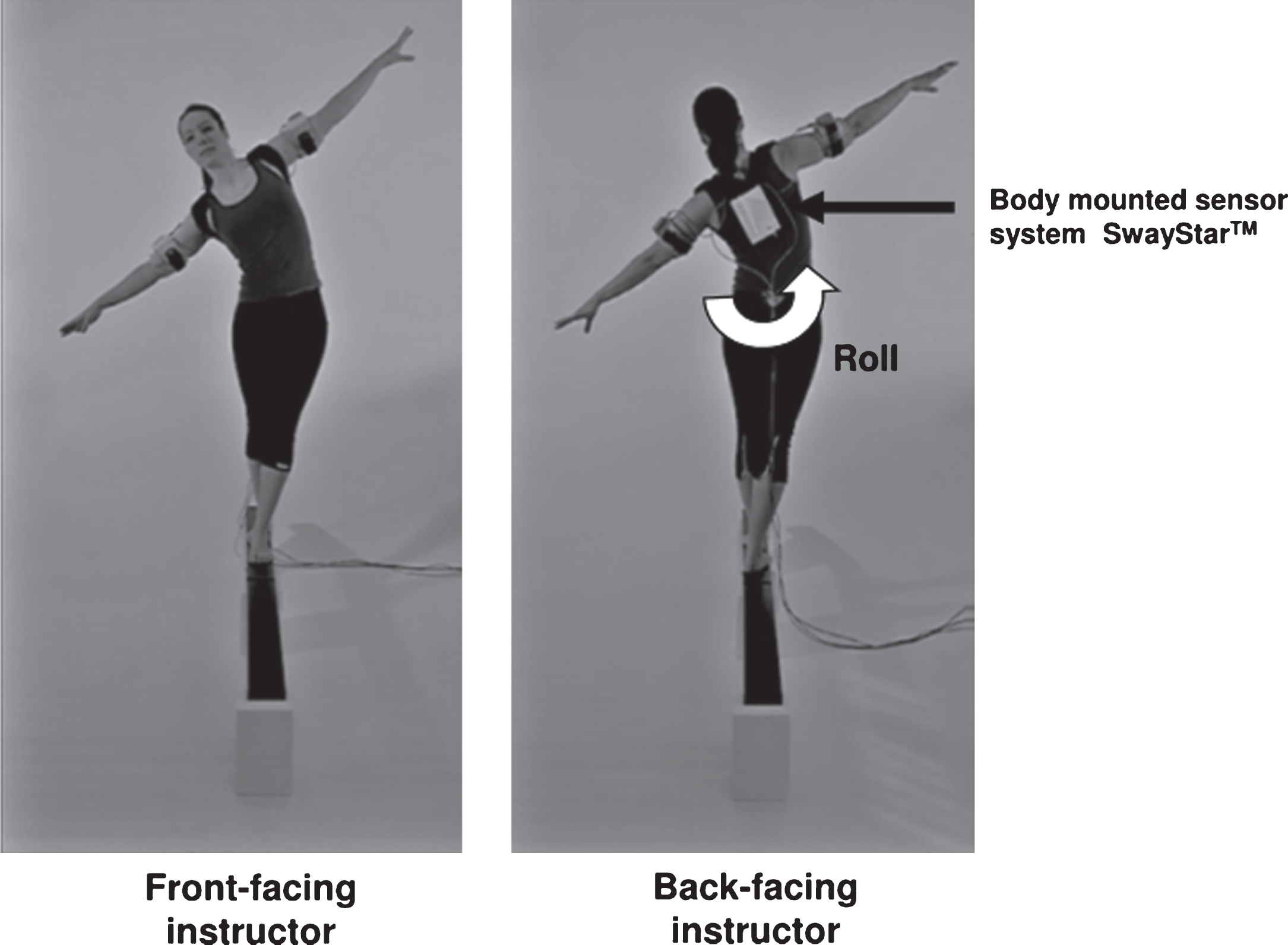
Front and rear facing view of instructor showing roll motion of trunk and adducted arms. The SwayStar™ system is shown mounted between the shoulder blades.
The gymnast in the video stood in tandem stance on a narrow raised beam. This part of the setup was similar to that of Thirioux et al. [48], who used a video of an avatar as a tightrope walker. To make the situation appear more genuine, a white paper surface was put on the floor and a black, thin beam was placed sloping down to the floor as an “extension” of the beam in the video. This was then widened on the floor to two beams side by side on which subjects stood with a foot separation of 10 cm. Tandem stance was not used as patients with balance problems would not stand without falling in tandem stance for the 15 min required to fulfil the SPO and OBTtasks.
The subjects’ roll lean angles and angular velocities of the upper trunk were measured with the same SwayStar™ system used to measure balance control. To measure the upper trunk rather than lower trunk movements this system was placed between the shoulder blades using a shoulder harness. The samples (with a rate of 100 Hz) of angular velocity from this system were sent to a computer via a Bluetooth communication. The velocity signals were numerically integrated on-line to yield angulardisplacement.
The onset of the roll lean angle of the upper trunk for SPO and OBT trials was determined as the time point when trunk roll velocity magnitude first exceeded and remained above 3°/s until the end of the movement. The 3°/s threshold was based on the 95% limit of roll sway velocity for eyes open stance in HCs of age 60 years [20]. The end time of the movement was determined as the time when roll velocity first crossed zero after the movement onset. Movement amplitude was determined as angle difference in degrees between beginning (onset) and end (maximum) angle. The angle was signed as correct or incorrect in direction expected (opposite to the instructor for SPO, same for OBT). The movement onset latency was calculated by comparing the onset of the instructor’s movement with the onset of the subject after correction for the Bluetooth transmission delay (110–125 ms) of the SwayStar™ system. Movement velocity was calculated as the average roll velocity between movement onset and end. The movement interval was calculated as the time between onset of the subjects’ movement and its end with the zero crossing invelocity.
The means of the measurements (latency, interval, amplitude and velocity) for each movement (1 to 10) were calculated for both patient groups and HC subjects. To compare the groups, the mean values of all ten movements were used. For each movement in the OBT trials, only the measures which were in the correct direction were considered. The values of every patient and HCs for the movements 2 and 9 were compared in order to detect if there was a significant difference possibly due to a learning effect. In summary, the main comparisons were SPO vs OBT trials for HCs and for each patient group, between HCs and each patient group for SPO and OBT trials.
To determine if the data were distributed normally, the data was analysed with the Shapiro-Wilk normality test. ANOVAs were then performed followed by post-hoc paired tests for variables with significant group differences which was the case for all measures (F >6.5 3,39 DOF), except interval. As the study included 16 subjects in each patient group, both parametric t-tests and non-parametric tests (Wilcoxon rank sum) were used post-hoc. Only parametric tests are reported here after checking that results were equally significant with both techniques. Comparisons between SPO and OBT variables were analysed with a two-tailed t-test because, in contrast to our results, Thirioux et al. [48] reported longer reaction times for the SPO task. Likewise, for comparisons between groups, two-tailed t-tests were used. Comparisons across trials within a set were analysed with a one-tailed t-test because a learning effect was expected. The significance level for statistical tests was first set at 0.05. Significance was then adjusted (Bonferroni correction) to 0.01 to account for multiple comparisons. This level was applied to all measures.
Results
There was a highly significant difference (p < 0.0001) between the patient groups for the balance control index (BCI) of combined trunk sway scores used to determine the presence of a balance deficit. The mean score of the obj-BD patients was 502.5 (sd 82.3), that of DO patients 390 (sd 33.62). HCs had a mean score of 364.8 (sd 53). We did not test HCs age-matched to the DO patients (46.4 sd 11.2 years). However, Hegeman et al. [20] have shown that there is no difference in BCI scores between HCs of the age of the DO patients (44.8 sd 12.1 years) and the BCI scores of HCs the same age as the HCs used in this study (60.2 sd 5 years).
The “Global Severity Index” score computed across all BSI scores were almost equal (0.78 for obj-BD and 0.79 for DO patients) and greater than normal (0.31 [16]). In particular, the anxiety scores taken from the BSI questionnaires were not different (p = 0.22) between the patient groups being on average 5.4 (sd 4.3) for the obj-BD group and 7.5 (sd 4.6) for the DO group. All patients except 1 were outside the normal range defined by the mean, 0.34, and sd 0.34 [17]. Likewise, the phobic anxiety scores taken from the BSI questionnaires were not different (p = 0.93) between the patient groups being on average 4.9 (sd 3.9) for the obj-BD group and 5.1 (sd 4.1) for the DO group. All patients except 5 were outside the normal range defined by the mean, 0.15, and sd, 0.24 [17]. The types of dizziness experienced by the patients were as follows: in the obj-BD group 37.5% episodic, 62.5% persistent, in the DO group, 50% episodic, 50% persistent. That is, there was no significant difference in the spread of dizziness types between the patient groups. However there were slightly more of the DO group who had a fear of falling (50% versus 17.5%). There was no difference in the mean DHI scores of patients with (52, sd 15) and without (45, sd 13) obj-BD (p = 0.135). The minimum score was 26, the maximum 76. The maximum possible score is 100. All HC had scores of 0.
Differences between SPO and OBT tasks
Both patients and controls performed the front-facing SPO task with mirror image movements to those of the instructor. However, the OBT task was not performed as consistently as HCs. 75% obj-BD patients had one or more complete errors for the OBT task and often had trials with corrections (see Fig. 2). DO patients had better results with only 56% with errors. In contrast, only 10% of HCs had more than one error for the OBT task. The typical picture, as shown in Fig. 2, was for OBT onset latencies to be longer and intervals shorter than those for SPO trials. This pattern was repeated across all subject groups (see Fig. 3 and Table 1). For example, when the OBT roll movements in the correct direction were compared to those of SPO in the obj-BD patient group, onset latencies were longer (by 0.34 s, p < 0.001) and velocities higher (by 4.3°/s, p < 0.001)) for the OBT task. A latency difference between SPO and OBT tasks was present for the DO group (p < 0.001) but this difference of 0.19 (see Table 1) was smaller than that of the obj-BD group. The latency difference between SPO and OBT for the obj-BD patient group was nearly double the difference of the DO and control groups (Table 1). A similar pattern for higher velocities and shorter intervals was noted for the OBT compared to the SPO task in the DO group (Table 1 and Fig. 4). This group also had larger amplitudes for the OBT task. HC subjects also had significant differences in the same direction for latencies (0.16 s), roll amplitudes (5.8°), velocities (6.1°/s) and intervals (0.39 s) between SPO and OBT tasks.
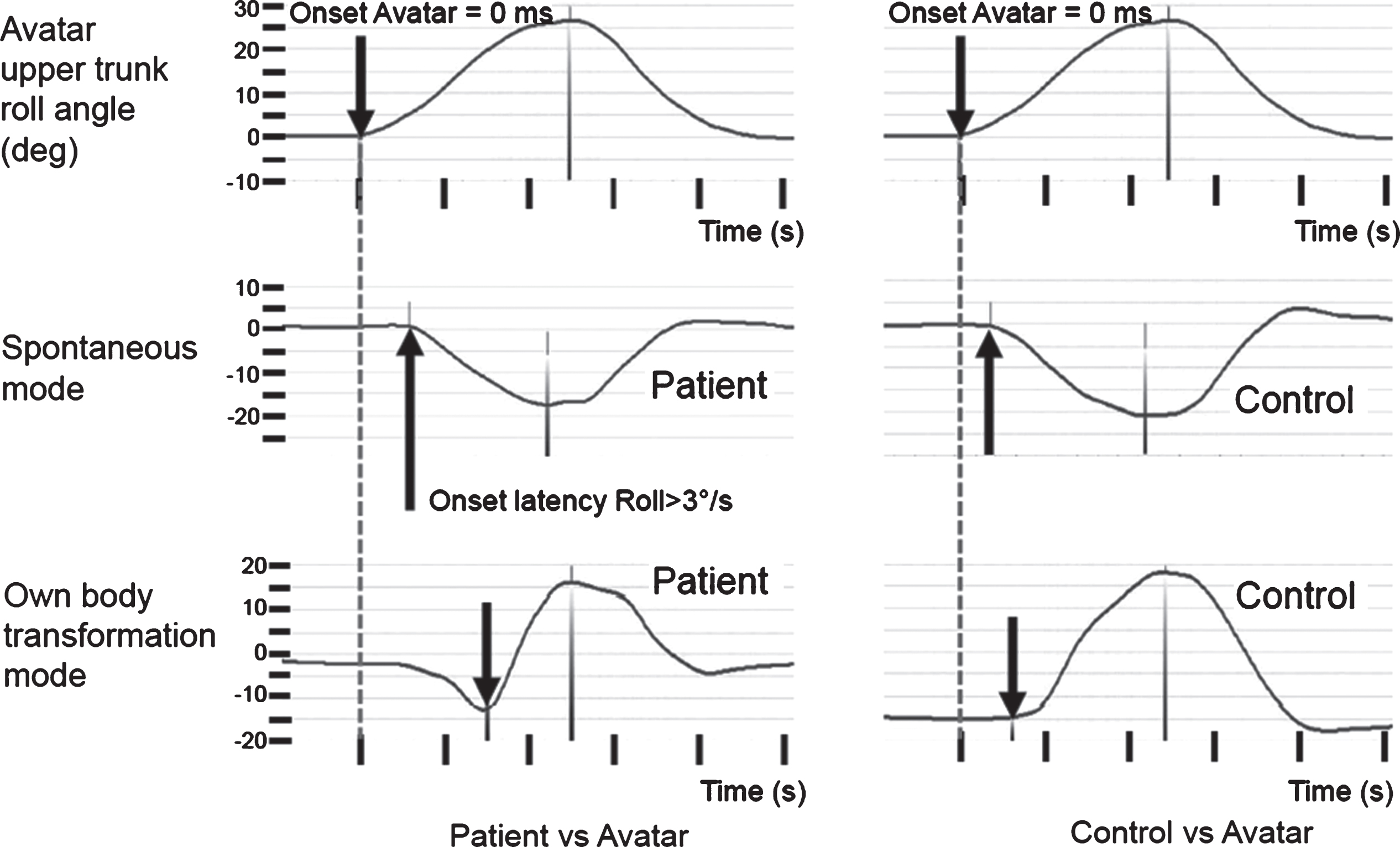
Example traces of upper trunk roll angle motion recorded during the SPO and OBT tasks for a patient with objective balance deficit (obj-BD) (on the left) and an age- and gender-matched control (on the right). The instructor’s traces are shown in the top 2 traces with a vertical downward pointing arrow and dotted line marking the instructor’s movement onset. The middle traces show the mirror image responses for the fifth spontaneous (SPO) trial and the lower set of traces for the fifth own body transformation (OBT) trial. The onsets and end points of the movement are marked. Note how the patient for the OBT trial first moves in the incorrect direction and then, rapidly corrects.
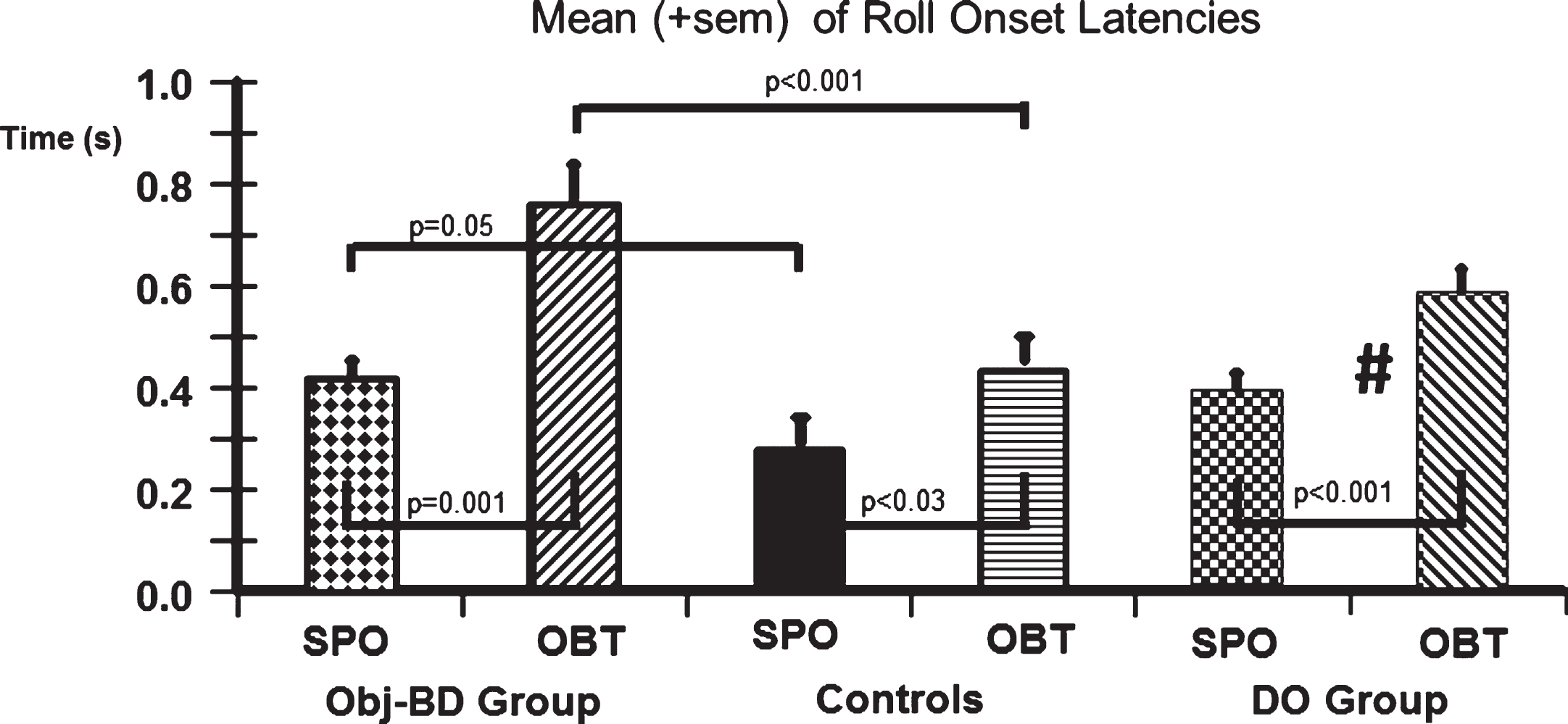
Mean and standard error of mean (sem) of onset latencies for the 2 patient groups with and without obj-BD and healthy controls (HC). The gate symbol (#) on the OBT latency column of DO patients indicates that the mean is different from that of the obj-BD group with a significance of p < 0.01.
List of mean values for all measures in the 2 different patient groups and healthy controls
The difference in mean values is always OBT-SPO. Values of p considered significant for differences are in bold text.
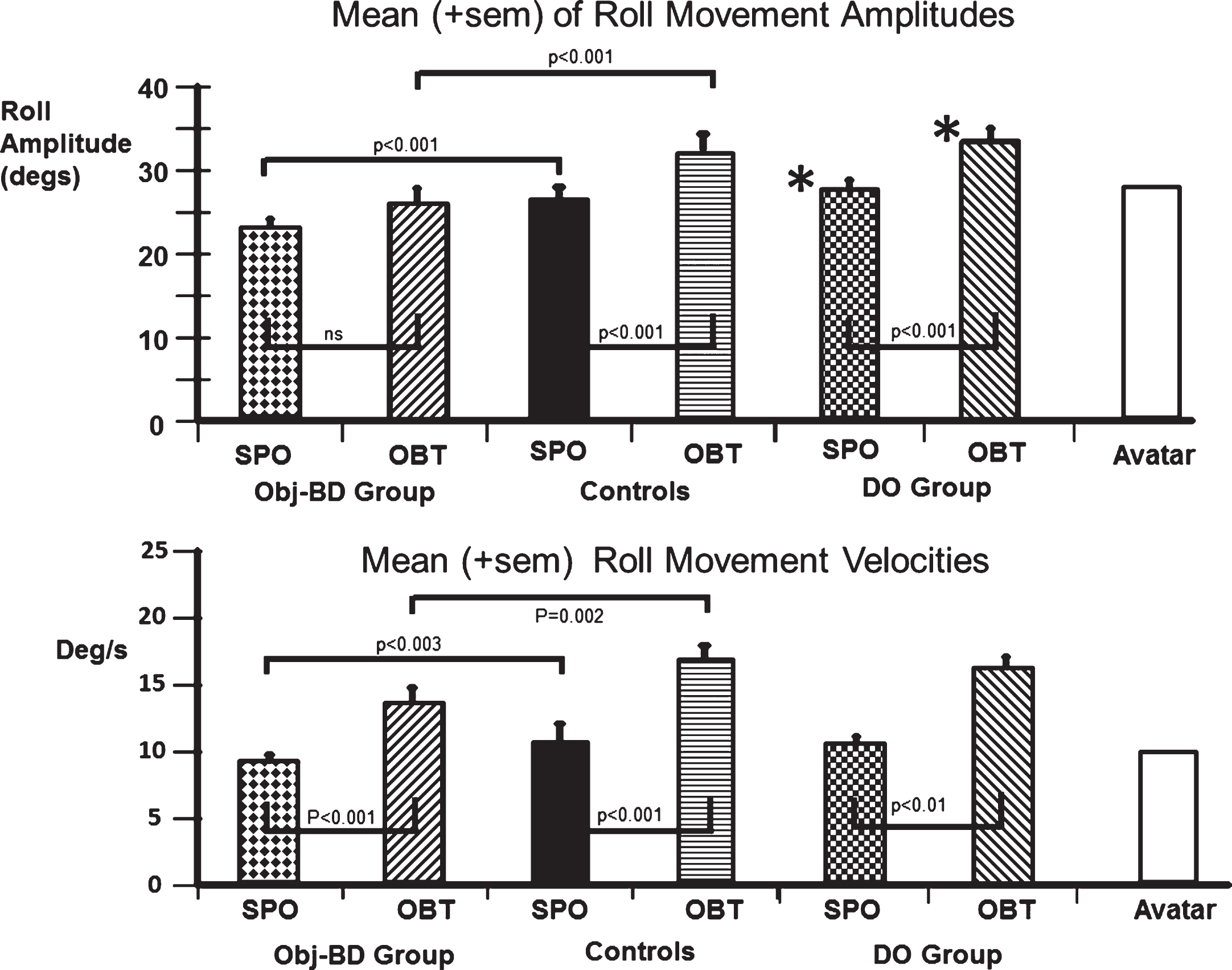
Mean and sem of movement amplitudes and velocities for the 2 patient groups and HC. The mean of the instructor’s values are shown for comparison. The asterisk symbol (*) on the columns of DO patients indicates that the mean is different from the corresponding mean of the obj-BD group with a significance of p < 0.001.
For the SPO task, latencies were significantly longer (p = 0.05) for the obj-BD group compared to HCs but were not different (p = 0.4) when compared to those of the DO group (Fig. 3). Movement intervals (p = 1) showed no significant difference between the groups. However, the amplitudes (p < 0.001) values for the SPO task were significantly lower for the obj-BD group compared to the HC and DO groups (see Fig. 4). For the OBT task, the obj-BD patients had longer onset latencies, smaller amplitudes and velocities than HC and DO patients (p≤0.002, see Figs. 3 and 4). Movement intervals for the OBT task were not different between the 3groups.
Differences between the measurements of the movements 2 and 9 indicated a learning effect in the SPO mode only. Significant reductions over successive movements were found in the SPO mode for latency, velocity and interval values. Controls showed latency reductions between the movements 2 and 9. Intervals were shorter and velocities faster when movements 2 and 9 were compared (p < 0.01). Obj-BD patients showed significant differences (p < 0.01) only for interval values between trials 2 and 9. No significant effects of trial number were found in the OBT mode for any group. We did not find differences between SPO and OBT measures for the back facing instructor.
Discussion
In the study we found that both patients and controls had less difficulty (as measured with movement onset latencies) simply copying movements than when asked to transform themselves into another person’s place and copy that person’s movements. That is, the movements of a front facing instructor were spontaneously copied using a mirror image strategy whereas when asked to copy exactly (lean left when the instructor leaned left and vice versa to the right) the movements started later, occasionally in the incorrect direction, but then accelerated to catch up with the instructor’s movement. This difference between spontaneous (SPO) and explicit changes of own body transformation (OBT) was not present for the back facing instructor, presumably because no front to back body transformation was necessary. Therefore, we concluded that processing a movement which involves rotating oneself mentally into a front facing person’s position in order to duplicate their movement requires more time and probably involves different neural mechanisms than when spontaneous copying is performed. In short, the front-facing OBT task is more difficult. Thus the question arises at which back to front yaw rotation angle the OBT task is considered more difficult than the SPO task and/or processing delays appear.
Compared to healthy controls the ability to perform movements in the SPO and OBT modes was impaired in patients with obj-BD (as determined by balance control during stance and gait tasks) and feelings of dizziness, as overall movement latencies were longer, amplitudes and velocities lower with respect to HCs. Those with dizziness only (DO) had little differences with respect to HCs. Therefore, we would argue that poor balance control and feeling dizziness, rather than feeling dizziness alone, affects both embodied (spontaneous) and disembodied (OBT) processing and, of the two, OBT based movements are more affected by the balance deficit. These results indicated that not only is there a global impairment in mental representation of rotation of bodies in patients with balance deficits as Grabherr et al. [18] found for bilateral loss patients, but also there is an impairment for the action based on the mental representation of rotation of the instructor’s body. Our patients had deficits in balance control and had dizziness. Therefore, we assume that this disabling combination leads to the global spatial impairment as dizziness alone led to no impairment with respect to controls. In our task, an action based on the transformation was delayed in patients with balance deficits. None of our patients had complete vestibular loss. The study of Grabherr et al. [18] required only a verbal indication of the transformation in a body part illustration but no action. The verbal indication was only delayed in patients with complete vestibular loss not in those with a partial loss. Furthermore, in our task, the action based on the body transformation involved a vestibular dependent motor task – leaning trunk roll. Thus we would argue the combination of transformation plus action based on the transformation lead to delays in those with partial vestibular loss.
For our SPO task, subjects always reacted consistent with an embodied self-location, i.e. as a mirror image response. Further, latencies were shorter for this task compared to OBT task. In these respects, our results differ for both patients and controls from those of Thirioux et al. [48] who reported longer reaction times for the SPO compared to the OBT task for healthy subjects. Furthermore, these authors reported that SPO movements were in the same direction as the OBT responses, i.e. not mirror imaged for the front and back facing avatar. The study of Thirioux et al. [48] did, however, use a different measurement procedure. Their subjects had to press one of two buttons on a rod they were holding to indicate when they reached maximum amplitude of lean to the left or to the right displayed by the avatar. Thus an additional motor task was involved in comparison to our study which depended solely on an objective measurement of the subject’s lean and not on the subject’s assessment of the maximum lean and its direction. Such an additional motor task could have caused a change in the measured reaction time and direction. For our paradigm the sum of the latency and interval until maximum lean were not different for the SPO and OBT tasks in controls (see Table 1). We have, however, no explanation of the apparent difference between the SPO and mirror image tasks regarding movement direction in the work of Thiriouxet al. [48].
Although it can be expected that different neural processes are involved with the SPO and OBT movements, it is nevertheless interesting to investigate neural correlates of these differences. Differences in evoked potentials in the left temporo-parietal junction were recorded by Thirioux et al. [48] between the SPO and OBT tasks and it was suggested that this region was involved in disembodied self-location. Because the change in activation occurred between 500 and 600 ms [48], and movement onsets were well before this period in healthy controls (see Fig. 3), we would argue that such activity would be a confirmation signal that the movement direction fitted the internal body representation. Interestingly, this activation would occur before the onset of OBT movements in obj-BD patients (see Fig. 3), providing temporal support for the concept of Thirioux et al. that delays, albeit pathological, in processing at the temporal-parietal junction could influence movements involving the disembodied self-location concept. A more direct timing confirmation of differences in the SPO and OBT modes is provided by the work of Blanke et al. [7]. These authors found that transcranial magnetic stimulation at the temporo-parietal junction 330–400 ms after onset of a stimulus indicating which mode of movement (mirror image or OBT) to choose interfered with the disembodied self-location concept. This is exactly the period between the onset of SPO and OBT movements in healthy controls (273 and 436 ms, respectively (see Table 1), suggesting the decision to initiate an OBT movement is influenced by activity in this region.
The longer latencies in SPO for obj-BD patients could be the result of patients being more anxious about losing balance during the trials. Also, the smaller amplitude of trunk-lean compared to controls in both SPO and OBT tasks could be due to anxiety about losing balance when leaning more, having learned that leaning further could bring them out of balance. It is known that vestibular loss leads to overreactions in the roll plane and subsequent instability [1, 4]. However, it is not known how chronic state and condition anxiety affect balance in patients with vestibular loss. However, one can postulate that the sudden changes brought about by an anxiety concerning falling could lead to neural processing delays and the delayed responses we observed. This hypothesis would involve a different effect of condition anxiety on balance deficit patients to that observed with healthy controls. Healthy subjects have, if any changes in latency, shorter latencies due to stronger responses if balance is perturbed when they are put in a situation at height where they are anxious about falling [11]. Increased responses amplitudes are the result of increased vestibulo-spinal [35] and muscle stretch reflex [22] gains with height-induced anxiety.
Our evidence that patients with obj-BD 1) had more errors in the OBT mode, 2) longer latencies in the OBT task compared to controls and 3) larger differences between the SPO and the OBT latencies compared to controls, support our hypotheses concerning the deficits in the embodied and disembodied self-location processes in patients with obj-BD and dizziness. This significant difference was not observed in patients with dizziness alone. Furthermore, the results suggest that patients with obj-BD were often unable to transform themselves into the body of the instructor and therefore leaned to the wrong side. Secondly, the longer OBT-latencies for obj-BD patients suggest that they had greater difficulty in processing movements for the OBT task. Because latencies were also longer in the SPO task compared to the control groups, this result could simply be due to patients with obj-BD being more occupied with keeping balance during the task. If this was the case, the latency differences between SPO and OBT trials should be the same for patients and controls. But as mentioned before, this was not the case. On the contrary, latency-differences between SPO and OBT movement onsets were twice as large in the obj-BD patient group compared to HCs and DO patients. Therefore, these results indicate that patients with dizziness and obj-BD took longer to process the transformation of themselves “into” the instructor’s body.
It should be noted that using the SPO task to compare between groups allowed us to compare their movement abilities in the absence of a difficult cognitive task. An alternative would have been to use the back-facing OBT task as comparison as this was similar in task difficulty to the SPO task.
It is also possible that the impairment in OBT tasks for the obj-BD group could be explained by a general deficit in mental rotation in vestibular loss subjects. There is evidence that the vestibular system plays a role in mentally rotating objects [33]. Furthermore, although we asked subjects to consider themselves rotated into the body of the instructor, it is possible that the obj-BD group may have used a different strategy referring to their own body [23] for the rotation and this change in strategy lead to the deficit we observed.
Clinical relevance and the need for further studies
The results of this study indicate that part of the disequilibrium in patients with chronic balance disorders may have its origin in their restricted body cognition and their limited ability to transform themselves into another location. Comparison of OBT to SPO movements may help quantify the central processing deficit of those with chronic balance disorders. Furthermore, incorporating these different movement concepts into rehabilitation programmes may help people with balance problems. To clearly identify the role of those cognitive aspects on balance, the effect of OBT training tasks on SPO and OBT movement differences needs to be examined in detail. If the simple training of own body transformation to another location leads to a better balance control, this would underline the importance of body cognition and own body transformation on balance control in patients with chronic balance disorders.
The question arises whether, because of the novel nature of the OBT task, it can be used to quantify the effect of training or therapy. Possibly, the use of the other psychometric measures and balance measures described in this report are better suited for this purpose. Future studies will need to explore this question.
Clinical application
A mental training approach, involving a switching between the SPO and OBT forms of postural control, has to our knowledge not yet been investigated, but may provide a huge potential in balance rehabilitation. Mental training to date has been limited to imagining a task being performed without actually performing it physically. It has not involved mentally switching the mode of performance from embodied to disembodied. Practice imagining a task is intended to improve its physical execution [30, 47]. However, according to Malouin & Richards [30], this imagery practice could be with the trainee imagining another person moving (external imagery - disembodied), or he can imagine himself moving (internal imagery - embodied). Mental practice has be shown to be an efficient aid to regaining of motor function in people with physical disabilities and is also well known as a method to enhance physical performance in athletes [39]. Thus one way to achieve an improvement in patients with balance disorders would be to imagine and perform balance movement tasks in which the physiotherapist stands in front of the patient. The patient would first have to imagine switching between embodied to disembodied movements, and then be asked reproduce the exercise movement switching between SPO and OBT modes.
Study limitations
A number of drawbacks are present in this study. Firstly, the number of subjects was limited to 16 in each patient group. Nonetheless our results were highly significant especially between the HCs and patients with dizziness and obj-BD. Significant differences were not found between the DO group and HCs. However, it is possible that with a larger number of subjects significance between the latter 2 groups would have been obtained. Secondly, several patient and a few HC measurements from the first OBT movement trial were not used, because the subjects did not perform the movement correctly. It is also possible that these incorrect first trials also provide information on deficient central processing in patients with chronic balance disorders.
Because we did not counter-balance between SPO and OBT trials being presented first, we did not control for first-trial effects. First trial effects in the form of delayed latencies were only seen in the SPO not OBT trials. This first trial effect would have acted opposite to the effect of increased latency we observed for OBT compared to SPO trials. Thus, if we had counter-balanced presentation order we would have expected an even greater difference between SPO and OBT latencies.
Also, the two tasks (SPO and OBT) were not matched for task difficulty. It is possible that the obj-BD patients have a global deficit for difficult cognitive tasks which might have been apparent with a control task matched for task difficulty with the OBT task. However, both the SPO and OBT movement onsets were delayed for the obj-BD patients with respect to the DO and HCs. Thus, although a general influence of task difficulty on the obj-BD patients cannot be ruled out, an effect of the balance deficit was also noted for the simpler SPO tasks. Thus, it is more likely that the balance deficit patients had longer cognitive processing delays for both tasks, due to the need for increased attention integrating vestibular and proprioceptive information during the leaning task [46].
Another point which should be mentioned is the homogeneity and the distribution of diagnoses in the patient group. While the three diagnostic types we used for the patients with obj-BD are representative for patients among the chronic balance disorders population [10] studies with larger numbers of patients within each type may yield differences in disembodied and embodied body perceptions.
It could be argued that the patients with phobic postural vertigo (PPV) should in the group with dizziness only (DO). However, these patients clearly had deficits in balance control not present in the DO group. The form of the balance deficit - easier stance and gait tasks showed excessive trunk sway whereas harder to perform balance tasks had normal sway - fitted previous descriptions of PPV patients as did their obsessive-compulsive behaviour [9, 38]. Although we could not find an organic reason for their unstable balance, this does not mean that one did not exist. Standard clinical tasks were carried out to test for vestibular function. Tests of utricle function using vestibular evoked myogenic potentials of ocular muscles [31, 42] were not performed. Thus we cannot rule out an utricle pathology in these patients. It is also possible that the high values of phobic anxiety (the PPV patients were among the highest scores in the BSI category) influence both vestibulo-ocular and -spinal reflexes in these patients [45].
Conclusion
Our results indicate that movements which require an own body transformation are deficient in patients with chronic balance disorders and impacts their balance control. This knowledge improves understanding in cognitive aspects of balance control and provides a theoretical basis for the development of clinical trials of balance control. We would suggest including disembodied cognitive training into balance deficit therapy in order to train this contribution of central processes to balance control.