
Abstract
INTRODUCTION:
Head impulse test (HIT) is the critical bedside examination which differentiates vestibular neuritis (VN) from posterior circulation stroke (PCS) in acute vestibular syndrome (AVS). Video-oculography based HIT (vHIT) may have aadditional strength in making the differentiation.
METHODS:
Patients admitted to the emergency department of a tertiary-care medical center with AVS were studied. An emergency specialist and a neurologist performed HIT. vHIT was conducted by an neuro-otology research fellow.
RESULTS:
Forty patients 26 male, 14 female with a mean age of 49 years were included in the analyses. Final diagnoses were VN in 24 and PCS in 16 patients.
In the VN group, clinical HIT was assessed as abnormal in 19(80%) cases by the emergency specialist and in 20(83%) by the neurologist. In all PCS patients, HIT was recorded as normal both by the emergency specialist and the neurologist (100%).
On vHIT, patients with VN had significantly low gain values for both the ipsilesional and contralesional sides when compared with the healthy controls, with significantly lower figures for the ipsilesional side (p < 0.001). All patients in this group had normal DWI-MRI.
PCS patients had bilaterally low gain (p < 0.05) on vHIT. However, gain asymmetry was not significant. Subgroup analyses according to presence of brainstem involvement revealed bilateral low gain (p < 0.05) in patients with brainstem infarction (anterior inferior cerebellar artery-posterior inferior cerebellar artery stroke, AICA-PICA stroke) whereas patients with pure cerebellar infarction (posterior inferior cerebellar artery-superior cerebellar artery stroke, PICA-SCA stroke) had gain values similar to healthy controls.
With a gain cut-off ≤0.75 and gain asymmetry cut-off ≥17%, as determined by ROC analysis, 100% of PCS patients and 80% of VN patients were correctly diagnosed.
CONCLUSIONS:
Clinical HIT, either performed by an emergency specialist or neurologist is equivalent to vHIT gain and gain asymmetry analysis as conducted by neuro-otologist in the diagnosis of PCS, albeit mislabeling about 20% of VN patients. vHIT does not appear to yield additional diagnostic information. These findings indicate the strength of clinical HIT. Pure gain-based vHIT analysis seems limited and needs to be incorporated with saccade analysis.
Keywords
Introduction
Acute vestibular syndrome (AVS) is a clinical syndrome of new onset continuous vertigo, nausea/vomiting, motion intolerance and gait instability lasting days to weeks [9]. It has been reported to be the diagnosis in approximately 10 to 20% of dizzy patients admitted to emergency departments in US [24]. The most common causes are vestibular neuritis (VN) in ∼70% and posterior circulation stroke (PCS) in ∼25% [24]. Though not considered as a stroke symptom previously [5], recent evidence has revealed that isolated vertigo is a common PCS presentation [9, 20]. Therefore, it is critical to differentiate stroke patients from patients with VN admitted to the emergency department with features of AVS. Current evidence indicates that bedside examinations mainly involving eye movements can distinguish central lesions from peripheral ones [9, 10]. HINTS battery involving head impulse test (HIT), nystagmus, test of skew have approximately 99% sensitivity in diagnosing PCS [16, 23], whereas magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI) has a sensitivity of 80% to 85% in the first 24 to 48 hours [16, 18].
The highest sensitivity component of the battery is the horizontal HIT of vestibulo-ocular reflex (VOR) [7]. Clinically a unilateral abnormal HIT has been found in approximately 92% of cases with acute VN [21]. It is present in less than 10% of stroke patients generally those involving the labyrinth, vestibular nerve or nucleus [11]. A sensitivity of ∼91% and specificity of ∼100% has been reported for central lesions in AVS [16].
Quantitative HIT, both video-oculography (VOG) based HIT testing (vHIT) [14, 17] and the gold standard, search coil [3], have been previously studied in AVS and can separate VN from posterior inferior cerebellar artery (PICA) strokes. However, anterior inferior cerebellar artery (AICA) strokes were at risk of being misclassified based on VOR gain alone but were correctly classified by corrective saccade analysis [3].
In this study our first aim was to assess the reliability of the clinical HIT results in the emergency department to differentiate VN from PCS in AVS. The second aim was to see if vHIT measurements yielded additional information in making the differentiation.
Patients and methods
The method was similar to two previous studies [3, 14]. Patients presenting to the emergency department of a tertiary-care medical center with AVS who had acute vertigo, nystagmus, nausea or vomiting and unsteady gait of less than 3 days in onset were enrolled in a prospective cross-sectional study from December 2013 to March 2016. Patients with a previous history of vestibular or ocular motor disorders were excluded. All patients gave written informed consent and the study was approved by the institutional ethics committee. The patients underwent structured bedside examination including the HINTS battery [9] plus bedside hearing by finger rub [16] first by an emergency specialist (FK) and then by a neurologist (AG) who were blinded to each other’s findings. Diagnosis of suspected central or peripheral lesion were made without knowledge of patient history.
The noninvasive, quantitative video-oculography device (ICS Impulse, GN Otometrics, Taastrup, Denmark) was used to measure and record eye movements. The vHIT was conducted by a neuro-otology research fellow (CK). The operator stood behind the subject to hold the head and instructed the subject to focus on a target approximately 1 meter away. The lateral canals were stimulated with the head inclined forward 30 degrees. At least 20 random impulses with unpredictable timing with amplitudes of 5–20 degrees and a head velocity of 50–250 degrees/second were performed. All vHIT trials were assessed by an expert masked neuro-otologist (NÇ) to classify as interpretable (no artifacts or fast eye movements during the VOR) or uninterpretable. For comparison vHIT recording was performed in 29 age and sex matched healthy controls. Gain asymmetry was determined by using the formula used in a previous study [25] which is as follows:
contralateral gain-ipsilateral gain/contralateral gain+ipsilateral gainX100.
The diagnosis of VN was determined by the presence of unidirectional spontaneous nystagmus obeying Alexander’s law or unilateral gaze-evoked nystagmus with the fast phase directed away from the vestibular deficit, abnormal clinical HIT, no neurologic signs including absence of skew deviation and normal DWI.
Any finding in the HINTS battery suspicious for a central lesion i.e. presence of direction changing nystagmus, a negative clinical head impulse test or skew deviation indicated PCS.
All patients underwent MRI to confirm final diagnosis. Lesion was determined by a neuroradiologist (CE); abnormal DWI was diagnosed as PCS.
Statistics
The IBM SPSS Statistics 23 software was used for the statistical analyses. The Shapiro–Wilk test was performed to check if the numerical data was normally distributed in each group. Parametric tests were used as normal distribution was conformed. Comparison of the numerical data between groups was performed by one-way ANOVA. Homogeneity of variances was tested by Levene statistics. As the variances were homogeneous, pairwise comparisons following ANOVA was performed by Bonferroni test. Paired t-test was used to test the significance of difference between the ipsilesional and contralesional VOR gains. Receiver operating characteristic curve analysis was used to identify potential quantitative cut-off points for differentiating VN from PCS. Categorical variables were compared with Chi-square test. All the tests were performed at a 0.05 level of significance (p < 0.05).
Reliability assessment
The Kappa statistic was used to document inter-rater reliability and was reported as an overall mean with standard deviation. Kappa statistic <0.00; poor, 0.00–0.20; slight, 0.21–0.40; fair, 0.41–0.60; moderate, 0.61–0.80: substantial and 0.81–1.00; excellent were agreement between physician raters. p-value of less than 0.05 was considered to be significant.
Results
Fifty-two AVS patients admitted to the Emergency Department of Ege University Medical School were present. Five were excluded because of a lack of confirmatory neuroimaging. Three patients could not cooperate with vHIT testing. In 4 patients vHIT results were accepted as uninterpretable. Therefore 40 patients 26 (% 65) male, 14 (% 35) female with a mean age of 49 years (19–82 years) were include in the analyses. Final diagnoses were VN in 24 and PCS in 16 patients (Fig. 1).
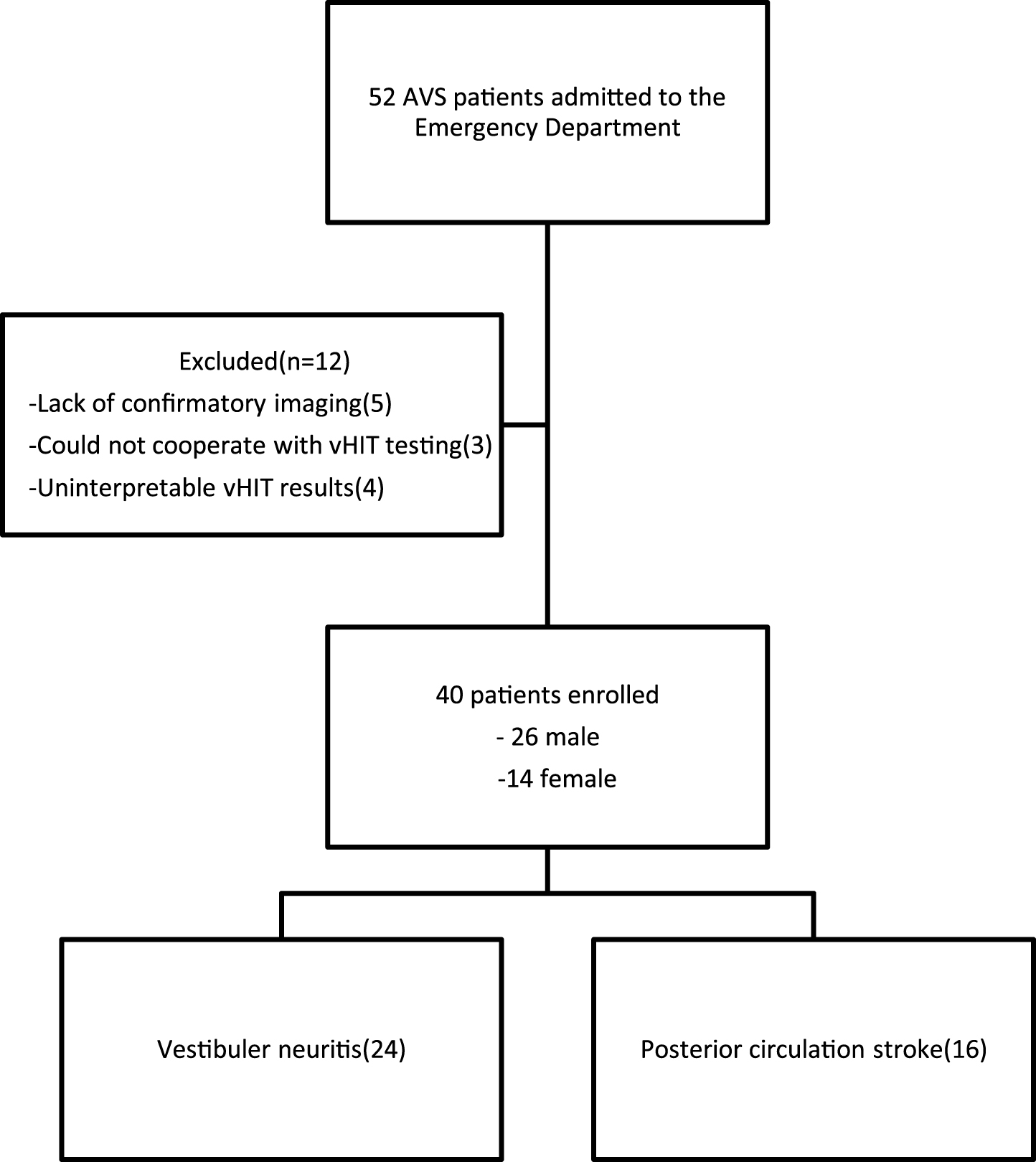
Flow diagram of patient screening, enrollment and final diagnosis
In 24 VN patients (12 male, 12 female) the mean age was 46 years (range 19–82 years). Unidirectional spontaneous nystagmus was present in 9 and unilateral gaze-evoked nystagmus was present in 6. Clinical HIT was assessed as abnormal in 19(80%) cases by the emergency specialist and in 20(83%) by the neurologist. Four patients who were found to have clinically normal HIT by the neurologist had unilateral low gain and gain asymmetry on vHIT and normal DWI indicating that the final diagnosis is VN.
In 16 patients (14 male, 2 female) with PCS the mean age was 52 years (range 26–80 years). None had additional cranial nerve or long tract sign. Skew deviation was present in two (patient 11 and 13). Two patients; one with a right lateral medullary+ cerebellar infarction and another with a right pontomedullary+ cerebellar infarction had left beating nystagmus (patient 3 and 11). Direction changing nystagmus was noted in seven (patients 2, 4, 6, 8–10, and 12). In all clinical HIT was clinically assessed as normal both by the emergency specialist and the neurologist (100%). PCS was further classified radiologically into subgroups according topography and vascular anatomy. In 9 with brainstem infarction, either alone or associated with cerebellar infarction (patient 3, 5, 7, 10, 11, 13–16), this was categorized as AICA-PICA stroke. In 7 with pure cerebellar infarction without brainstem involvement (patient 1, 2, 4, 6, 8, 9 and 12) this was designated as PICA-SCA stroke (Table 1).
Clinical and radiological features of patients with posterior circulation stroke
P, Patient; L, Left beating; DCN, Direction-changing nystagmus; ES, Emergency Specialist; Neu, Neurologist; PICA, Posterior inferior cerebellar artery; AICA, Anterior inferior cerebellar artery; SCA, Superior cerebellar artery.
The conformity of clinical HIT results reported by the emergency specialist and the neurologist was excellent and the κ coefficient was 0.86.
VOR gains in healthy controls and patients are given in Table 2. When compared with the results of healthy controls VOR gains of patients with VN were low both for the ipsilesional and contralesional sides reaching a statistical significance (p < 0.001 and p = 0.001 respectively). Gain asymmetry of 37.7% (±20.2%) was also statistically significant (p < 0.001).
VOR gains in patient groups and healthy controls recorded by vHIT
VOR: Vestibulo-ocular reflex. vHIT: Video head impulse test.
Typical vHIT recordings of VN and all 16 PCS are presented Fig. 2a and b respectively. Comparison of the VOR gains of PCS with the healthy controls showed that low gain values were present both for the ipsilesional (p = 0.036) and contralesional (p = 0.021) sides. However, gain in AICA-PICA stroke was reduced both for the ipsilesional (p = 0.005) and contralesional sides (p = 0.008) without significant asymmetry (p = 0.71). In PICA-SCA stroke VOR gains were not different from the healthy controls ipsilesionally (p = 1.00) or contralesionally (p = 0.96) and there was no asymmetry (p = 0.065) (Table 2).
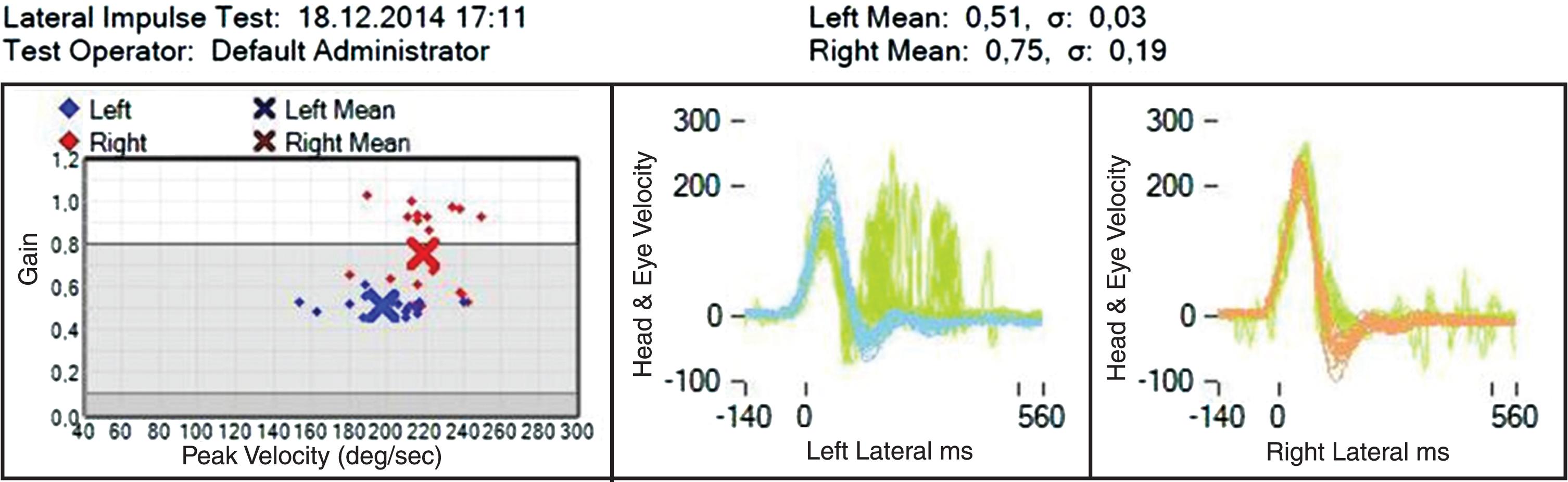
Asymmetrically reduced VOR gain and overt saccades on the left side in a patient with vestibular neuritis

(b) vHIT recordings and MRI findings of the patients with PCS within the order of Table 1. (vHIT: video head impulse test, PCS: posterior circulation stroke).
Cut-off points for vHIT gain were determined by receiver operating characteristic curve (ROC) analysis. The specificity was 93% at gain values ≤0.75 when the sensitivity was 96% for the VN group (AUC = 0.977, SE: 0.017, 95% CI = 0.944–1.00, p < 0.001). In 23 of the 24 VN gain values were ≤0.75. One of the 7 (14%) PICA-SCA stroke and 4 of the 9 (44%) AICA-PICA stroke had gain values ≤0.75. Gain asymmetry ≥17% was found to have a sensitivity of 79% (19/24) and a specificity of 84% in diagnosis of VN (AUC = 0.896, SE:0.04, 95% CI = 0.818–0.974, p < 0.001). None of the 7 PICA-SCA strokes and just one (11%) AICA-PICA stroke had an asymmetry ≥17%. With both gain ≤0.75 and asymmetry ≥17% taken into consideration, 100% of PCS were correctly diagnosed but only 80% of VN were correctly identified.
In this study, clinical HIT was found to be abnormal in about 80% of VN patients, regardless of speciality (emergency speciality: 80%; neurologist 83%). In all of the 16 PCS (100%) HIT was found to be normal both by the emergency specialist and the neurologist. Clinical HIT allows identification of a peripheral vestibular deficit with a sensitivity ranging from 34% to 100%; complete vestibular loss is associated with the highest sensitivity [2, 21]. Incomplete vestibular loss, improper technique due to slow head impulses and being conservative in rating HIT as deficient may explain normal HIT in our VN patients. We confirm that frontline clinicians, irrespective of specialty, can confidently diagnose PCS based on normal HIT. Abnormal clinical HIT has been reported in 9% to 39% of patients with acute cerebellar or brainstem strokes [1, 15]. We found 100% sensitivity, perhaps due to clinicians cognizant about the possibility of HIT in PCS and therefore more likely to undercall abnormal HIT.
Head impulses mainly drive the short latency, oligosynaptic VOR pathways from the semicircular canals to the extraocular muscles. It is known that high acceleration reveals VOR deficits better and elicits larger overt catch-up saccades [25]. Catch-up saccades that are imperceptible to clinical detection, termed covert saccades, are generated while the head is still moving and reduces the sensitivity of the test. Repeated testing has also been suggested to avoid false-negative results [25]. Clinicians with neuro-otological experience had lower HIT sensitivity (due to being more conservative in rating an abnormal HIT) and higher specificity (better in identifying normal HIT) than clinicians without experience [8]; the disagreement was mainly restricted to mild deficit. The authors advised ordering quantitative measurements, such as search coil or high speed video methods when clinical HIT is not conclusive.
vHIT has been shown to measure VOR gains accurately, equivalent to search coils, and can identify peripheral vestibular deficits in patients with VN [13]. Both ipsi- and contralesional VOR gains detected by vHIT in our VN patients were low when compared to healthy controls and substantial asymmetry was present. Mildly reduced contralesional gains has previously been reported [22], possibly reflecting contribution to the VOR from ipsilateral canal excitation only when contralateral canal inhibition is saturated by high acceleration head impulse. The “on” and “off” direction gain asymmetry can be explained by push-pull cooperation between the coplanar canals; the VOR, especially at higher head acceleration, is driven better by ipsilateral canal excitation than contralateral canal inhibition [25].
VOR gains of our PCS patients were bilaterally low without a prominent asymmetry. This was due to AICA-PICA strokes, as subgroup analysis showed that gains recorded from PICA-SCA strokes was not different from healthy controls (Table 2). AICA strokes have been reported to show abnormal VOR gains that can be confused with a peripheral lesion [3, 14]. Structures supplied by AICA, such as vestibulo-oculomotor substrates and the oligosynaptic pathways connecting them, are likely affected [12]. Our AICA-PICA stroke had bilaterally reduced gains which was also reported in previous studies [3, 14] and a case report with isolated floccular infarction [19]. The explanation seems to be the reciprocal interneuron connections between the vestibular nuclei as it is the case in VN, causing compensatory inhibition of the contralateral vestibular nucleus, and the modulating role of flocculus on VOR in floccular lesions [3, 19].
Our PICA-SCA stroke patients had normal and symmetrical vHIT gains. Previous studies on PICA strokes have shown normal clinical HIT in 99% of patients [24, 16]. Normal vHIT results has been reported and high-frequency VOR pathways was suggested to be unaffected in ischemia of the lateral medulla and inferior cerebellum [14], both supplied by the PICA. However, a search coil study reported 20% reduction in gains in PICA-SCA stroke [3], suggesting technical factors, such as goggle slippage, were likely to account for normal range VOR gains in our PICA-SCA stroke patients.
ROC analysis showed that using a gain cut-off ≤0.75, 96% of our VN patients could be diagnosed with a specificity of 93%, but alarmingly 44% of AICA-PICA and 14% of PICA-SCA strokes also had gains ≤0.75. Using such gain cut-off would detect most VN, but incorrectly diagnose nearly one in two AICA-PICA stroke and one in seven of PICA-SCA stroke as VN. A previous vHIT study has shown about 90% specificity and sensitivity, using a gain cut-off 0.75 [14]. In our study using a gain asymmetry ≥17% plus gain cut-off ≤0.75 improved diagnostic accuracy, with 100% AICA-PICA strokes correctly diagnosed and about 80% of VN detected. However disappointingly this degree of diagnostic certainty was not different from the percentage achieved by clinical HIT. vHIT analysis did not add much in making the diagnosis as both diagnostic methods led to similar percentage of VN being misdiagnosed. A search coil study has shown exceptional diagnostic accuracy with both HIT gain and corrective saccade analysis [3]. Although search coil is unlikely to be in widespread clinical use, its superiority over vHIT is unquestionable and raises the possibility that technical factors and artefact render vHIT gain less diagnostically helpful.
Other than five patients with neuroimaging inadequacy, seven of the 52 AVS patients had to be excluded as three could not cooperate with vHIT testing and four had vHIT results uninterpretable comprising approximately 14% of the overall group. We did not repeat clinical and video HIT evaluation, and it is possible that diagnostic accuracy might change over time, as the effect of ischemia can be rapidly evolving. Our results cannot be generalized to other causes of AVS, such as Meniere’s disease and vestibular migraine.
In conclusion for now clinical HIT, performed by emergency physicians or neuro-otoologists, seems adequate in diagnostic evaluation AVS. If vHIT is undertaken then both gain and gain asymmetry should be taken in account. In the future the sensitivity of vHIT analysis for PCS diagnosis needs to be increased, possibility by incorporating saccade analysis, further refinement in video technology and increased operator proficiency.
Footnotes
Acknowledgments
The authors would like to thank to Associate Prof Timur Kose PhD for his contributions for the statistical analysis.