
Abstract
The diagnostic criteria for Meniere Disease (MD) are clinical and include two categories: definite MD and probable MD, based on clinical examination and without the necessity of advanced vestibular or audiological testing. The condition is a heterogeneous disorder and it is associated with endolymphatic hydrops (EH), an accumulation of endolymph in the inner ear that causes damage to the ganglion cells. Patients with suspected EH can be examined by Magnetic Resonance Imaging (MRI), offering new insights into these inner ear disorders. Results of imaging studies using the hydrops protocols show conflicting results in MD patients. These discrepancies can be dependent either on the MRI sequence parameters or on the method of hydrops grading or the inclusion criteria to select patients. The visualization of EH can be classified based on a semi-quantitative ratio between endolymph and perilymph liquids, or on the distinction between the saccule and the utricle structures. In addition, MRI can also be used to evaluate whether cochleovestibular nerves can present with imaging signs of axonal loss.
In this systematic review, we have selected case-controlled studies to better characterize the potential added value in the diagnosis and management of patients with MD. Using different techniques, studies have identified the saccule as the most specifically involved structure in MD, and saccular hydrops seems to be associated with low to medium-tone sensorineural hearing loss degree. However, early symptoms still appear too subtle for identification using MRI and the reproducibility of the hydrops protocols with various MRI scan manufacturers is debatable, thus limiting expansion of these techniques into clinical practice for the diagnosis of MD at this time.
Further research is needed. The future inclusion of semicircular canal hydrops location in the imaging signs and the application of MRI in patients with atypical presentations hold promise.
List of Acronyms
Meniere’s disease
sensorineural hearing loss
Endolymphatic Hydrops
Magnetic Resonance Imaging
Inversion Recovery
Intratympanic
Intravenous
Gadolinium-based contrast agent
Introduction
Meniere disease (MD) is a clinical syndrome defined by episodes of spontaneous vertigo usually accompanied by tinnitus, pressure within the ear and fluctuating sensorineural hearing loss (Table 1) [1]. The syndrome is a heterogeneous condition and several comorbidities have been consistently associated such as autoimmune arthritis [2, 3], psoriasis [4] or migraine [5, 6]. The molecular pathophysiology is starting to be deciphered and different mechanisms including rare allelic variations in autosomal dominant familial MD [7–9], common allelic variants such as rs4947296, which regulates the expression of TNF receptors and NFkB-mediated inflammation in mononuclear cells [10] or alterations in the innate immune response with elevated levels of pro-inflammatory cytokines IL1, IL6 and TNFα [11], seem to contribute to the development of the phenotype. Regardless of the involved molecular mechanisms, the episodes of vertigo have a higher frequency in the first 5 years of the disease [12], but the hearing loss usually progress during the first 5–10 years [13], leading to an accumulation of endolymph (termed endolymphatic hydrops, EH) in the cochlear duct and the vestibular organs (saccule, utricle, ampullae), that has been demonstrated in human histopathological studies [1, 15].
Diagnostic criteria for diagnosis of Meniere disease
Diagnostic criteria for diagnosis of Meniere disease
In the last decade, numerous imaging studies from various research teams have shown the feasibility of in vivo visualization of EH by Magnetic Resonance Imaging (MRI) and its pathological consequences on the auditory or vestibular systems. This new imaging application is mainly due to the efforts of Prof Naganawa’s team in Nagoya (Japan) who developed all the steps needed for the scientific validation in humans, including technical development of the acquisition sequences and application to various disease models [14]. However, the reproducibility of MRI sequences to evaluate the amount of endolymphatic fluid as well as the system of hydrops classification have been recently challenged [15–18] in case-controlled studies, and the usefulness of the MRI hydrops protocol remains debatable in clinical practice.
In this systematic review, we will discuss the observation of endolymph accumulation with MRI. We will start by briefly outlining the physical basis of MRI sequences for the hydrops protocol including the pitfalls and quality criteria, before discussing findings from case-controlled diagnostic trials testing its usefulness in patients with MD and future directions of research.
This review has been conducted using the criteria recommended by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Selection of studies
The assessment and selection of the studies was performed according to the following aspects: Participants definition, Intervention, Control studies, main and secondary Outcome measure and Study design (PICOS): Participants: a) individuals with diagnosis of MD according to 1995 or 2015 diagnostic criteria, b) sensorineural hearing loss without vestibular symptoms and c) vestibular migraine according to Barany Society 2012 diagnostic criteria. Intervention: MRI acquisition with different sequences using either IT or IV GBCA (Gadolinium-based contrast agent), both or no GBCA Control group: control and non-control studies Outcome measures: EH visualization in the cochlea or vestibule Secondary outcomes: other data related to main diagnosis such as duration of disease or hearing threshold. Study design: randomized case control studies, cases series or cross-sectional studies.
Search strategy
A structured search using PubMed was performed on the 25th of July 2018, and included all relevant articles published. The search used the following key word combinations: “MRI” AND “Endolymphatic Hydrops” (n = 389). Two reviewers have then selected articles published in and after 2013 (n = 146). Moreover, references of the retrieved articles were also inspected to extract any further relevant publications.
After title and abstract review, the search resulted in 52 individual articles from which additional relevant articles were identified upon examination of the cited references. After having eliminated 3 articles on the basis of non-English language and 35 articles that consisted of letters, reviews and uncontrolled studies, 13 articles were assessed and included in the review for a total of 833 individuals (Table 2).
Case control studies of MRI in patients with MD (N = 13)
Case control studies of MRI in patients with MD (N = 13)
Importantly, we have excluded studies where the contralateral ears of patients with unilateral MD were used as reference, since bilateral involvement may occur in 10–50% of cases [19]. Other reviewed studies were only focused on methodological development of the hydrops sequence and knowledge coming from temporal bone analysis, both for the purpose of understanding MRI of the inner ear. The findings coming from the 13 selected studies are separately discussed. However, non-controlled studies were also reviewed to compare the differences in the methodology.
The main objective of this review is to determine if visualization of EH on MRI can be used as diagnostic criteria for MD. For this, information was retrieved from each selected publication regarding patient inclusion criteria, number of patients, duration of disease, use of gadolinium-based contrasts, image acquisition technique and other technical aspects such as inversion time with FLAIR, and location of EH (cochlea, vestibule, semicircular canals).
Data extraction, synthesis and quality evaluation
From each study the following information was extracted: first author, year of publication, journal, type of study (controlled/case series), sample size, patient inclusion criteria and the clinical and technical variables described above. The Cochrane Collaboration Tool was used to assess the quality of each study and the risk of bias.
Results
Knowledge from non-controlled studies and methodological pitfalls
MRI sequence physical basis
Hydrops MRI currently relies either on Inversion Recovery (IR) sequences in the vast majority of publications [15, 20–24], or Heavily-Weighted T2 Gradient Echo sequences in a few other scientific articles [25–27].
Using IR sequences, the method of MRI EH evaluation requires contrast media injection and delayed acquisition, in order to selectively enhance the perilymphatic fluid. The signal from one of the two inner ear liquids, the endolymph, is cancelled out. The two inner ear liquids have very close T1 and T2 relaxation times such that the proposed contrast to assess endolymphatic filled spaces, i.e., hyposignal for endolymphatic spaces and hypersignal for perilymphatic spaces, relies on very slight variations in sequence parameters.
Some studies obtain the inner ear contrast by subtracting two IR sequences with different Inversion Time [28, 29] or by merging the 3D-FLAIR sequence with the T2-Weighted sequence [30, 31]. Clinicians should interpret these images with caution to exclude description of endolymph in non-physiologic compartments due to geometric coregistration problems between the two sequences [18]. In addition, it is now possible to acquire one 3D-FLAIR sequence to estimate the distribution of endolymphatic fluid with good inter-reader reproducibility [17]. The 3D-FLAIR sequences are now widely available with all MRI manufacturers without requiring post-processing techniques, yet the signal of the endolymph is similar to those of temporal bone, requiring training for interpretation [32].
Finally, other publications [25–27] proposed MRI analysis through heavily T2 weighted-sequences. It is important to mention that only Gradient-echo sequences (FIESTA sequence for General Electric manufacturer, balanced FFE for Philips and CISS for Siemens) can be used for this purpose because of the low Repetition Time and Echo Time, rendering the sequence sensitive to the presence of inner ear membrane such as those of the saccule. The main problem encountered for clinical practice is movement artifacts with B0 field inhomogeneities, and it is often difficult to confirm that the “black band” effect, which is presumed to be the lateral wall of the saccule, is not artefactual. It is very difficult to map the utricle and the cochlear duct membranes with T2-weighted sequences with 3T or 1.5T MRI scans due to the low spatial resolution although these sequences are much more efficient in evaluating the cranial nerves size in the internal auditory canal by measuring its diameter.
Contrast media diffusion
Two alternative routes for contrast media administration have been assessed: intratympanic (IT) and intravenous (IV). The main advantage of an IT injection is a higher perilymphatic contrast, particularly in the basal turn if the cochlea, although previous studies suggest this method can cause local toxicity in animal models [33], and it requires an MR scan waiting time of 24 h before imaging acquisition. In addition, patients with bilateral MD will require a double IT injection. Partial or complete obstruction of the round window and enlargement of the endolymphatic space could also complicate inner ear analysis after IT injection [34]. One research team has also proposed to inject the contrast media through the Eustachian tube [35], without significant differences with classic IT injection.
The intravenous method requires a shorter waiting time, which has been evaluated as optimal in the 4–6 hour interval [36, 37]. More recently, the effect of varying the contrast media molecule on normal inner ear structures enhancement has been assessed [38]; moreover, the use of 3D-FLAIR sequences with constant flip angle seems to be more sensitive that those with variable flip angle for exploring patients with MD, owing to the higher sensitivity to a low dose of contrast media [39].
Knowledge from controlled studies
Thirteen case-controlled studies were selected. Ten of them have stated the inclusion criteria for MD (5 used the 1995 AAO-HNS criteria and 5 used the 2015 Barany Society criteria), and 3 of them did not mentioned any criteria (Tables 1 and 2). The 3D-FLAIR sequence was used in 6 control studies (inversion time range 2100–2400 ms), but it was not described in 9 studies. Seven studies used IV Gadolinium-based contrast agents and 4 studies did not used contrast. Remarkably, the duration of disease was only reported in 3 studies, and this variable probably may explain the large variability observed among studies.
Semi-quantitative grading system
Two grading methods for the EH degree classification have been proposed. The first grading system, proposed by Nakashima et al. [40] with application in a recent case-controlled study [22], divided EH grades into three categories: none, mild and significant, both in the cochlea and the vestibule. This semi-quantitative grading system was initially based on the histopathology of the dilated endolymphatic spaces, with separate evaluations for the vestibule and the cochlea. Interestingly, the vestibular EH was significantly different between ears with MD and control ears; however, the utricle and saccule were not individually assessed.
Another limitation for the three-stage grading of Nakashima et al. is that it is easy to shift from the normal condition to EH simply by varying the Inversion Time sequence by 100 ms [15, 16]. The use of an anatomical landmark such as the utricle to do a relative qualitative diagnosis of saccular expansion has proven to be less sensitive to acquisition condition, yet not perfect for saccular hydrops diagnosis [15]. The semi-quantitative classification has the advantage of encompassing the cochlear duct for hydrops diagnosis. However, some studies have suggested a lower specificity in patients with MD [17, 22]. A recent meta-analysis of temporal bone studies also proposed a cochleocentric distribution of the endolymph fluid with constant cochlear duct dilatation in healthy subjects [41], explaining the frequent visualization of endolymph in normal cochlear ducts with MRI.
Saccular and utricular grading system
In temporal bone studies, EH typically involves the pars inferior of the labyrinth, mainly the saccule [42]. Saccular hydrops, can range from mild to severe, based on the degree of membrane distension toward the stapes footplate, as seen in post-mortem studies [43]. Furthermore, the degree of distension of the inner ear structures appears to be related to their mechanical compliance, which is high in the case of the saccule, but lower for the utricle and semi-circular canals [44]. Case-controlled studies have proposed a new measure based on the size and morphology of the saccule obtained using a 3D-FLAIR sequence, the saccule to utricle ratio inversion (SURI) (Fig. 1). The current limitations of this classification are the absence of a cochlear duct evaluation and difficulty distinguishing the utricle from the saccule in most severe cases of saccular hydrops [32]. The absence of inclusion of grading for utricular protrusion into the lateral semicircular canal following IT contrast media injection [45] could limit this classification’s usefulness.
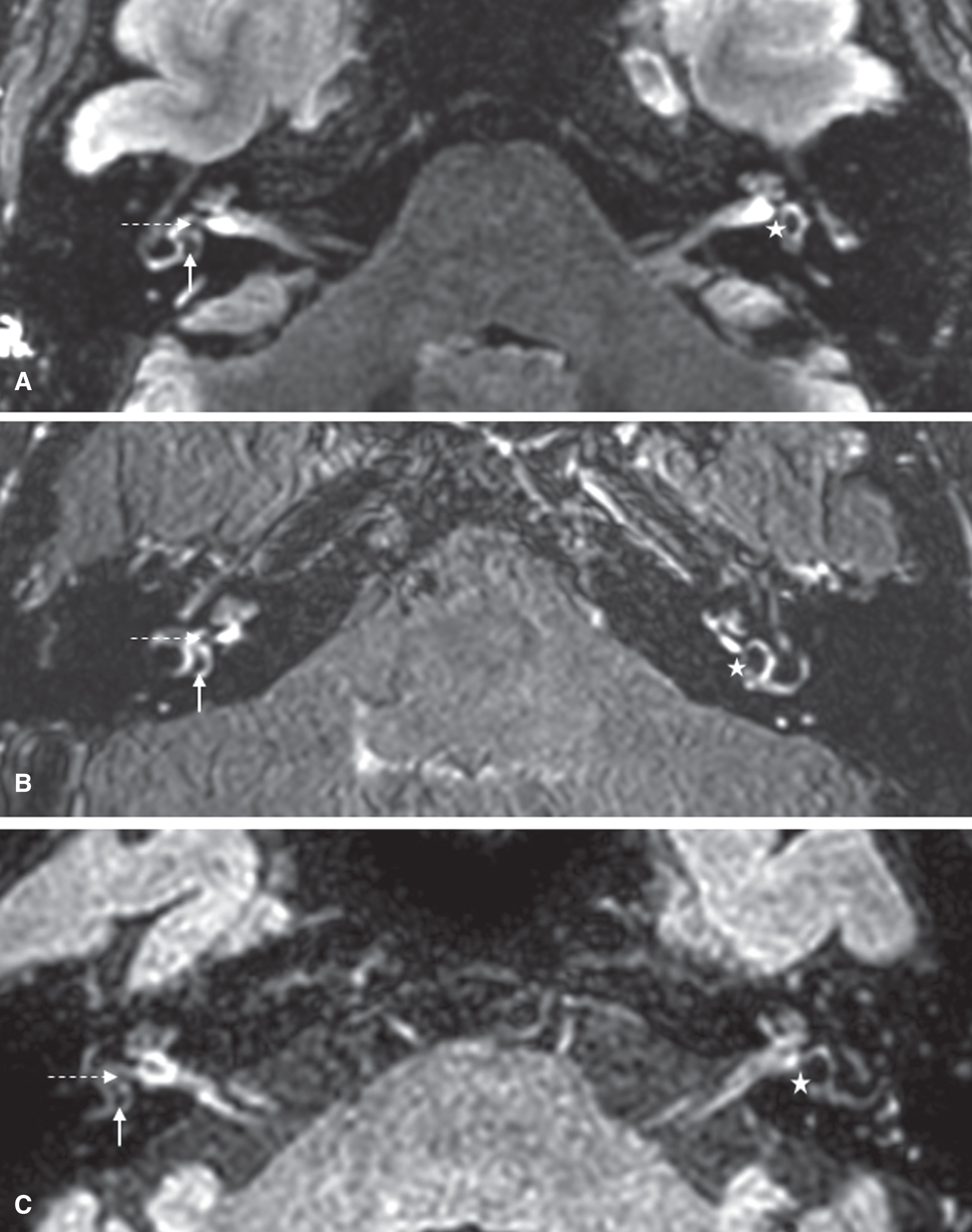
3D-FLAIR sequences in the axial slice of reference in 3 different patients with MD with left saccular hydrops, as assessed with the SURI method. Patient A was explored with a General Electric ® MRI scan, patient B with a Siemens ® MRI scan, and patient C with a Philips ® MRI scan. For the right inner ears, no saccular hydrops is detected; the saccules (dotted arrows) appear smaller than the utricles (white arrows). For the left inner ears, saccular hydrops is detected; the utricles were not visible whereas the saccules (white stars) were seen at the inferior part of the vestibule. These pictures are extracted from the online database available for researchers [32].
Three different research groups have demonstrated saccular expansion in patients with MD: Venkatasamy et al. [27] have compared high-resolution T2-weighted images of the saccule in normal subjects with histological sections from cadavers to identify saccular changes in MD compared to healthy volunteers. They found no correlation between the presence of saccular hydrops and the duration of the disease or the degree of hearing loss. Saccular abnormalities were found in 84% of patients with MD with bilateral damage in 30% of patients with MD. Saccular hydrops was found to be associated with the presence of hearing loss, unilateral hypofunction on vestibular testing, or time since the last crisis. Simon et al. [26] measured saccular height and width in a coronal plane for MD patients. The estimated sensitivity and specificity was 63% and 95% for height, and 41% and 95% for width, respectively, for the symptomatic ear The inter-rater reliability was 0.76 for height and 0.51 for width measurements.
Finally, Attyé et al. have investigated the relationship between the presence of saccular hydrops and clinical presentations in three studies. In the first study, which corresponds to the first mention of the SURI method, they found that 15 of 30 patients with MD presented with saccular hydrops in the symptomatic ear [17]. Saccular hydrops was compared in three groups patients including those with isolated SNHL, those with recurrent vestibulopathy and definite MD, and a control group. They demonstrated that saccular hydrops is associated with SNHL thresholds above 40 dB, while vertigo patients without SNHL do not have saccular hydrops. Furthermore, saccular hydrops was described in patients without a clinical diagnosis of MD, and in subjects with isolated low-tone sensorineural hearing loss [21]. In another publication, the same group further confirmed that inner ear MRI showed hydrops when hearing loss was greater than 35 dB [20].
We have not found any MRI studies describing EH in patients with familial MD or in patients with clinical variants of MD [6]; moreover, there are no longitudinal MRI studies in patients with MD, which would be very useful to determine the time needed to develop EH.
Differential diagnoses for MD
A large retrospective case-controlled study including 200 patients with MD has shown that besides saccular hydrops, radiologists must be vigilant regarding other inner ear disorders, such as perilymphatic fistulae, inner ear malformations or brain lesion along central cochleovestibular pathways, which may mimic MD symptoms [46]. The presence of perilymphatic fistulae in patients with MD symptoms was not associated with saccular hydrops.
MRI studies of internal auditory canal cranial nerves
The principal central pathway for audition and equilibrium leading to the cerebral cortex passes from the labyrinth, via the cochlea-vestibular nerve (VIII), to the brainstem nuclei. Sensorineural degeneration of cochlear and vestibular nerves has been proposed to occur in patients with MD [47, 48] while EH should be considered as a histologic marker for MD rather than being directly responsible for its symptoms [49].
Henneberger et al. and Flatz et al. measured both the VIII nerve and the VII nerve via their diameters in MD patients compared with controls [50, 51] using MRI. They demonstrated swelling of these nerves in patients with MD group, raising the hypothesis that although cellular death would theoretically be expected to lead to a decreased nerve thickness, the increases in the diameter of of VII and VIII nerves support a mechanism of neuroinflammation in MD pathophysiology.
Conclusions
Conclusions on methods for MRI studies in MD
Although there is some variability in the method to visualize EH, the most common sequence is 3D-FLAIR combined with IV GBCA. For 3D FLAIR-based studies, the inversion time is critical to discriminate perilymph versus endolymph and it is not described in most of the studies.
Conclusions on MRI findings in MD
MRI EH can be reliably measured in the saccule using the SURI method. EH in the saccule is associated with hearing loss and probably with the duration of disease. Uncontrolled studies have described EH in patients with vestibular migraine, acute low tone SNHL (without vertigo), tinnitus regardless of hearing loss, and autoimmune inner ear disease.