
Abstract
BACKGROUND:
Since the first description by Hallpike and Cairns, the excess of endolymphatic fluid, also known as endolymphatic hydrops (EH), has been established as being the main biomarker in patients with Menière’s disease. Recently, the concept of primary (PHED) and secondary hydropic ear disease (SHED) has been introduced. PHED corresponded to Menière’s disease while SHED was defined as the presence of EH in patients with pre-existing inner ear disease.
OBJECTIVE:
In this article, we would like to summarize the methodology of hydrops exploration using MRI and the previously published radiological findings in patients with PHED and SHED.
RESULTS:
Before the emergence of delayed inner ear MRI, the presence of EH was assumed based on clinical symptoms. However, because of the recent technical developments, inner ear MRI became an important tool in clinical settings for identifying EH in vivo, in patients with PHED and SHED. The presence of EH on MRI is related with the degree of sensorineural hearing loss whether in patients with PHED or SHED. By contrast, in PHED or SHED patients without sensorineural hearing loss, MRI showed no sign of EH.
CONCLUSIONS:
Thanks to the recent technical developments, inner ear MRI became an important tool in clinical settings for identifying EH in vivo, in patients with PHED and SHED.
Introduction
In 1938, Hallpike and Cairns pointed out the excess of endolymphatic fluid, also known as endolymphatic hydrops (EH), as being the main biomarker in patients with Menière’s disease (MD) characterized by recurrent spells of vertigo, hearing loss, tinnitus and aural fullness [13, 21]. Various factors leading to the development of EH have been suggested, including excessive endolymph production, decreased endolymph absorption, ionic imbalance, viral infection and allergic responses [3].
EH might be idiopathic (= MD), which is the more common type, or might be acquired if caused by inflammatory or traumatic insult to the labyrinth. Recently, Gürkov introduced the concept of primary (PHED) and secondary hydropic ear disease (SHED) [12]. PHED included the clinical “cochleo-vestibular” phenotype, which corresponds to definite or probable MD, and the “vestibular” or “cochlear” phenotype, which corresponds to possible MD. In these patients, no identifiable cause for EH was found. By contrast, SHED was defined as the presence of EH in patients with pre-existing inner ear disease such as infections, trauma, and tumors.
Over the last decade, inner ear MRI became an important tool in clinical settings for identifying EH in vivo, in patients with MD. Since the first studies of the Nagoya group research, other research teams aimed to improve hydrops exploration on MRI and to clarify the mystery of the inner ear [27, 41].
In this article, we would like to summarize the methodology of hydrops exploration using MRI and the previously published radiological findings in patients with PHED and SHED.
State of the art: Imaging of endolymphatic hydrops
How to perform the MR “hydrops” protocol?
In 2007, Nakashima et al. were the first to report EH on MRI in living patients, based on the selective enhancement of the perilymphatic space 24 hours after the intratympanic administration of contrast media [5]. Later, the same research team also showed that the evaluation of the endolymphatic and perilymphatic spaces was possible 4 hours after the intra-venous administration of contrast media [31].
The main advantage of contrast intratympanic administration is a higher perilymphatic signal; al-lowing the use of 3D-real inversion recovery seq-uences [41]. Indeed, these MR pulse sequences are less sensitive to gadolinium but enable the visualization of endolymph, perilymph and bone in a single image [18]. However, due to its invasiveness, and since there were no demonstrated differences in the detection rate of EH between intratympanic and intravenous methods, the latter is now widely employed [18]. In addition, intratympanic administration is not suitable for patients with middle ear diseases.
The intravenous method requires a shorter waiting time (4 hours) and allows in the same time frame to evaluate indirectly the permeability of the blood-labyrinthine barrier (BLB), which cannot be evaluated with intratympanic administration. It also implies studying the endolymphatic space in both ears, which is crucial since some patients might also present EH in asymptomatic ears. Using the intravenous method, 3D-FLAIR sequences have been used since they are more sensitive to T1-shortening than 3D-real inversion recovery sequences, thus al-lowing detection of any subtle enhancement [25]. However, as the contrast remained slightly lower when using an intratympanic injection, several studies have proposed post-processing techniques, for example fusion of gray-scale inverted positive endo-lymph with native positive perilymph images or FLAIR and T2 sequences co-registration [2, 28].
As reported by other teams, we also believe that 3D-FLAIR sequences using a constant flip angle instead of a variable flip angle, were sufficient to provide a good contrast-to-noise ratio without requiring any post-processing technique [6, 38].
How to diagnose EH on MRI?
In the last decade, most studies have used the semi-quantitative grading system first introduced by Naka-shima et al [31]. They have evaluated separately the area of the endolymphatic space in the cochlea and the vestibule entirely. Cochlear and vestibular EH were defined by an area ratio (areaendolymphatic space /areaperilymphatic space) greater than 33%. However, some authors have suggested that this grading was not specific, since healthy subjects could present with cochlear duct dilatation, a finding also observed in histopathological studies. Moreover, a case-controlled study also demonstrated that the utricle occupied more than 50% of the vestibular area in 15% of healthy subjects [3].
Based on these findings, Attyé et al. proposed an anatomical grading system based on the saccular morphology, also known as the saccule to utricle ratio inversion (SURI) [1, 3–5]. This anatomical grading system has been revised by Conte et al. who described the vestibular endolymphatic space (the saccule) contacting the oval window (VESCO sign), and lately, by Bernaerts et al. who performed a four-stage hydrops classification in combination with cochlear BLB impairment [6, 8].
However, none of these classifications have in-cluded utricular and ampullar hydrops in the grading using intravenous injection of contrast media. Lately, Kahn et al. have published a new anatomical-based grading system taking in consideration each compartment of the endolymphatic space and also the presence of cochlear BLB impairment [16]. The degrees of EH in the vestibule and cochlea were assessed on axial slices by visual comparison of the hypointense signal areas (cochlea, saccule, utricle and ampullas) from the endolymphatic space versus the hyperintense signal of the perilymphatic space.
The degree of cochlear hydrops was categorized as being (Fig. 1): none; grade I: when the area of the endolymphatic space exceeded the area of the scala vestibuli. We did not consider the cochlear duct to be pathological when its area was less than the scala vestibuli since 30% of healthy subjects might present this finding [43]. The degree of saccular hydrops was defined as (Fig. 1): none, grade I (when the saccule appeared larger or equal to the utricle, surrounded by perilymphatic space, also known as the SURI sign), grade II (when the saccule was in contact to the oval window, without surrounding perilymphatic space, also known as the VESCO sign). The degree of utricular hydrops was defined as (Fig. 2): none, grade I (herniation of the utricle in the non-ampullated part of the lateral semicircular canal), grade II (when there was no more surrounding perilymphatic space). The degree of ampullar hydrops was defined as (Fig. 2): none, grade I (when there was no surrounding perilymphatic space). The presence of cochlear BLB impairment was also evaluated and was defined as a marked enhancement in the perilymph of the basal turn of the cochlea, as previously reported [6].
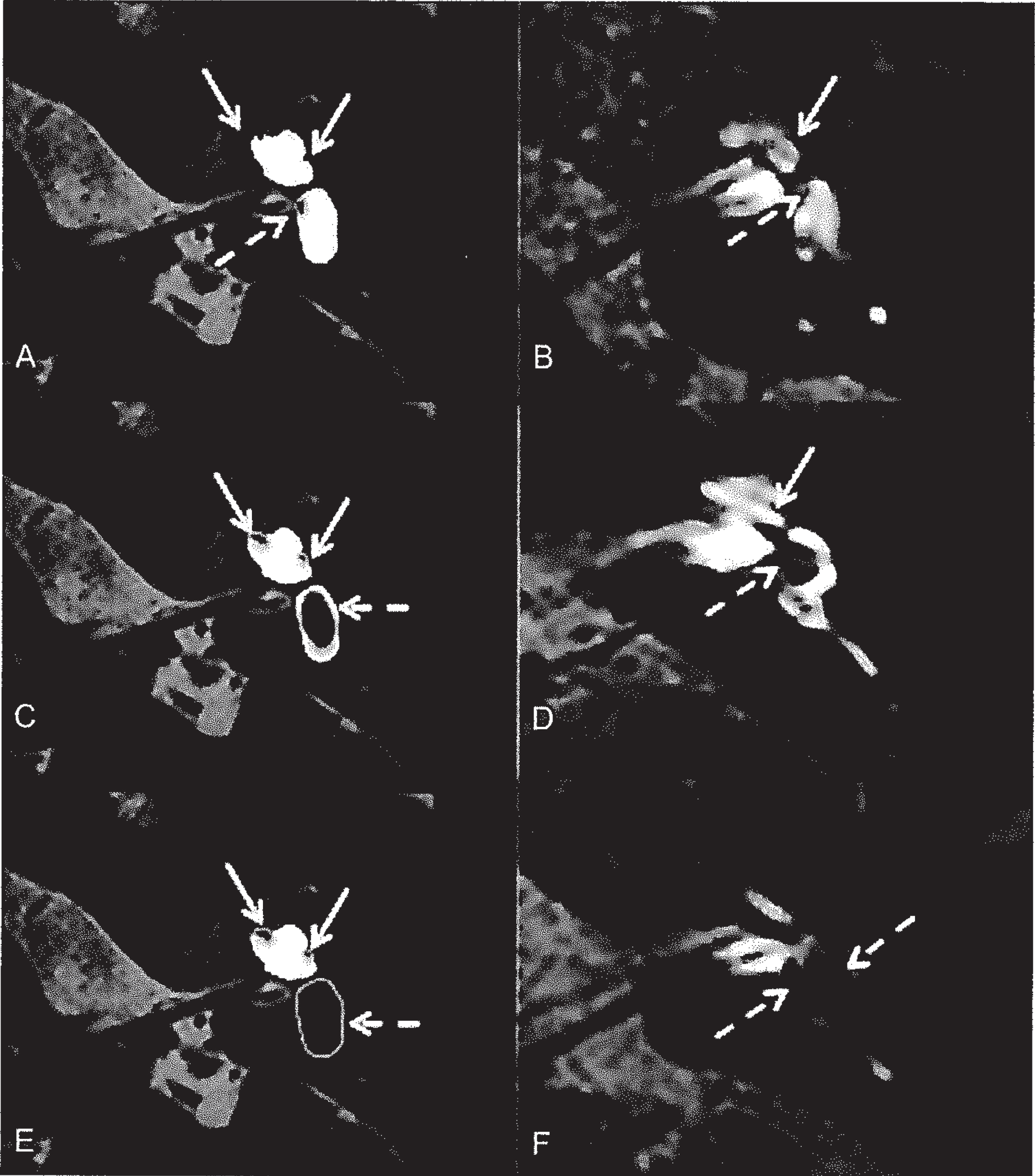
Cochlear and saccular hydrops grading. A-B: Axial section in through the inferior part of the vestibule showing normal saccule (dotted white arrow) and cochlear duct (white arrow). C-D: Axial section through the inferior part of the vestibule demonstrating left cochlear hydrops (white arrow) saccular hydrops (Grade I, white dotted arrow) surrounded by perilymphatic fluid with no contact with the oval window. E-F: Axial section through the inferior part of the vestibule showing left severe saccular hydrops (Grade II, white dotted arrow) without surrounding perilymphatic fluid.
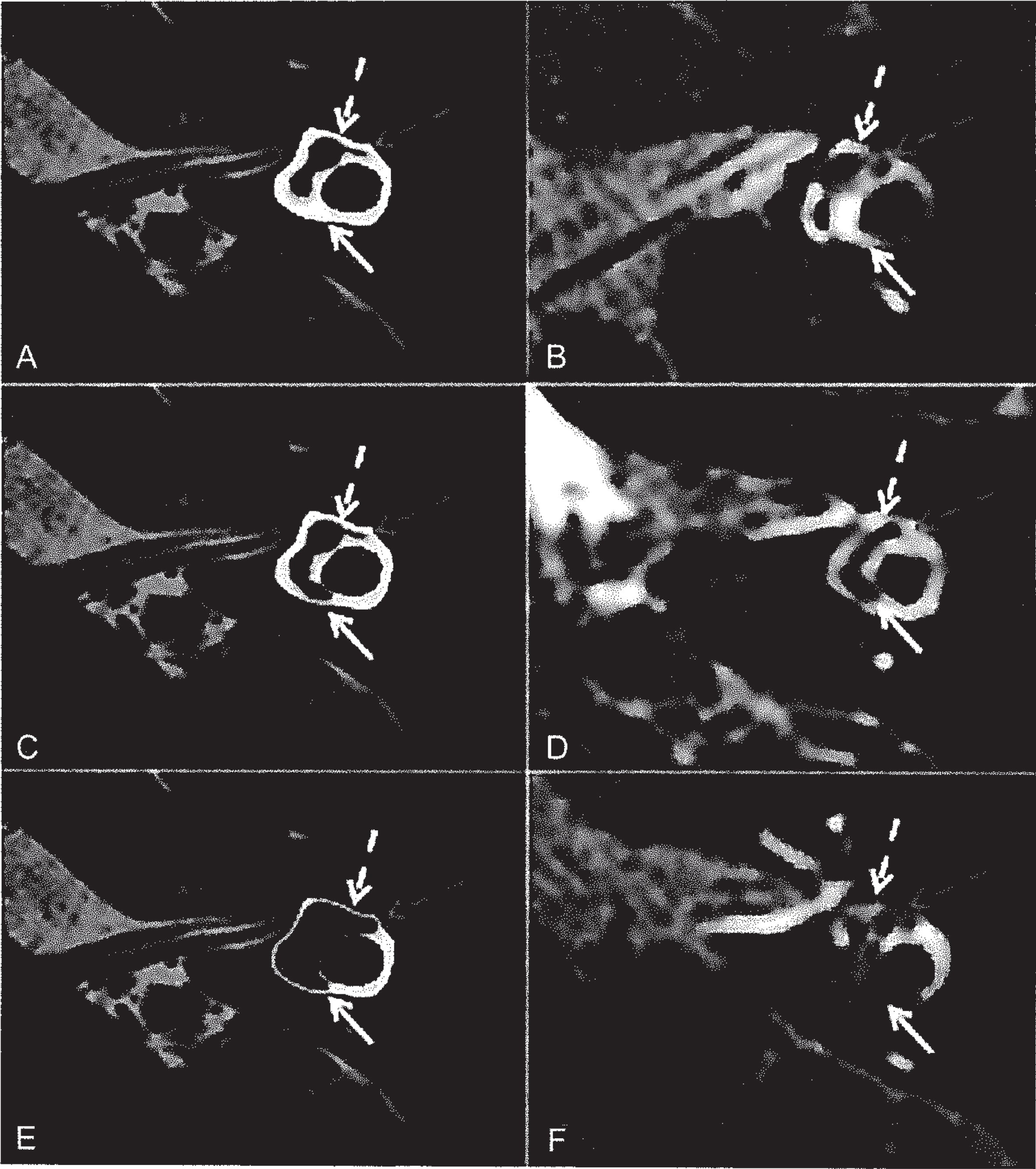
Utricular hydrops grading. A-B: Axial section through the superior part of the vestibule at the level of the lateral semicircular canal (white arrow) showing normal utricle (dotted white arrow) and lateral ampulla (gray dotted arrow). C-D: Axial section through the superior part of the vestibule at the level of the lateral semicircular canal (white arrow) and lateral ampulla (gray dotted arrow) demonstrating a protrusion of the left utricle (dotted white arrow) in the non-ampullated part of the lateral semicircular canal (Grade I, white dotted arrow). E-F: Axial section through the superior part of the vestibule at the level of the lateral ampulla (gray dotted arrow) demonstrating a severe dilatation of the left utricle (dotted white arrow) with no surrounding perilymphatic fluid and a protrusion in the non-ampullated part of the lateral semicircular canal (Grade II white arrow).
In a meta-analysis of histopathological studies, Pender demonstrated that the lesion distribution in MD was cochleocentric, involving the cochlea, then the saccule, the utricle and at a later stage, the ampullas [34]. Using the compartmental grading system on MRI in patients with definite MD, we observed the same pattern of distribution: saccular, utricular and ampullar hydrops were respectively found in 91%, 45% and 8.5 % of cases. Utricular hydrops was always associated with severe saccular hydrops and ampullar hydrops was always associated with severe utricular hydrops. For this reason, we have raised the hypothesis that when the compliance of a compartment was overstretched, contiguous extension of the dilatation in each endolymphatic space could occur. As reported by other authors, we also found a significant correlation between the severity of EH and the degree of hearing loss, which is considered to be linked to the severity of the disease [7]. Moreover, most patients with Tumarkin crisis had severe vestibular EH on MRI [14], involving in some cases, even the ampullas.
Using this compartmental MRI grading, contralateral EH in asymptomatic ears was observed in 15% of definite MD while using the semi-quantitative grading system, other studies have reported EH up to 65% of cases. It has been reported that 30% of MD patients had bilateral endolymphatic hydrops on histopathological studies [14], which seems to be “in-between” various reported values using MRI.
In patients with low-frequency sensorineural hearing loss (fluctuating or not), which are analogous to the cochlear form of MD as defined by the AAO-HNS 1995 guidelines, saccular hydrops is constantly observed for hearing loss above 40 dB [5, 7]. By contrast, in patients with the vestibular form of MD (also known as recurrent vestibulopathy), saccular hydrops is never observed, suggesting another physiopathological mechanism [5].
In a previous study, Quatre et al. have demonstrated that the electrocochleography and distortion product otoacoustic emissions were more sensitive than inner ear MRI for the diagnosis of EH in the early stages of the disease [36]. Indeed EH on MRI, as assessed using the SURI score, was only observed for hearing loss over 40 dB. By contrast, Kahn et al. showed that, in the later stages of the disease, inner ear MRI was more sensitive (91%) than cervical vestibular-evoked myogenic potentials (48%) and ocular vestibular-evoked myogenic potentials (32%) [16]. The authors have suggested that EH occurred before impairment of the hair cells. However, these results should be interpreted with caution since the clinical utility of vestibular-evoked myogenic potentials as a measure of otolithic function has limitations.
As the endolymph fluid is absorbed by the endo-lymphatic sac, it has been presumed that this site was the origin of EH in MD. This theory of abnormal longitudinal flow has been reinforced by temporal bone specimen studies, which have shown that there was calcification of the vestibular aqueduct [23]. Based on these findings, Attyé et al. demonstrated a reduction in aqueduct wall visibility on delayed 3D-FLAIR sequences, reinforcing this theory [1]. Calcifications of the vestibular aqueduct on cone-beam CT have also been previously reported in patients with MD [40]. Recently, we have demonstrated that the absence of visible vestibular aqueduct on temporal bone CT could predict the presence of EH on MRI with high positive predictive value (93.1%) [20].
Imaging of secondary hydropic ear disease
Over the past decades, histopathological studies have reported that EH might also be the result of different lesions of the inner ear. Nowadays, inner ear MRI enables to confirm this hypothesis in living patients with for example clinical manifestations of delayed EH, Minor syndrome, large vestibular aqueduct syndrome, vestibular schwannoma, intracranial hypotension and otosclerosis [10, 37, 39].
In patients with superior semicircular canal dehiscence syndrome, the symptoms are linked with the presence of a third mobile window caused by a bone defect of the superior semicircular canal, which potentially leads to low-tone air-bone gap, autophony, hyperacusis, aural fullness and pulsatile tinnitus. Patients can also experience vertigo revealed by Valsalva maneuver and Tullio sign.
Moreover, some studies have raised the hypothesis that some patients with superior semicircular canal dehiscence syndrome might show sign of EH on MRI. Using the semi-quantitative grading system, Sone et al. have reported EH in 80% in only 5 SCDS ears [39]. In our center, by using the compartmental grading system, EH was observed in only 9 out of 33 SCDS ears (27.3%) and was correlated with the degree of sensorineural hearing loss [37]. Since superior semicircular canal dehiscence syndrome and EH symptoms can overlap and otolithic tests might be altered in the affected ears in both SCDS and MD patients, inner ear MRI might enable to diagnose a subset of patients with SHED.
In patients with otosclerosis, the origin of sensorineural hearing loss is uncertain and various mechanisms have been considered including direct injury of the spiral ligament of the cochlea and endolymphatic hydrops (EH) [15, 19]. Using the semi-quantitative grading system, Wang et al. found that vestibular EH was present in 15 out of 27 otosclerotic ears (55.5 %) causing elevation of hearing thresholds and becoming a possible high-risk factor for complications after stapes surgery [44]. Using the compartmental grading system, EH was surprisingly observed in only 1 out of 39 (2.6%) otosclerotic ears [16]. The low rate of EH in our study contrasts with the previous literature in which vestibular endolymphatic hydrops is a frequent finding in otosclerotic ears (between 26.1% and 55.5%) on MRI [24, 44]. However, in a series of 95 temporal bones, Liston et al. described EH in only 6 cases (6.3%) [19]. In our opinion, the most likely explanation for this discrepancy relies on the poor specificity of the semi-quantitative grading system for EH detection. More importantly, in our study, the only case of EH was observed in one patient that presented an extensive capsular otosclerosis with hypodensities (CT scan) surrounding the vestibular aqueduct. Based on this finding, we have suggested that the underlying mechanism of EH in this patient was caused by an obstruction of the vestibular aqueduct by an otosclerotic focus, which may create a disturbance of the outflow and/or absorption of endolymph, leading to the development of EH [42].
In patients with vestibular schwannoma, due to the increased protein concentration in the perilymphatic space, it is possible to assess the endolymphatic space without contrast media administration, with T2-weighted and/or 3D-FLAIR sequences [10, 26]. The elevated perilymphatic protein induces a fall in signal in the perilymphatic compartment, spontaneously contrasting with the endolymph, which still shows normal hyperintensity on T2-weighted sequences [10]. In a previous study using high-resolution T2- weighted sequences, we found a correlation between hearing loss and utricular hydrops while we found no correlation with saccular hydrops [10].
In patients with intracranial hypotension, EH is also possible, sometimes mimicking Menière’s disease, caused by an equilibration of pressure between cerebrospinal fluid and perilymphatic space, in cases of patent cochlear aqueduct [11]. Recently, one radiological study demonstrated EH of the lateral ampulla in a patient with SIH that presented hearing loss and dizziness, followed by orthostatic headache [11]. EH of the ampulla is uncommon in Menière’s disease patients occurring at a later stage of the disease [16, 34]. Yet, the physiopathological mechanism might be different in patients with spontaneous intracranial hypotension. In our experience, 2 out of 3 patients with intracranial hypotension and cochleovestibular symptoms, presented EH on delayed inner ear MRI [35].
Conclusion
Here, we summarized the methodology of hydrops exploration using MRI and the previously published radiological findings in patients with PHED and SHED.
Before the emergence of delayed inner ear MRI, the identification of EH was based on the clinical symptoms, highly evocative when the patient presented the full clinical triad. However, because of the recent technical developments, inner ear MRI became an important tool in clinical settings for identifying EH in vivo, in patients with PHED and SHED. The main finding was that EH is related with the degree of sensorineural hearing loss whether in patients with PHED or SHED and cochlear or cochleovestibular phenotype. By contrast, in patients with PHED or SHED and vestibular phenotype, MRI showed no sign of EH.
Footnotes
Acknowledgments
We thank Pamela Haylock (Lariboisiere University Hospital) for critically editing the manuscript.
Conflict of interest
The authors have no conflicts of interest to disclose.
Financial disclosure
No financial disclosure