
Abstract
BACKGROUND:
During walking, postural stability is controlled by visual, vestibular and proprioceptive input. The auditory system uses acoustic input to localize sound sources. For some static balance conditions, the auditory influence on posture was already proven. Little is known about the impact of auditory inputs on balance in dynamic conditions.
OBJECTIVE:
This study is aimed at investigating postural stability of walking tasks in silence and sound on condition to better understand the impact of auditory input on balance in movement.
METHODS:
Thirty participants performed: walking (eyes open), tandem steps, walking with turning head and walking over barriers. During each task, acoustic condition changed between silence and presented noise through an earth-fixed loudspeaker located at the end of the walking distance. Body sway velocity was recorded close to the body’s center of gravity.
RESULTS:
A decreased body sway velocity was significant for walking (eyes open), tandem steps and walking over barriers when noise was presented. Those auditory stimuli did not affect sway velocity while walking with turning head. The posture has probably improved due to the localization ability when walking with the head facing forward, while the localization ability was impaired when turning the head.
CONCLUSIONS:
The localization ability of a fixed sound source through the auditory system has a significant but limited impact on posture while walking.
Introduction
Nowadays, it is well understood to what extend the sensorineural systems such as the visual, vestibular and proprioceptive system influence postural stability. Though, auditory input can be assumed to effect postural control as well. Beside the well-known comorbidities between the hearing and vestibular peripheral sensors due to the close anatomical conditions there is evidence for a neurophysiological connection between vestibular and hearing system [1, 5]. Burian and Gstoettner [5] observed in guinea pigs by investigating the vestibular nuclear complex, first order neurons from descending vestibular nerve root to the dorsal cochlear nucleus (DCN). Secondary vestibular afferent nerve fibers to the DCN in rabbits were found by Bukowska [4]. Barker et al. [1] treated anaesthetized rats with an acoustic overexposure of 100 dB SPL at a single frequency tone (14.8 kHz). They found an increased expression of a vesicular glutamate transporter in the DCN as a projection from the lateral vestibular nucleus (LVN). Afferent nerve pathways from cerebellum mainly and some from vestibular organ converge in the LVN. In turn, nerve fibers from LVN form the lateral vestibulospinal tract and pass the spinal cord. Its axons end at motor neurons which lead to an upright and balanced posture. Some fibers from LVN ascend to the nuclei of the oculomotor nerve for the reflective eye movement. However, the cerebellum is, in addition, anatomically and functionally connected with the auditory system [3, 26]. Connections were demonstrated between the cochlear nucleus and the vermis area of the cerebellum as well as between the dentate nuclei of lateral hemispheres in cats [9, 24]. Activations of the cerebellum and some areas of lateral hemispheres were shown by functional imaging techniques for different listening tasks [3, 26].
The localization ability and therefore the orientation in a room might have an impact on postural control during walking. Cues such as interaural time and level differences of sound are decisively for localize a sound source. Our brain analyzes both signals, from right and left ear, in time and level differences to determine the direction the sound is coming from. If the sound source is located right handed of the head, the sound reaches first the right and then the left ear. Furthermore, the sound level is higher at the right ear than at the left ear. Interaural time difference is most efficient for lower frequencies, whereas interaural level difference is helpful for higher frequencies to localize the sound source. The head shadow effect also contributes to localization. In addition, room properties (e.g. reverberation time), position of the listener/sound source and the stimulus also affect the localization ability [7, 18]. For example, in a reverberant room, the reflections on the walls reach the ears from another direction than the sound source is located. This could lead to inaccurate localization of the sound source. In rooms with less reverberation, the localization ability is less impaired.
Studies, which investigated to what extent auditory input changes postural control under stance conditions on a balance platform, found that sound compared to silence improved postural stability [6, 22]. Zhong and Yost [27] measured the angle of the feet movements after performing the Fukuda Stepping test (100 steps, eyes closed) in silence and with noise presented from the front. The angular difference from the starting position was significantly smaller when noise was presented. Perhaps the localization ability of the sound source was crucial. Similar results were found by Karim et al. [16]. Eight participants performed the Fukuda-Unterberger test (50 steps, blindfolded) in silence, with noise presented through headphones and with noise presented through a fixed loudspeaker placed in front. Participants performed significant better in the fixed loudspeaker condition compared to silence or noise played through headphones. Furthermore, spatial acoustical cues such as reverberation time seem to influence posture as well [15]. Participants performed better in a normal clinical room compared to a semi-anechoic room. In two studies, postural control was investigated for walking in hearing impaired patients with hearing devices [20, 25]. Both research groups analyzed the postural stability in bilateral hearing aid or bilateral cochlear implant users with hearing devices turned on and off. Patients wore inertial sensors during the tasks or performed exercises on a walkway with inbuild pressure sensors. Only some patients improved with hearing devices turned on vs. off postural control.
However, postural control in motion differs from those in stance in many ways. On one hand, higher sensory-motoric integration is required to maintain postural control while the changing environment challenging during motion (e. g. new obstacles, surfaces, dual tasks). On the other hand, most of the motion movements are highly automated by central circuits. This is a completely different situation for a meaningful integration of auditory inputs for postural control. These aspects are poorly investigated until now. The aim of the present study was therefore to characterize the possible impact of an auditory input on body sway during walking conditions. This is of utmost interest since falls occur mainly during walking.
Materials and methods
Ethical approval
The Institutional Review Board (University of Berlin) approved the study protocol (approval number EA1/326/15). All experiments were carried out in accordance with the Declaration of Helsinki and all participants agreed to the informed consent.
Subjects
In this study, 30 subjects (18 females and 12 males, mean age = 25 years, range = 16–38 years) with normal hearing in pure-tone audiometric testing at 0.25, 0.5, 1, 2, 4, 6 and 8 kHz [13] (0.1 percentile), normal or corrected visual acuity of at least 0.7 logMAR (tested with Landolt rings) and no vestibular abnormalities were recruited. Saccular function was tested by recording cervical vestibular evoked myogenic potentials with an ECLIPSE® measurement system (Interacoustics, Denmark) and utricular function was investigated by performing subjective haptic vertical testing with a screening tablet (Zeisberg GmbH, Reutlingen, Germany). The functions of anterior, posterior and horizontal semicircular canals were analyzed by the video head impulse test system Eyeseecam® (Otometrics, Denmark). Performance of Standard Balance Deficit Test [2] with the Vertiguard® device showed for the participants a composite score of 29–45. A composite score below 50 means a normal age related postural stability. The participants had no history of vertigo at any time. In addition, they had to fill in the Dizziness Handicap Inventory [14]. Exclusion criteria were acute or chronic medical diseases (e.g. renal/bowel/cardiovascular disorders) and neurological diseases (e.g. depressions, anxiety, addiction). Furthermore, any neuro-orthopedic condition (e.g. arthroses of the hip/knee) and any medically prescribed drug intake influencing the balance system were exclusion criterions as well.
Room properties
The experiment was carried out in a hallway about 2.5 m wide and 16.5 m long. In order to provide a similar visual environment for all participants, all windows were blinded and artificial light with an approximated mean light flux of 320 lx (measured at head height) was applied by four ceiling lights. Also, the walls and the ceiling were white and the floor light grey. A specialist measured with the integrated impulse response method [12] a reverberation time of T30 (125–8000 Hz) = 2.46-1.05 s. The reverberation time was independent from spatial position. In silence, the sound level was 35 dB (A) and was monitored by a calibrated sound level recording system.
Procedure and setup
Participants performed the following test battery: walking with eyes open walking with eyes open with turning head to the right and to the left in rhythm tandem steps with eyes open walking with eyes open over barriers
The total walking distance was 12 m for walking with eyes open, walking with turning head and walking over barriers. For tandem steps the walking distance was 6 m. The measurement values of the first two steps and the last two steps were not included in the analysis as artifacts caused by starting and stopping the movement should be avoided. The walking distance has been divided into two sections for analyzing the postural stability and one section in between both analyzed sections to change the acoustic condition. After two steps, the first section to be analyzed began with a distance of 3 m (or 1.5 m for tandem steps). This section was followed by a distance of 4 m (or 1.5 m for tandem steps) to change the acoustic condition. The acoustic condition changed between silence as reference condition (R) and continuous (cN) or interrupted (iN) white noise presented by a fixed loudspeaker in front. Interrupted noise was generated by alternating stimulus and pause with the same duration of 0.5 s.
A second analyzed section of the same distance of 3 m (or 1.5 m for tandem steps) followed, but with noise presented. The participants continued walking for at least 1 m. Within the analyzed 3 m distance (or 1.5 m for tandem steps) participants performed 4–6 steps (or 5–7 tandem steps). Number of steps at walking over barriers was always eight as the distance of barriers was 1 m and only one intermediate step between two barriers was allowed. This setup, in which the acoustic condition changed between silence and noise while walking, was chosen to hold the motion sequence as constant as possible. In total, participants completed eight trials as each walking task was performed for reference condition combined with continuous or interrupted noise presented from the front. All four walking tasks were performed with one acoustic combination (R/cN or R/iN) until the acoustic combination changed. The noise signal was always presented in the second half of the walking distance. Furthermore, all participants were asked to perform the task over the whole distance without stopping and with their daily life walking speed as constant as possible. In addition, they were instructed to look ahead towards the loudspeaker while walking, but they were not instructed to pay attention to or to ignore the stimulus. Participants were only told how to correctly perform the task and that body sway is being measured. During the performances, the time was recorded in each analyzed section to ensure a similar walking speed. Time differences of up to 10 %between the first and the second section were accepted.
The loudspeaker (JBL Control One, frequency range 50–20000 Hz±3 dB) for presenting the stimuli was placed 2 m beyond the end of the walking distance. White broadband noise with a frequency range of 80–20000 Hz was presented at 60 dB SPL at the participant’s end position of the walking distance. All participants wore disposable socks during data recording as personal shoes are known to influence sway measurements. They also wore similarly comfortable, soft pants to ensure that no additional unwanted noise was produced by the attire of the participants.
Body sway velocity was recorded with the Verti-Guard® system (Zeisberg GmbH, Reutlingen, Germany). Two gyrometers placed orthogonal to each other measure the momentary angular velocity ω [°/s] in anterior-posterior and medial-lateral planes close to body’s center of gravity with a sampling frequency of 80 Hz. The sign +/- indicates the direction in both planes. For the further calculations the absolute values of angular velocities were calculated for each plane. In addition, there was no filter applied to the raw data. The higher the angular velocity, the lower is the postural stability. Participants wore the device with a belt on their waist. The calibration of both gyrometers was performed by placing the device on a firm ground for 20 s. During the measurements, a video- and a sound level recording system were used for matching offline angular velocity values with the actual, real-time movements. Furthermore, all incorrectly performed tasks or recordings with unintended background noise were rejected.
Statistical analysis
Data analyzing was performed with MATLAB R2014b and IBM SPSS version 23. For all four walking tasks the values were compared between the reference condition and condition cN or iN. For determining gender-related differences, a t-test for independent samples or Mann-Whitney test (depending on the data distribution) was applied. Data distribution was tested with the Kolmogorov-Smirnov test. In case of significant gender-related differences, further analyses for these data were performed in a gender-specific way. The significance level was p < 0.05 for all statistical calculations. For each comparison (R/cN and R/iN) data were recorded in separate trials as described above. Hence, measured values of reference condition were not compared more than once with another condition.
Results
For a better presentation of the observed effects, the differences between condition R and cN or iN were given in percentage by determining the mean value of condition R as 100 %.
Gender-specific analysis
For walking over barriers (medial-lateral direction) and presented interrupted noise the recorded changes in body sway velocity differed significantly between female and male participants. The difference between condition R and iN for this task for females was on average –0.04 [°/s] and for males –1.12 [°/s]. The sign (-) indicates a reduced angular velocity by presenting noise versus reference condition. Though, only the male participants showed a significant difference (p = 0.001) of –13.3 %between the reference condition and condition iN for walking over barriers (Fig. 1). In all other conditions, no gender-specific differences could be observed.
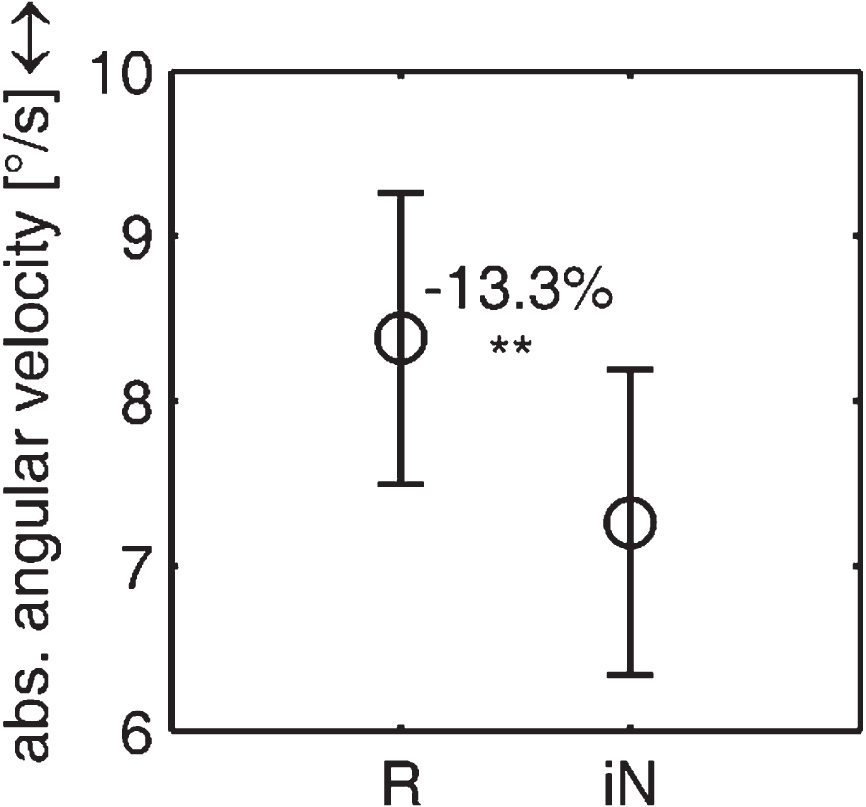
Significant change of body sway velocity (median) for walking over barriers in medial-lateral (↔) direction between reference condition (R) and presented interrupted noise (iN) for male participants. Standard deviation is additionally shown. The percentage deviation of body sway velocity of condition iN from condition R was calculated by determining the mean value of condition R as 100 %.
The results for all walking tasks and sound conditions (R-cN/R-iN) are summarized for all participants in Table 1.
Mean absolute angular velocity values [°/s] and the standard deviations (italic) of all participants are shown for all tasks. Arrows indicate medial-lateral (↔) and anterior-posterior (↕) direction. The reference condition (R) was compared with presented continuous (cN) or interrupted (iN) noise. A t-test for dependent samples or Wilcoxon test was applied
Mean absolute angular velocity values [°/s] and the standard deviations (italic) of all participants are shown for all tasks. Arrows indicate medial-lateral (↔) and anterior-posterior (↕) direction. The reference condition (R) was compared with presented continuous (cN) or interrupted (iN) noise. A t-test for dependent samples or Wilcoxon test was applied
Significant differences are highlighted with * (p < 0.05).
A comparison of condition cN/iN with the corresponding reference values showed on average a decreased angular velocity for walking with eyes open, tandem steps and walking over barriers. A significantly reduced body sway velocity could be observed for walking with eyes open (medial-lateral direction) (–7.8 %, p = 0.036) and tandem steps (anterior-posterior direction) (–8.8 %, p = 0.029) when continuous noise was presented compared to silence (Fig. 2a and b). For walking with turning the head in rhythm, the angular velocity did not change significantly, but there is a trend recognizable that the angular velocity increased with presenting noise vs. the reference condition.
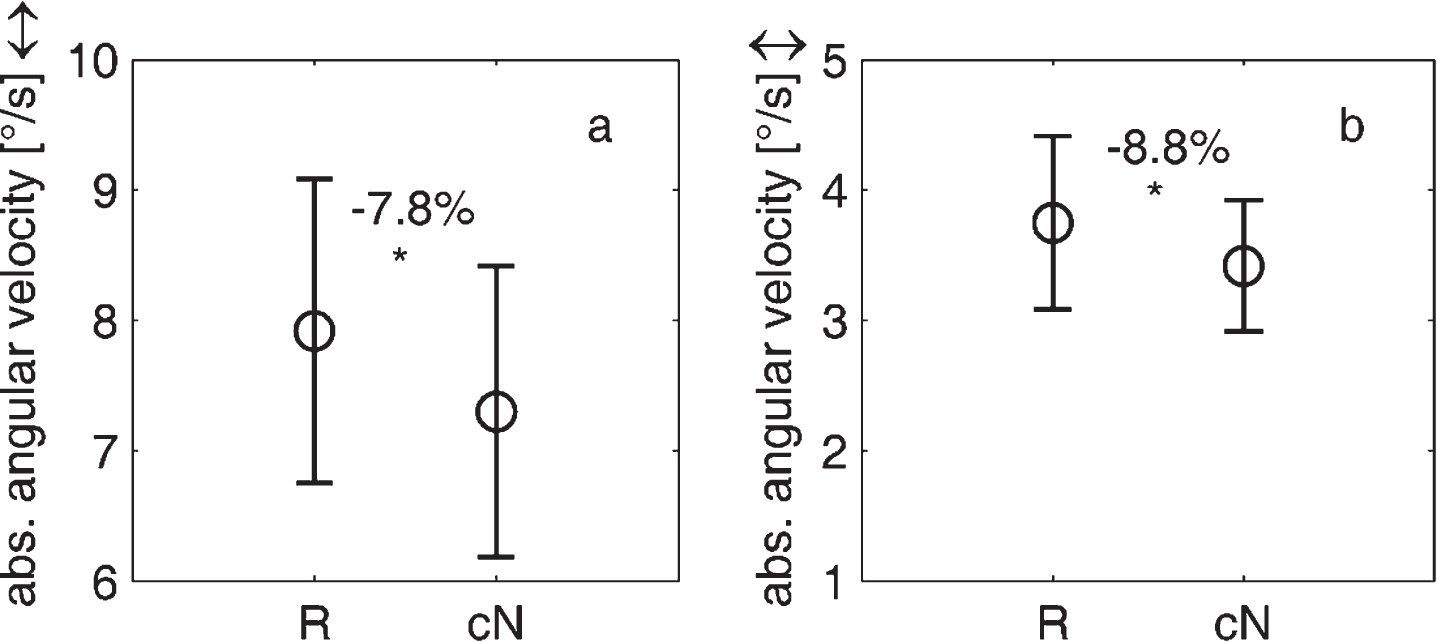
Significant changes of body sway velocity (median) for walking with eyes open (a) and tandem steps (b) in medial-lateral direction (↔) and anterior-posterior direction (↕) between reference condition (R) and presented continuous noise (cN). Standard deviation is additionally shown. The percentage deviation of body sway velocity of condition cN from condition R was calculated by determining the mean value of condition R as 100 %.
A changed auditory input could influence the postural control when noise was presented from a point sound source in front compared to silence. Postural stability was improved for walking tasks with the head focused to the front in noise condition compared to silence. This was not true for walking with moving the head to the right and left in rhythm. In a few studies before, a reduced body sway for standing tasks could be observed when sound was presented vs. silence [6, 27]. These research groups recorded body sway with a force platform or a head video system. They presented speech signals or broadband noise from 1, 2 or 4 fixed loudspeakers. Furthermore, hearing device users performed better during walking when hearing aids were turned on vs. off [20, 25]. Weaver et al. [25] have used inertial sensors to measure gait velocity, step length and sway time variability, among others. They presented broadband noise with additional natural rainfall sound from a fixed loudspeaker at the end of the walkway. In total, 13 hearing aid and 12 cochlear implant users participated. The group analysis did not show a significant improvement between hearing devices turned on vs. off, but when looking at individual data some patients showed an improved postural stability with hearing devices turned on. In Shayman et al. [20] study, three hearing impaired patients bilaterally treated with hearing aids or cochlear implants were included. Gait velocity and step length were recorded with pressure sensors inbuilt in the walkway. In aided condition, three treadmill machines parallel to the walkway provided background noise. Patients walked with closed eyes. The results showed improvement in gait performance in hearing devices on (vs. off) condition in all patients, but the effect was individually very different. However, there are only a few investigations for walking conditions and the measurement method in literature varies widely from the method in the present study. In addition, the information processing while walking is more complex than while standing. Therefore, our data are hardly comparable with the results from other, previous studies.
The gender-specific analysis showed just in one case a significant difference between female and male participants. Body sway was reduced when interrupted noise was presented during walking over barriers in roll direction compared to the reference condition. On average, men were taller than the female participants. Thus, for male participants walking over barriers was less difficult whereas this task was more demanding for female participants. Our results confirmed this assumption as males swayed significantly less in medial-lateral direction compared to female participants in the reference condition (no auditory information). Therefore, an improvement of the postural stability was possible for male participants only.
Body sway velocity was reduced independently of the type of stationary noise in our study. It is most likely that this is based on the fact that the participants localized the sound source during walking towards the loudspeaker. Zhong and Yost [27] observed a similar effect when participants performed the Fukuda Stepping test with eyes closed in silence and in noise presented from the front. The angular deviation of the feet from the midline after stepping was significantly smaller when noise was presented compared to silence. It is assumed that participants performed better because they localized the point sound source. This assumption is also supported by a study from Karim et al. [16]. Participants showed in the Fukuda Unterberger test a significant smaller angular deviation from midline, when noise was played through a fixed loudspeaker compared to silence or noise played through headphones. Neurophysiological connections between the auditory and vestibular system, as described above, additionally support these findings [1, 5].
Furthermore, walking with head turning to the right and to the left showed no significant changes in body sway velocity when changing the auditory input. There is only a trend for this task to see body sway velocity increased with presenting noise vs. silence. One reason might be impaired localization ability during moving the head in rhythm to the right and left in combination with walking forward and in addition the long reverberation time. Thus, the information from the static sound source might not be used to significantly increase postural control. Furthermore, walking with turning the head is more difficult to perform from a motoric and cognitive point of view than the other tasks as participants had to move their head in horizontal plane and legs ahead at the same time. Thus, for this task visual, vestibular and proprioceptive inputs had a larger impact on postural stability.
Another feature influencing the performance might be the effects of multi-tasking. Participants automatically regulated postural stability while walking and listened to the stimulus at the same time. In one task, walking with turning head, participants performed two additional tasks when a stimulus was presented. Different studies found a positive correlation between the difficulty of the secondary task and the maintenance of postural control [10, 23]. As listening to noise while walking is a considerable easy cognitive task, the combination of both did not have a negative impact on the improvement of postural stability. For walking with head turning, an increased body sway velocity was observed since this multi-task condition induced a higher cognitive load.
All the present findings indicate that body sway in different sensorimotor gait tasks is not highly influenced by acoustic information in young healthy people. However, the localization ability of auditory signals could improve postural control during walking.