
Abstract
BACKGROUND:
Patients with vestibular impairment often suffer from postural instability. This could be compensated by other sensory systems such as the auditory system.
OBJECTIVE:
The aim of this study was to investigate whether auditory input improves postural stability in patients with abnormal subjective haptic vertical (SHV).
METHODS:
Participants (n = 13) with normal hearing and vision, but abnormal SHV participated. Participants performed standing on firm ground and foam support (eyes open/closed) and Tandem Romberg test (eyes closed) in quiet (reference), noise and with plugged ears. All tasks were conducted in a soundproofed and reverberant room. Postural stability was recorded close to the body’s center of gravity. Reference conditions were compared with a control group.
RESULTS:
In only two tasks sway increased significantly when noise was presented during challenging tasks in the soundproofed room. Sway of the reference conditions did not differ significantly between control and study group.
CONCLUSIONS:
This study shows no influence of applied auditory stimulation on posture in participants with abnormal SHV in a reverberant room, but an adverse effect on balance during difficult tasks in the soundproofed room. Noise possibly masked auditory information that was helpful in improving posture in the quiet condition. Futhermore, noise might have distracted participants from maintaining balance.
Introduction
Maintaining balance includes automatic processes and attentional requirements [32, 36]. It is influenced by multisensory inputs such as the visual system, proprioception and the vestibular organs [29]. A dysfunction of one of these sensorineural systems often causes a reduction of postural stability that increases the risk of falling [5]. Furthermore, hearing might likewise influence balance [22, 37], as the receptors of vestibular and hearing organs have the same embryonic origin and receptors from both are bathed in the same fluid [9]. In addition to these anatomical conditions, there is already evidence for neurophysiological connections between the hearing and vestibular systems [2, 8]. However, besides anatomical and neurophysiological conditions, auditory cues (e. g. interaural time and level differences) are indispensable for spatial orientation and localization [6, 26]. The auditory input and thus the localization ability is influenced by the room properties (e.g. reverberation time), the position of the sound source(s)/listener and the characteristics of the stimulus being presented [14, 24].
To our knowledge, few research groups have analyzed the relationship between auditory cues and balance in vestibular impaired humans [15, 33]. These researchers used different acoustic conditions and measured postural stability mainly with a force platform. Stevens et al. [31] recruited balance impaired patients from a neurologic clinic and subjects with no balance impairments. All six patients had uncompensated, vestibular vertigo, but the cause of the vertigo varied among the patients. Postural stability increased in sound-on condition compared to sound-off condition in subjects with more imbalance. In the study of Vitkovic et al. [33] vestibular impaired patients performed a range of standing tasks in different acoustic environments. Most patients suffered from a unilateral vestibular dysfunction. Postural stability was improved in the sound condition vs. no-sound condition. However, the results indicate a small effect of auditory information on balance. The research group of Maheu et al. [21] investigated postural stability in normal hearing, hearing-impaired and hearing-impaired patients with additional vestibular dysfunction. Only patients with additional vestibular dysfunction benfit from auditory input (hearing aids on vs. off) whereas no significant difference was observed between normal hearing and hearing-impaired patients with hearing aids turned on. Guigou et al. [15] investigated dynamic posturography in patients with bilateral vestibulopathy. Rotating sound was presented via headphones. Postural stability decreased in vestibular impaired patients with rotating sound compared to silence. In contrast, postural control in healthy participants was not impaired by rotating sound.
In healthy humans, some studies showed a positive influence of auditory input on postural or head stability [22, 37], though, in some experimental setups no influence was observed [12, 28]. Among these studies, the group of participants, room acoustics and the experimental setup varied widely. In the studies that have found a positive effect on balance, the sound conditions reduced body/head sway in stance tasks or reduced rotation/displacement of the feet in the Fukuda stepping test [22, 37]. Stevens et al. [31] investigated vestibular impaired and healthy participants. Healthy participants barely improved than the balance impaired patients in the sound-on condition. A similar observation was made by Vitkovic’s research group [33]. Balance impaired patients seems to benefit more from the sound-on condition than healthy participants whereby the improvement was small. However, Easton et al. [12], Gandemer et al. [13] and Seiwerth et al. [28] found no significant changes in postural control in healthy participants when sound was played from the front or when wearing ear protectors in a soundproofed room. Possibly, the auditory influence on posture is very sensitive to room acoustic (anechoic versus reverberant), stimulus (static versus dynamic, noise versus speech), number and location of sound sources. The physical and mental condition of the participant and the body sway recording system also have an influence.
In the present study, participants had abnormal subjective haptic vertical (SHV). The SHV access the internal representation of the direction of gravity [27]. The perceived direction of gravity is important because of the use of gravity as a reference for almost all aspects of perception and movements. Perceived orientation is fundamental for balance and orienting oneself in the environment. A lack in the accuracy of the SHV could be related to a peripheral (e. g. utricular) or central dysfunction. Compensated utricular disorders are common in the younger population. Due to their biomechanical structure, the otolith organs (utriculus, sacculus) are affected both earlier and more frequently from dysfunction than the semicircular canals. Isolated disorders of the otolith organ account for about one third of the otogenic vestibular disorders [11]. An otolith dysfunction is often caused by head trauma (mild to severe) but also by a late stage in Meniere’s disease, aging or blast trauma [20, 34]. The otoconia overlie the hair cells and could dislocate by an acute injury such as head trauma. People with otolith disorders compensate the diminished input by using other sensory systems such as vision or proprioception.
Due to the mentioned anatomical, physiological and neurological conditions of the hearing and vestibular systems, and the described studies, we assume that patients with an abnormal SHV possibly compensate the vestibular deficit by using auditory information. This could be important if this input is masked or absent (as known from the proprioceptive and visual input).
Materials and methods
Ethical approval
The Institutional Review Board (University of Berlin) approved the study protocol (approval number EA1/326/15). All experiments were carried out in accordance with the Declaration of Helsinki and all participants agreed to the informed consent.
Subjects
Hearing thresholds of study participants
Hearing thresholds of study participants
In the present study seven females and six males participated (mean age = 28.2 years, range = 21-36 years). All participants were confirmed to have normal hearing thresholds, measured with pure tone audiometry at 0.25, 0.5, 1, 2, 4, 6 and 8 kHz [18] (0.1 percentile) (Table 1) and normal or corrected visual acuity of at least 0.7 (tested with Landolt rings). Furthermore, function of the otolith organs and of the semicircular canals was investigated. Utricular and saccular functions were examined by SHV testing, using a SHV-board (Zeisberg GmbH, Reutlingen, Germany) and by recording the cervical vestibular evoked myogenic potentials, using an ECLIPSE measurement system (Interacoustics, Denmark). An abnormal SHV-result was indicated if the difference between the lines drawn when in the±20° positions was more than 5° (more information in Schuler et al. [27]). For all participants, an abnormal SHV-result was confirmed (mean difference between±20° positions = 13.3°, standard deviation = 3.5°) whereas saccular function was found to be normal (positive cervical vestibular evoked myogenic potentials testing with an asymmetry ratio below 0.3). The etiology of this abnormal SHV-result was unknown for all participants. The semicircular canal function of all canals, tested with the EyeSeeCam® video head impulse test system (Interacoustics, Denmark), was without pathological findings (gain > 0.8 for horizontal and > 0.6 for vertical canals). The vestibular results of the participants are shown in Table 2. Postural control in a battery of stance and gait tasks was analyzed with the standard balance deficit test [4, 30]. Two participants showed a pathologic result for the entire test battery. Stance tasks within the test battery were pathological for a further two participants. In addition, subjective dizziness was assessed by the Dizziness Handicap Inventory questionnaire [19]. The Dizziness Handicap Inventory score was below or equal 30, confirming either no or a minor handicap [35]. Exclusion criteria from this study were an acute or chronic cardiovascular disease, neurological diseases (e.g. depression, anxiety, addiction, stroke, ataxia), an orthopedic malposition of the feet and any medication which influenced postural stability (e.g. sedating drugs). In total, 61 volunteers were screened to identify 13 participants with an abnormal SHV-result. 30 of 61 volunteers were included in the healthy group and 18 volunteers did not meet the inclusion criteria.
Vestibular results of study participants
A control group of 30 healthy participants with normal hearing, vision and vestibular function was compared with this group of subjects. The results of the healthy participant group were already published in Anton et al. [1]. All participants underwent the same clinical tests as the participants in this study. Eighteen female and twelve male subjects aged between 16 and 38 years (mean = 25 years) participated. The inclusion and exclusion criteria were the same but the SHV-results confirmed normal utricular function (mean difference between±20° positions = 1.6°, standard deviation = 1.4°). This result differed significantly from the result of participants with an abnormal SHV-result (Mann-Whitney test, p = 0.000).
During the preliminary examinations for the recruitment of the healthy participants, some volunteers showed an abnormal SHV. Therefore, we decided to investigate this group as well to learn more about the influence of audiotory cues in participants with vestibular impairement. All volunteers were recruited randomly by worth of mouth.
The experiments took place in two rooms with different reverberation times. One room (LR) demonstrated a very long reverberation time (T30 (125-8000 Hz)=2.46-1.05 s) (reverberant room) and the other room (SR) a very short reverberation time (T30 (125-8000 Hz)=0.32-0.16 s) (soundproofed room). The extrem different room acoustic properties could provide information to the study question. A specialist determined the reverberation times using the integrated impulse response method [17] by measurements at several points for both rooms. The reverberation time was the same at all measurement points of the room. The ambient noise level was monitored with a calibrated sound level system and recorded in both rooms < 40 dB SPL. A server room close to the hallway was the source of a constant low-frequency ambient noise. Additionally, the light conditions were kept as constant as possible for each participant by applying artificial light and darkening all windows.
Procedure and setup
All participants performed five standing tasks under different acoustic conditions in both rooms. The tasks included: standing on a firm ground with eyes open/closed; standing on a foam support with eyes open/closed; Tandem Romberg test with crossed arms, heel-to-toe position and eyes closed.
For the tasks standing on a firm ground/foam support, the arms hung relaxed and the distance between the two feet corresponded to the width of participant’s fist (width of fist from forefinger to little finger). The distance between the feet was marked and the feet were parallel to each other. Participants wore similar disposable socks to avoid any influence on sway measurements by different personal shoes. They also wore similar, comfortable, soft pants to ensure a free movement during performing the tasks. During testing, all participants wore a belt with a device consisting of two gyrometers, positioned close to body’s center of gravity (VertiGuard® system, Zeisberg GmbH, Reutlingen, Germany). The gyrometers were orthogonal to each other. Momentary angular velocity ω [°/s] of trunk movements was recorded in anterior-posterior and medial-lateral directions with a sampling rate of 80 Hz. Both gyrometers were calibrated before and during each session by placing the device on a solid surface for 20 s. In addition, the drift velocity caused by the temperature was compensated by a self-calibration algorithm. The drift of both gyrometers is 0.007 °/s. A low angular velocity means less body sway and thus a higher postural control.
Each task was performed in quiet in each room as reference condition (R), with a loudspeaker in front presenting continuous white noise (cN) or interrupted white noise (iN) and with wearing earplugs (Howard Leight Max) and additionally circumaural ear protectors (Moldex M1) (EP). Both noise stimuli consisted of white broadband noise (80 Hz-20 kHz). In the iN condition, stimulus and pause alternated with the same duration of 0.5 s for a one second repeat rate. This interruption rate was chosen to ensure that the reverberation in the rooms was not masked and could therefore, be perceived by the participant whereas the continuous noise possibly masks useful auditory information. A single loudspeaker (JBL Control One, frequency range 80 Hz - 20 kHz (±3 dB)) presenting the noise stood 2 m in front of the participant in the room LR and 1 m in front in the room SR. This difference was due to the different room sizes. The sound pressure level was 60 dB SPL at participant’s position in both rooms. Thus, a direct stimulation of the utricular function is very unlikely due to the low presentation level.
All standing tasks were recorded for 20 s. To avoid the measurement of higher body sway velocity caused by turning on and off the loudspeaker, the first and the last second were not included in the analysis. The order of standing tasks, the acoustic conditions as well as the room test order were randomized by using MATLAB R2014b. All test sessions were monitored using a video and audio recording system for an offline analysis. Incorrectly performed tasks or test sessions with unwanted background noise were removed from further analysis. All participants received the same instruction.
Statistical analysis
For the statistical comparison of the reference condition with one of the other acoustic conditions, the individual velocities for each of the two sway directions (anterior-posterior/medial-lateral) were determined. Then, for each test condition, the median of the angular velocities was calculated. The reference condition always relates to the measurement in silence in the room SR or LR. Extreme values (more than 1.5 times smaller or greater than the interquartile range) were not included in the statistical analysis. Overall, 3.29% of the data were categorized as extremes. Significant differences between female and male were tested applying Mann-Whitney U-test and significant differences between the reference condition and condition cN, iN or EP were tested by Wilcoxon’s test. Mann-Whitney U-test was used to compare the reference conditions for the test group and control group (with normal SHV-result). The Bonferroni method was applied for correction of the p value within multiple comparisons of the sound conditions, and both groups of subjects. No more than four comparisons were made for each reference condition. Therefore, a significance level of p < 0.0125 was chosen for all statistical calculations. For the data analysis MATLAB R2014b and IBM SPSS version 23 were used. Since the angular velocities were very small, the significant differences between two sound conditions were expressed in percent. The mean value of condition R was normalized to 100%.
Results
Comparison between healthy participants and participants with an abnormal utricular function
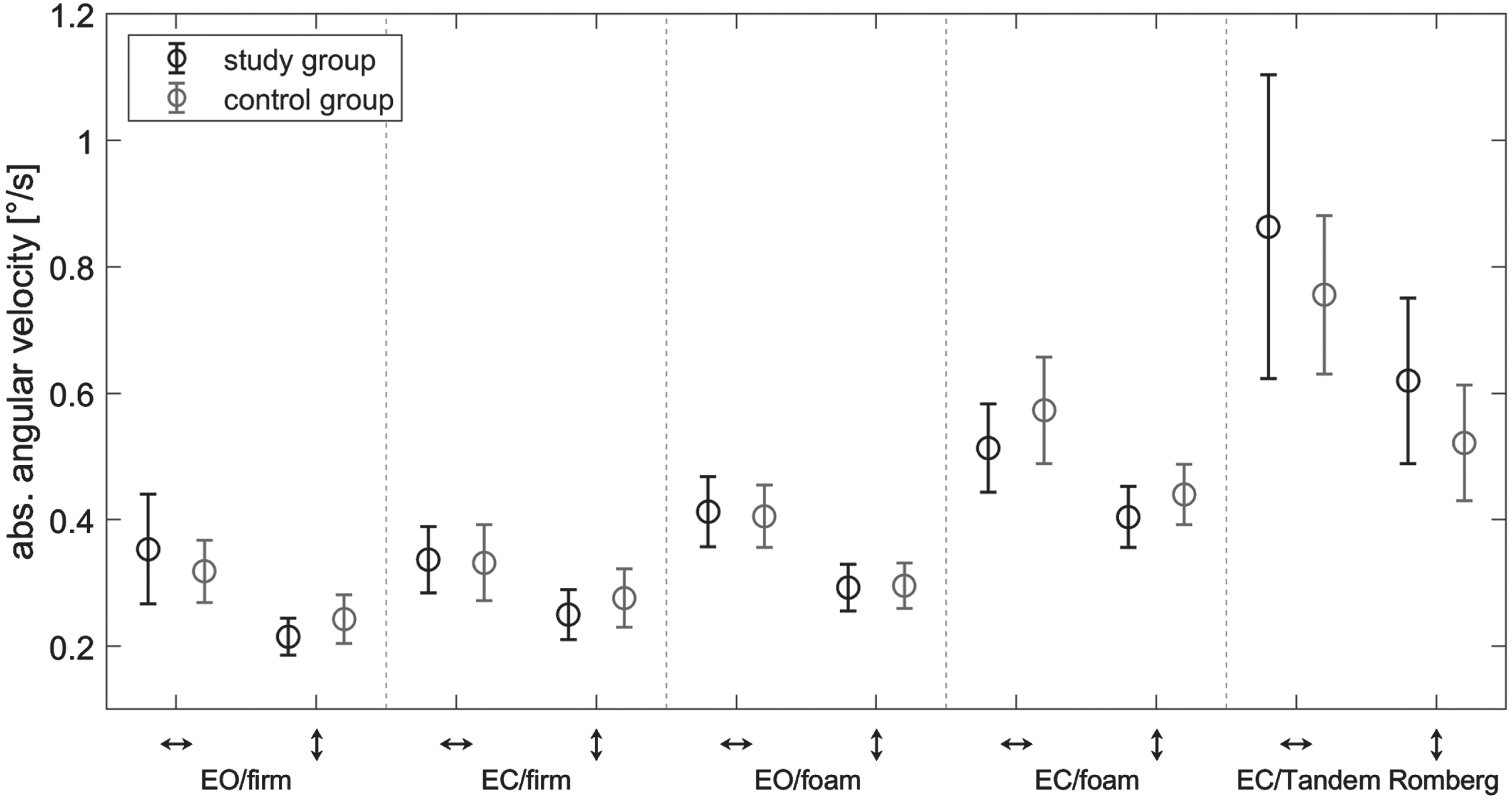
Exactly the same experimental setup used for the study group was used earlier for the control group (30 participants with normal hearing, vision and vestibular function). These data are already published in Anton et al. [1]. Therefore, the reference conditions of all stance tasks in both rooms were statistically compared for both groups for an exploratory investigation only. No significant differences were observed for the reference conditions between the study and control group. Figures 1 and 2 show the mean angular velocities of the study and control group of all tasks in room SR and LR.

Mean absolute angular velocities and standard deviations for the reference condition of the study (black) and control group (grey) in the room with a short reverberation time. Data are shown for the standing tasks: Eyes open (EO) and closed (EC) on firm ground and foam support and Tandem Romberg test in anterior-posterior (↕) and medial-lateral (↔) direction.
Mean absolute angular velocities and standard deviations for the reference condition of the study (black) and control group (grey) in the room with a long reverberation time. Data are shown for the standing tasks: Eyes open (EO) and closed (EC) on firm ground and foam support and Tandem Romberg test in anterior-posterior (↕) and medial-lateral (↔) direction.
Mean of total angular velocity values and standard deviations of the tasks conducted in the room SR are shown in Table 3.
Mean of total angular velocity values [°/s] and standard deviations (italic) of participants with abnormal subjective haptic vertical in the soundproofed room. The reference condition (R) was compared with presented continuous (cN) or interrupted (iN) noise or ear protectors (EP) in medial-lateral (↔) and anterior-posterior direction (↕)
Mean of total angular velocity values [°/s] and standard deviations (italic) of participants with abnormal subjective haptic vertical in the soundproofed room. The reference condition (R) was compared with presented continuous (cN) or interrupted (iN) noise or ear protectors (EP) in medial-lateral (↔) and anterior-posterior direction (↕)
Significant differences are highlighted with ** (0.001≤p < 0.01).
Significantly higher sway velocities were observed for two stance tasks for the noise conditions compared to condition R for the study group (shown in Fig. 3). Standing on a foam support with eyes closed (anterior-posterior direction) and Tandem Romberg test (medial-lateral direction) showed significantly increased sway velocities for condition cN or iN (p = 0.008, 14.8% increase, effect size = 2.49; p = 0.009, 31.8% increase, effect size = 1.08) (shown in Fig. 3a and 3b). For the rather easier tasks (standing on a firm ground) or condition EP there was no significant effect observed in the soundproofed room.

Significant changes of angular velocities in soundproofed room. Medians and standard deviations (black = study group, grey = control group) are shown for standing on a foam support with eyes closed (anterior-posterior direction) (A) and Tandem Romberg test (medial-lateral direction) (B) between reference condition (R) and condition where continuous (cN) or interrupted white noise (iN) was presented. The percentage deviations of angular velocity of conditions iN and cN from condition R were calculated by normalizing the mean value for condition R to 100%.
Table 4 illustrates the mean of total angular velocity values and standard deviations of the tasks undertaken in the room with a long reverberation time.
Mean of total angular velocity values [°/s] and standard deviations (italic) of participants with abnormal subjective haptic vertical in the reverberant room. The reference condition (R) was compared with presented continuous (cN) or interrupted (iN) noise or ear protectors (EP) in medial-lateral (↔) and anterior-posterior direction (↕)
Mean of total angular velocity values [°/s] and standard deviations (italic) of participants with abnormal subjective haptic vertical in the reverberant room. The reference condition (R) was compared with presented continuous (cN) or interrupted (iN) noise or ear protectors (EP) in medial-lateral (↔) and anterior-posterior direction (↕)
No significant results.
The analysis showed no significant differences between the reference condition and any of the acoustic conditions in the reverberant room. There was almost no difference between the reference and noise/ear protector conditions for standing on firm ground.
In summary, for participants with an abnormal SHV, moderate white noise presented from a fixed sound source seems to have an adverse effect on postural stability for challenging stance conditions (standing on a foam support, Tandem Romberg test) in the soundproofed room. This holds true as in two out of 30 tested conditions in the soundproofed room where significance was reached. No differences in sway velocity could be seen between the study and control group for the reference conditions.
It seems that the auditory information, which might help to compensate for the impaired peripheral receptor function, was masked by the applied moderate white noise in the soundproofed room. Here helpful reflections of the remaining background noise should be fast and not overlaid in time. A long reverberation time might partly affect detection accuracy of the reflections and thus impair spatial orientation. Surprisingly, postural control did not change significantly when participants wore ear protectors. Sway increased in healthy young or elderly people when their ears were plugged [1, 3]. This supports the conclusion that the participants investigated in the present study had no great benefit from auditory cues such as reflections at all. Guigou et al. [15] observed a similar effect: Vestibular impaired patients had greater sway when listening to rotating sound through headphones. These patients had no access to reflections which might have helped. Possibly, patients with vestibular disorders are distracted by additional sound when they spend their attention on maintaining balance, especially for more difficult tasks. Many cognitive processes are essential for stabilizing posture [32, 36]. The cognitive load in patients with vestibular impairement might be higher for the same tasks than for healthy participants. In Guigou et al. [15] and in the present study the attentional focus or cognitive load was not investigated. An effect of attentional focus on posture (improvement or impairment) was observed by Bonnet [7].
Since the similar tasks were performed in both rooms and an increased sway was only observed during noise application in the soundproofed room, the masking and the attention effect should contribute to the observed results.
The present results from participants with an abnormal SHV are opposite to some findings in patients with other vestibular deficits. Stevens et al. [31] demonstrated an improved postural stability for a noise condition compared to silence in six balance impaired patients. These patients showed different causes of imbalance and where applicable hearing aids were used. The baseline for body sway was higher compared to the healthy participants in Steven’s study. Noise was presented from four loudspeakers placed close to the patient’s head. Compared with the present study, noise was delivered from four loudspeakers instead of one loudspeaker in front. Additionally, the loudspeakers were placed much closer to the participant’s head. Hence, small head movements caused higher interaural time and level differences in Stevens’ experimental setup [31] compared to our setup. This kind of auditory feedback [5] could have helped balance impaired patients to improve postural control in the noise condition compared to silence. In addition, the patients in Stevens’ study [31] suffered from different vestibular diseases whereas all participants in the present study only had a history of abnormal utricular function. Furthermore, different measurement systems were used to determine postural stability. The ankle referenced platform system calculates positional changes of the center of gravity by anthropometric models [10] whereas the measurements in the present study were performed with a sensor close to the center of gravity. Vitkovic et al. [33] observed, also in vestibular impaired patients, an increased postural stability in stationary or moving white noise conditions compared to silence. These patients had different causes of vertigo and different degrees of hearing loss. In their setup noise was presented from either a single loudspeaker in front, or from an eight-loudspeaker frontal semicircular array, with a distance of 106 cm to the participant and at a comfortable sound level. The vestibular impaired patients showed a benefit from added sound. In Vitkovic’s study [33] and in the present study the groups of patients showed different vestibular and hearing conditions. Therefore, one reason for the inhomogeneous results might be the different pathophysiological conditions.
In essence, the present results show an adverse influence of auditory stimulation on postural control during very limited tasks and conditions in participants with abnormal SHV. This holds especially true for tasks with a reduced visual or proprioceptive input. This could be related to the increased attentional focus for maintaining posture during the more complicated tasks in combination with the more effective masking of residual helpful auditory information by the applied noise in the soundproofed room. In contrast to young or elderly healthy volunteers investigated earlier [1, 3], no helpful effect of any auditory input was detected. Future studies should investigate the properties of auditory signals that are helpful for the vestibular compensation in vestibular disorders. Further studies should also focus on cognitive processings during maintaining balance in vestibular impaired patients. This was not determined in the present study but might have had an impact on the postural stability. Another limitation is the low number of participants. However, a calculation of the minimum number of participants resulted in 5 or 14 participants (calculated for standing on a foam support with eyes closed in anterior-posterior direction or Tandem Romberg test in medial-lateral direction in room SR). Nevertheless, a larger number should still be investigated to confirm the results. In addition, the age range of participants was limited to a younger population. Other results could be expected in elderly patients. Furthermore, it would be interesting to apply different stimuli and background noises such as speech or informational masking noise compared to energetic masking noise. This could offer further knowledge about the integration of vestibular and auditory information in normal daily life situations.