
Abstract
OBJECTIVE:
The aim of the present study was to investigate the factors influencing semicircular canal function as evaluated by video Head Impulse Test (vHIT) in patients with vestibular schwannoma.
METHODS:
Twenty-four patients with untreated vestibular schwannoma underwent vHIT examination. The correlations between semicircular canal function and factors including age, tumor size, disease duration and hearing loss were evaluated.
RESULTS:
The functions of all three semicircular canals on the affected side evaluated by vHIT were significantly lower than those on the unaffected side. Although there were no significant correlations between semicircular canal function and age, tumor size or disease duration, a negative significant correlation between vestibulo-ocular reflex (VOR) gain as evaluated by vHIT and hearing loss was observed.
CONCLUSIONS:
From the results of the relationship between hearing loss and VOR gain, the damage to the audio and vestibular systems in patients with VS may be correlated. As it has been suggested that tumor size was not a significant factor in the VOR gain evaluated by vHIT, multifactorial causes rather than the simple compression of the vestibular nerves alone may be related to the dysfunction of the semicircular canals in patients with vestibular schwannoma.
Keywords
Introduction
Vestibular schwannoma (VS) is a benign tumor of the vestibular nerve that transmits balance information from the inner ear to the brain, and is a commonly observed tumor of the cerebello-pontine angle (CPA). The most frequent symptoms of VS are unilateral hearing loss, tinnitus and disequilibrium, with vertigo reported as the most debilitating symptom with respect to health-related quality of life [14].
Recently, the video Head Impulse Test (vHIT) has been reported as the examination of choice for the evaluation of semicircular canal function [25]. vHIT is a non-invasive testing method that can evaluate the function of all semicircular canals including the vertical canals as accurately as scleral search coils [10], and we have reported the evaluation of vertical semicircular canal function by using vHIT in patients with VS [5]. Correlations between vestibular test findings, such as the caloric test or vestibular evoked myogenic potentials (VEMP), and various factors including tumor size or location and hearing loss in patients with VS have been investigated [1, 28]. However, there are few studies on the correlations between the results of vHIT and the above-mentioned factors [3, 21]. The vertical semicircular canal function in patients with VS, in particular, was discussed in only one report [19]. Based on the previous studies, the existence of a significant correlation between vestibular test findings and tumor size still remains controversial. Moreover, the findings of VEMP and caloric testing could not predict the nerve of origin in patients with VS [18]. On the other hand, many studies have reported that there is no significant correlation between hearing loss and tumor size in patients with VS [15, 23]. In this retrospective study, we investigated the correlation between semicircular canal function, including the vertical canals, as evaluated by vHIT and factors such as age, tumor size, disease duration and hearing loss in patients with VS.
Materials and methods
Patients
We retrospectively reviewed the medical records of patients with VS treated in the Department of Otolaryngology at Hokkaido University Hospital. Patients with VS who received vHIT were included in this study. Diagnosis of VS was based on MRI findings. Patients who had received any type of treatment for VS, including surgery and radiotherapy, before examination were excluded and only the vestibular test results obtained before treatment are dealt with in this study. Moreover, the patients for whom vHIT was contraindicated due to severe structural neck problems were excluded in this study. Patients with a history of definitive inner ear disease, such as Meniere’s disease, familial hearing loss, chronic noise exposure, ototoxic drug intake, head trauma, and inner ear malformation were also excluded.
Patients underwent a thorough history-taking, physical examination, and audiological examinations including pure-tone audiometry, speech audiometry and equilibrium examinations including spontaneous nystagmus test, positional nystagmus test and head-shaking nystagmus test. Disease duration was defined as the duration from the onset of symptoms such as hearing loss or dizziness to vHIT examination.
This research adhered to the tenets of the Declaration of Helsinki and was approved by our institutional review board (No. 018-0001). Informed consent was obtained from all individual participants included in the study.
Imaging
All patients for whom CPA MRI scans were available were analyzed for tumor size. Computed tomography scans were used to measure tumor size in one patient with a cardiac pacemaker. All examinations were performed on 1.5 or 3.0 Tesla scanners. The imaging protocol consisted of axial T1 and T2 whole head images and CPA MR cisternography. Tumor size, defined as the maximum diameter in the axial plane, was measured by examiners who were not involved in the vestibular examinations including the vHIT. Based on the radiological evaluation, patients were classified according to Koos grading [7]: Grade I = small intracanalicular tumor, Grade II = small tumor with protrusion into the CPA but no contact with the brainstem, Grade III = tumor occupying the cerebellopontine cistern with no brainstem displacement, and Grade IV = large tumor with brainstem and cranial nerve displacement.
Video Head Impulse Testing (vHIT)
Our method for vHIT has been described previously [5]. Briefly, semicircular canal function was evaluated using an ICS impulse 3-D video head impulse system (GN Otometrics, Taastrup, Denmark). The video camera was contained within the right eye-frame of the goggles. Googles were secured firmly to the subject’s head with an adjustable elastic strap to avoid slippage of the googles during impulse. The head of the subject was quickly turned (amplitude of 10–20°) with unpredictable timing and direction corresponding to the horizontal, left anterior-right posterior (LARP) and right anterior-left posterior (RALP) planes, and the vestibulo-ocular reflex (VOR) gains of the anterior semicircular canal (ASC), horizontal semicircular canal (HSC) and posterior semicircular canal (PSC) were evaluated. Eye and head velocities were sampled at 250 Hz and the VOR gain, the ratio of the area under the curves for the head and eye velocity, was calculated from the average of at least 20 head impulses. Trials with blinks and outliers were detected automatically or manually and excluded from the recording. A normal gain was defined as≥0.80 in the horizontal canal and≥0.70 in the vertical canal [12]. The catch-up saccade (CUS) was defined as abnormal in this study if the velocity of the CUS exceeded 90 deg/sec based on our previous study [5]. The correlations between VOR gains and factors such as age, tumor size, disease duration and hearing loss were investigated. Moreover, the relationship between the presence or absence of CUS and the abovementioend factors were also investigated. No severe adverse events were associated with the vHIT, apart from one case who experienced mild dizziness. All examinations were performed by the same operator.
Audiometric data
Audiometry was performed using a pure-tone audiometer (AA-76; Rion Co., Tokyo, Japan) in a silent booth by experienced audiologists. The pure-tone thresholds for each ear were determined at frequencies of 125, 250, 500, 1,000, 2,000, 4,000 and 8,000 Hz for air conduction, and at 250, 500, 1,000, 2,000 and 4,000 Hz for bone conduction, with masking as appropriate. The degree of hearing loss was evaluated from the average of the 0.5, 1, 2 and 4 kHz thresholds based on a previous report [8] and the average for the affected side was defined as the hearing level.
Statistical analysis
Statistical analyses were performed using GraphPad Prism software (version 6.0; GraphPad Software Inc.; La Jolla, CA). Statistical differences were analyzed using the paired t test, the Mann-Whitney U test, and linear regression analysis, with a p value of less than 0.05 considered statistically significant.
Results
Subject profiles
A total of 24 patients with VS were enrolled in this study and detailed subject profiles are shown in Table 1. Nine patients were male and 15 were female, with a median age of 66.5 years (range, 46 to 83 years). The VS was located on the right side in 14 and on the left side in 10 patients. The maximum tumor diameter ranged from 3.0–28.6 mm (median; 10.1 mm). Based on the Koos grading, 7, 13, 1 and 3 patients were classified as Grade I, II, III and IV, respectively. Disease duration ranged from 3–276 months (median; 72.5 months). Mean VOR gain was significantly lower toward the affected side for all three canals compared with that toward the unaffected side (affected ears: ASC = 0.79, HSC = 0.80, PSC = 0.67; unaffected ears: ASC = 0.87, HSC = 0.91, PSC = 0.77; paired t tests, p = 0.019, 0.003 and 0.009, respectively). CUSs of ASC, HSC and PSC toward the affected side were detected in 1 (4.2%), 14 (58.3%) and 12 (50.0%) cases, respectively. It is impossible to examine the results of CUS in ASC statistically as almost all patients showed no CUS in ASC. Therefore, the results for ASC were excluded from the investigation of the presence or absence of CUS.
Detailed subject profiles
Detailed subject profiles
Linear regression analysis was used to determine any potential correlation between VOR gain and age (Fig. 1A–C). No significant correlations were observed between the VOR gain of the ASC, HSC and PSC toward the affected side and age (r2 = 0.135, 0.002 and 0.047, respectively and p = 0.078, 0.85 and 0.31, respectively). Paired t test was used to investigate the relationship between the presence or absence of CUS and age. There were no significant differences in age between the patients with CUS and without CUS in HSC or PSC (p = 0.80 and 0.96, respectively).
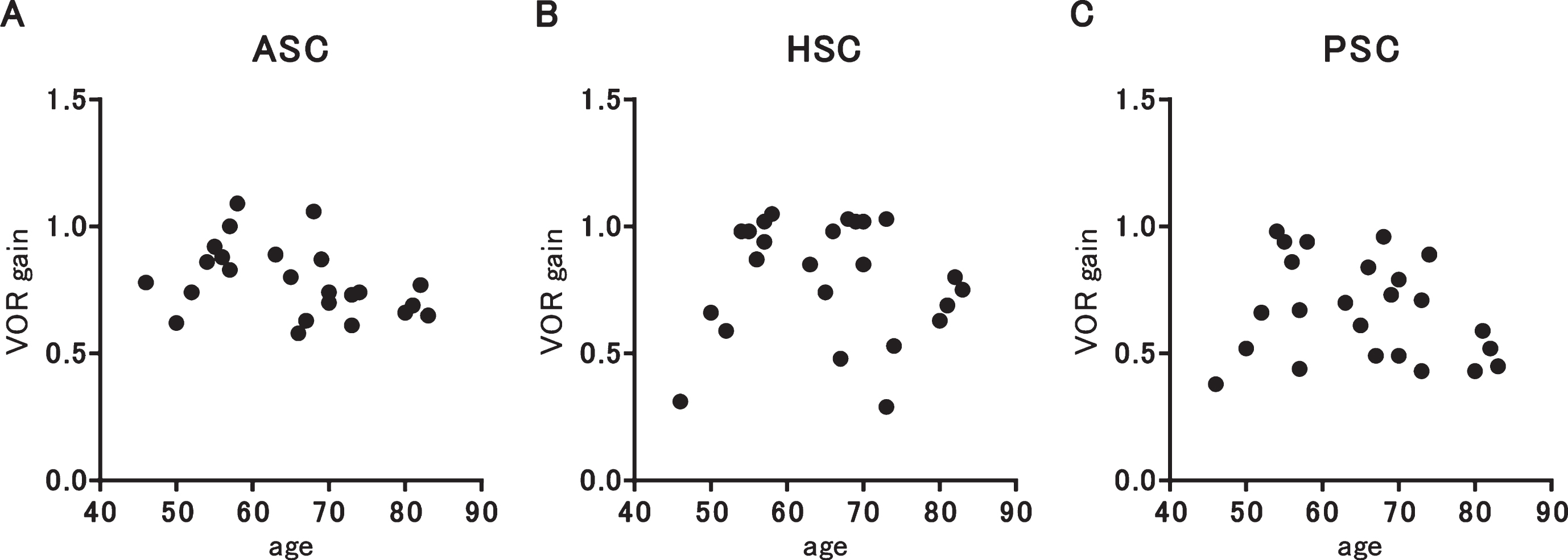
Correlation between VOR gain and age. The results for the ASC (A), HSC (B) and PSC (C) are presented. There was no significant correlation in any of the three canals.
Linear regression analysis was used to determine any potential correlation between VOR gain and tumor size (Fig. 2A–C). No significant correlations were observed between the VOR gain of the ASC, HSC and PSC toward the affected side and tumor size (r2 = 0.009, 0.095 and 0.006, respectively and p = 0.67, 0.14 and 0.73, respectively). Correlation between VOR gain and Koos grading was evaluated by Mann-Whitney U test. Patients were divided into two groups (Koos grading I or II (n = 20) and III or IV (n = 4)). There were no significant differences in the VOR gain of the ASC, HSC and PSC toward the affected side between these two groups (p = 0.91, 0.07 and 0.28, respectively). As the median of tumor size was 10.1 mm, the patients were again divided into two groups based on tumor size [smaller than 10 mm (n = 12) and greater or equal to 10 mm (n = 12)]. Again, there were no significant differences in the VOR gain of the ASC, HSC and PSC toward the affected side between the two groups (p = 0.93, 0.77 and 0.50, respectively). Paired t test was used to investigate the relationship between the presence or absence of CUS and tumor size. There were no significant differences in tumor size between the patients with CUS and without CUS in HSC or PSC (p = 0.54 and 0.17, respectively).

Correlation between VOR gain and tumor size. The results for the ASC (A), HSC (B) and PSC (C) are presented. There was no significant correlation in any of the three canals.
Correlation between VOR gain and disease duration was evaluated by linear regression analysis (Fig. 3A–C). There were no significant correlations between the VOR gain of the ASC, HSC and PSC toward the affected side and disease duration (r2 = 0.012, 0.003 and 0.020, respectively and p = 0.60, 0.79 and 0.51, respectively). Paired t test was used to investigate the relationship between the presence or absence of CUS and disease duration. There were no significant differences in disease duration between the patients with CUS and without CUS in HSC or PSC (p = 0.87 and 0.44, respectively).
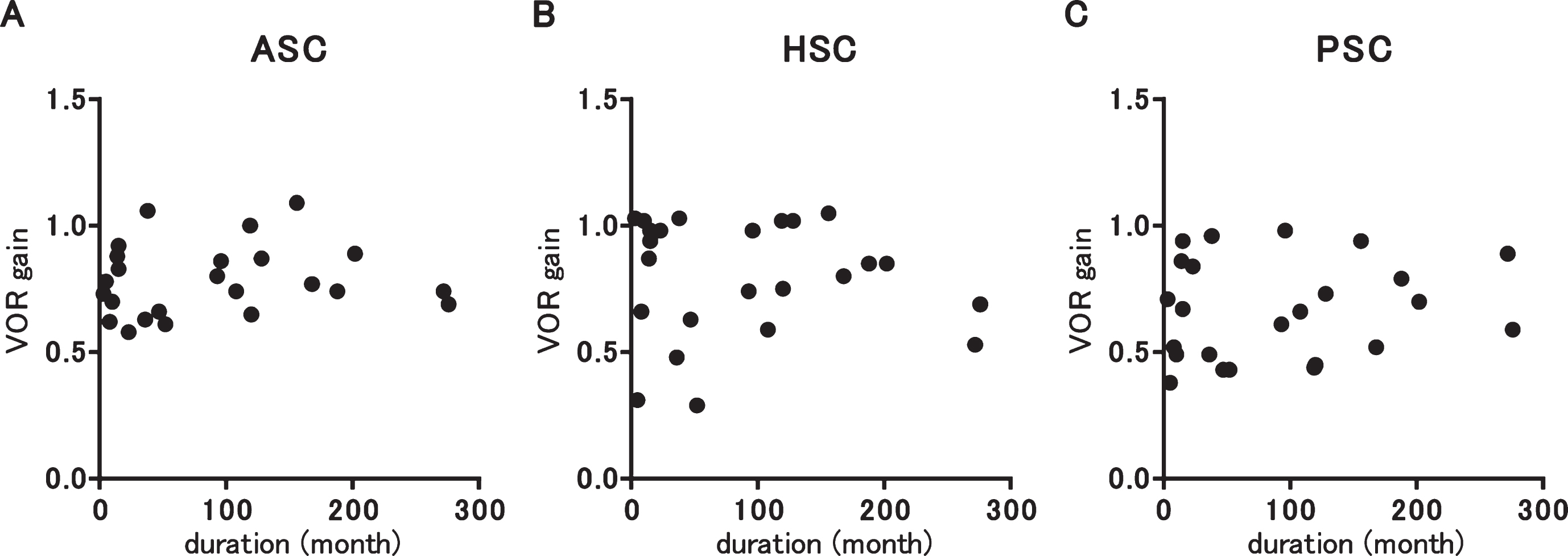
Correlation between VOR gain and disease duration. The results for the ASC (A), HSC (B) and PSC (C) are presented. There was no significant correlation in any of the three canals.
Hearing level ranged from 10.0 to 115.0 dB (median; 58.13). Correlation between VOR gain and hearing level was evaluated by linear regression analysis (Fig. 4A–C). Significant negative correlations were observed between the VOR gain of the HSC and PSC toward the affected side and hearing level (r2 = 0.079, 0.23 and 0.21, respectively and p = 0.18, 0.019 and 0.024, respectively). Paired t test was used to investigate the relationship between the presence or absence of CUS and hearing loss (Fig. 5A–B). There was a significant difference in hearing loss between the patients with CUS and without CUS in HSC; however, no significant difference was observed in PSC (p = 0.033 and 0.29, respectively).
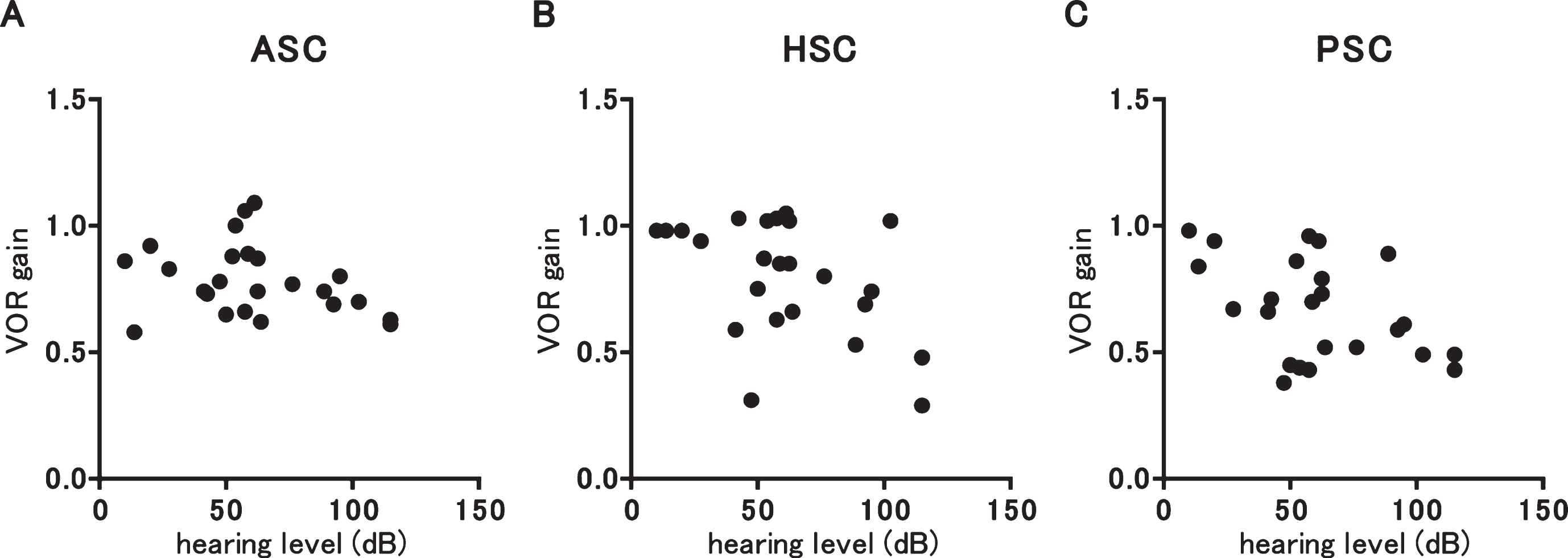
Correlation between VOR gain and hearing loss. The results for the ASC (A), HSC (B) and PSC (C) are presented. There were significant negative correlations between the VOR gain of the HSC and PSC.
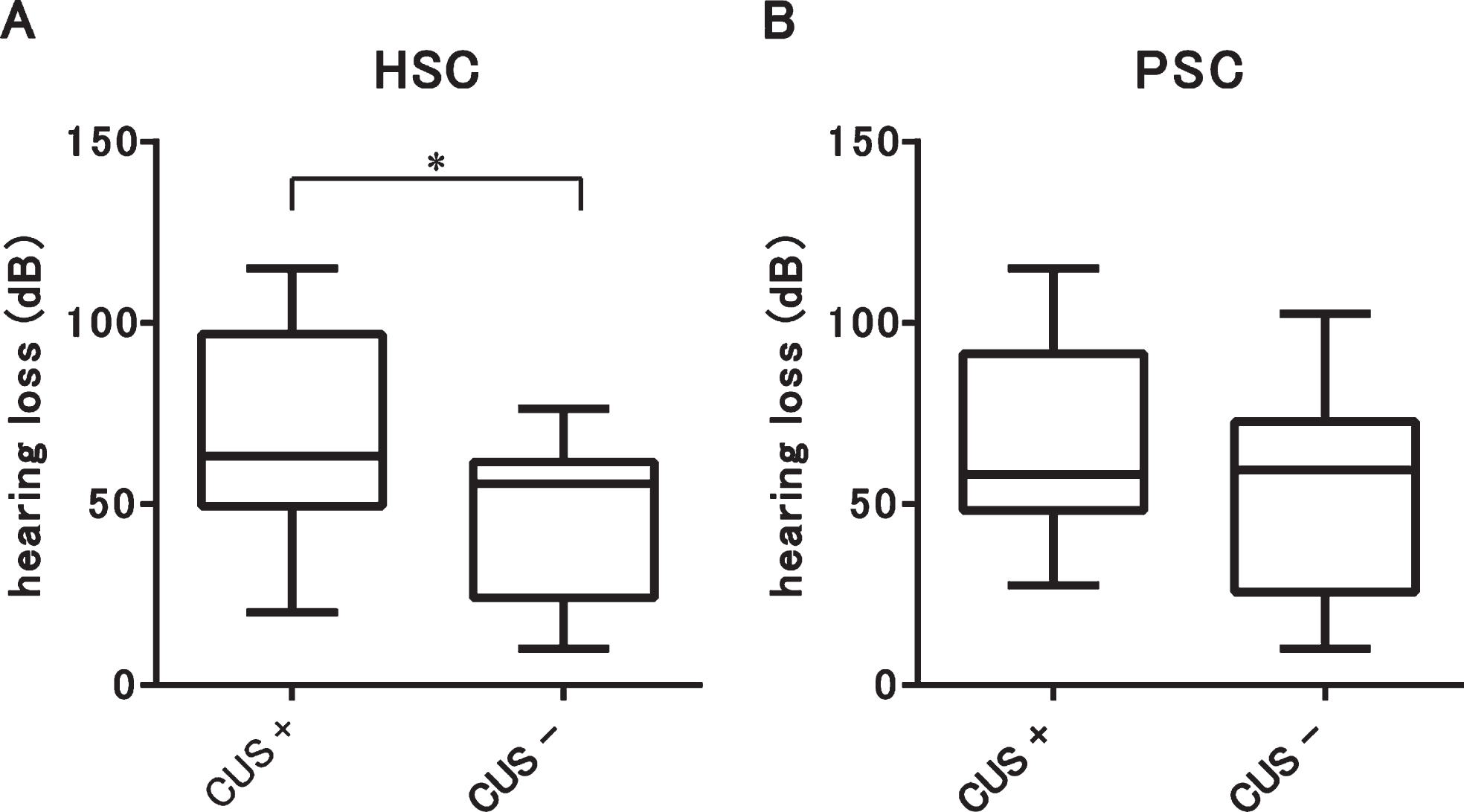
Relationship between the presence of CUS and hearing loss. The results for HSC (A) and PSC (B) are presented. There was a significant difference in hearing loss between the patients with CUS and without CUS in HSC. *p < 0.05.
In this study, we investigated the correlation between VOR gain as evaluated by vHIT and various factors including age, tumor size, disease duration and hearing loss. Significant negative correlations between VOR gain and hearing loss for HSC and PSC on the affected side were observed. Additionally, there was a significant difference in hearing loss between the patients with CUS and without CUS in HSC. These results indicate that the damage to the audio and vestibular systems in patients with VS may be correlated. A previous report demonstrated the vHIT gain of the HSC was significantly correlated with asymmetry in hearing level of the affected and unaffected sides, while vHIT gain of the ASC or PSC showed no significant correlation [19]. As there were no significant correlations between VOR gain and tumor size or disease duration, it is possible that the cause of the vestibular dysfunction in patients with VS is not the compression of the vestibular nerves by the tumor alone, but may be multifactorial. From the results obtained in this study, there were no differences between the horizontal and vertical canals in terms of the absence or presence of significant correlations with the various factors. Our previous results demonstrated that significant correlations were observed in the VOR gain for all pairs evaluated (i.e., ASC vs. HSC, HSC vs. PSC, and PSC vs. ASC) in patients with VS [5].
Although correlations between the VOR gain of vHIT and tumor size in patients with VS have been reported [3, 19], there were no significant correlations between the VOR gains in the three semicircular canals and tumor size in this study. One reason for this discrepancy is considered to be that the tumor sizes in our study were smaller than those in previous studies. The majority of patients (20/24) enrolled in this study were classified as Grade I or II according to Koos grading. In the study reported by Taylor et al. [19], the patients were divided by tumor size into small (≤14 mm) and medium to large (>14 mm), with 24 of the 50 patients categorized as small. Applying this classification to our study, 19 of the 24 patients would have been defined as small. The proportions of the small group in two studies thus differed significantly (p = 0.01, Fisher’s exact test). With regard to intracanalicular type, no significant difference in tumor size was observed between patients with a normal caloric response and those with canal paresis or between patients with a normal VEMP and those with an abnormal VEMP [18]. As many patients of intracanalicular type were included in this study, this may have affected the results with regard to the lack of any significant correlation between VOR gain and tumor size.
Many studies have investigated the correlations between vestibular test findings, such as caloric test or VEMP, and tumor size in patients with VS, with Wagner et al. reporting that loss of vestibular function in VS tends to be more severe in patients with large tumors [24]. It has also been reported that larger tumors are associated with a higher risk of postural instability and canal paresis [1]. Although the results of the pure-tone audiograms did not significantly predict tumor size, ocular VEMP and cervical VEMP responses remained significant predictors of tumor size [9]. Increased tumor size is not directly associated with hearing loss and only somewhat with vestibular deficit [26]. Regarding hearing loss, several reports have found no relationship between the degree of hearing loss and tumor size [15, 23]. Moreover, extension of the tumor to the IAC and the severity of the hearing loss are not correlated [15, 22]. It has been considered that nerve compression is not the only cause of hearing loss in VS [15], and the possibility that extracellular vesicles derived from VS associated with poor hearing cause damage to cochlear cells has been reported [17]. Although that study investigated damage to the cochlear cells alone, a similar mechanism may exist concerning damage to the vestibular systems. As the cause of hearing loss in patients with VS, elevation of internal auditory canal pressure has been speculated, and pressure was not found to correlate with tumor size [2]. If the damage to the vestibular nerve correlates with the internal auditory canal pressure in a similar fashion to that of the cochlear nerve, it may explain why the damage is not correlated with tumor size.
vHIT cannot distinguish between a peripheral vestibular end-organ disorder and vestibular nerve disorder as a cause of disequilibrium in patients with VS, and histopathological study is essential to detect the involved region. Histopathological data regarding the mechanism underlying the disequilibrium in patients with VS is very limited compared with the extensive knowledge about hearing loss; that is, both retrocochlear and cochlear mechanisms are associated with hearing loss in patients with VS [11, 16]. Roosli et al. reported that tumor size and distance from the cochlea did not correlate with structural changes in the cochlea or the hearing threshold [16]. In the vestibular system, the relationship between tumor size and the degree of degeneration in the vestibular nerve or end organ has not been investigated histologically. In case of a small tumor, histopathology is localized exclusively to the nerve of tumor origin and the related peripheral tissue structures, in contrast to large tumors in which global and severe degeneration of the vestibular neuroepithelia, as well as peripheral nerve atrophy and loss of Scarpa’s ganglion are observed [13]. As only one patient was treated by surgery, the relationship between the nerve origin and the results of vHIT could not be investigated in the present study. From the results of histopathological study, vHIT results may be able to predict the nerve origin, particularly in patients with a small tumor. In a previous study, it has been reported that the nerve of origin of tumors cannot be predicted based on caloric response and VEMP [18]. Further study is needed to investigate whether vHIT results can predict the nerve origin.
It is reported that a VOR gain in the horizontal impulse may be influenced by the side on which the camera is positioned; that is, the gain in the impulse toward the camera side can be higher than that toward the other side in normal subjects [6]. Although the direction of impulse had little influence on the VOR gain in the vertical impulse, VOR gain of the HSC may be influenced by whether the tumor exists on the right or left side. In this study, the VS was located on the right side in 14 and on the left side in 10 patients, and there was no significant difference of VOR gain toward the affected side between the right and left side (p = 0.21, Mann-Whitney U test). In previous studies analyzing VOR gain in normal subjects, it has been reported that VOR gain was largely unaffected by age [12, 27]. There was no significant correlation between VOR gain in patients with VS and age in the present study.
There are some limitations to this study. Due to the retrospective nature of this study, the presence of bias based on the selection criteria for patients cannot be completely ruled out. As mentioned above, the relationship between the nerve origin and the results of vHIT could not be examined in the present study. Moreover, the correlation between tumor size and damage to the vestibular nerves or end-organs, such as the semicircular canals and otolith organs, should be investigated histopathologically in future studies.
Conclusions
A significant negative correlation between VOR gain as evaluated by vHIT and hearing loss was observed and there was a significant difference in hearing loss between the patients with CUS and without CUS in HSC. These results indicate that damage to the audio and vestibular systems in patients with VS may be correlated. As it has been suggested that tumor size is not significant factor in VOR gain, multifactorial causes rather than simple compression of the vestibular nerves alone, may be related to the dysfunction of the semicircular canals in patients with vestibular schwannoma.
Conflict of interest
The authors declare that they have no conflict of interest.