
Abstract
The aim of the present study was to evaluate the severity of vestibular drop attack (VDA) in Ménière’s disease (MD) and to examine the association between VDA severity and other MD-related complaints. The study used a cross-sectional survey design using an electronic questionnaire. The mean age of participants was 56.7 years, and the mean duration of MD was 12.4 years. Four categories of VDA were identified based on level of severity. VDA occurred in 305 (50.7%) of the 602 patients. Of these, 133 patients (22%) experienced mild VDA (i.e., associated with tripping); 80 (13%) experienced moderate VDA (i.e., associated with fall threat unless they had been able to grab support); and 92 (15%) experienced severe VDA (i.e., patients fell to the ground, as in a classical Tumarkin attack). In 70%of participants, VDA occurred less than once a week. VDA lasted for only a few seconds in 90%of participants. 87%reported single attacks, whereas 13%experienced VDA in clusters. VDA was associated with visual auras, reduced quality of life, poor postural control, and fatigue. Approximately half of MD patients experience VDA with varying degrees of severity. If VDA causes falls or near-falls, the attacks should be appropriately treated.
Introduction
Ménière’s disease (MD) is an inner ear disorder consisting of episodic vertigo, fluctuant hearing loss, tinnitus, and aural fullness [18]. The essential element of the illness is, in the inner ear, accumulation of endolymph that causes so-called endolymphatic hydrops that can be visualized in MRI [20]. Too little attention has been paid to ailments of the otolith system and to the association of the vestibular system with the cognitive [3] and autonomic nervous systems [46]. The vestibular and otolithic ailments have been frequently observed in MRI [32] and can be recorded with tailored tests like visual vertical recordings, cervical Vestibular Evoked Myogenic Potential (cVEMP), and ocular Vestibular Evoked Myogenic Potential (oVEMP) [14].
Tumarkin was the first to report sudden vestibular drop attacks (VDA) when one of his male patients with MD suddenly slumped to the ground without vertigo and without losing consciousness [42]. Na-med Tumarkin’s Otolithic Crisis, or “Tumarkin att-acks,” these events were found to be an ailment of the otolith system. Patients often describe VDA as a sudden alteration of lower extremity muscle tone and sometimes as a violent sense of being pushed [11]. Jansen and Russel [11] said that “the most distressing aspect of the attacks to the patients was the lack of warning and suddenness with which they occurred.” Other complaints in MD associated with the otolith system are postural instability and gait problems [26]. Recent evidence indicates that patients with VDA can lose consciousness for a short period of time [28].
VDA can also lead to dangerous falls, although not in every case. More studies must look at the varying severity of VDA in MD patients. A study by Morales, Angulo and Teran [19] showed that 33%of MD patients developed VDA in which the diagnostic criteria included falling to the ground. With a broader definition of VDA (consisting of attacks that do and do not lead to a fall), Kentala et al. [12] reported VDA in 72%of 243 studied patients with MD. However, other studies, perhaps ones with a narrower definition of VDA, have reported lower prevalence numbers ranging from 3.3%to 14%[4 , 45]. A more recent estimation indicates that VDA occurs with variable severity among 50–72%of MD patients [31, 34]. While Tumarkin attacks focus on the fall to the ground, and those more severe attacks can result in injury [31], it is obvious that in milder forms of VDA, patients may experience only a near-fall—they have the ability to reach for nearby support and avoid the fall. A modern concept of otolithic ailments should allow for varying degrees of severity in VDA, but more studies like this one are necessary to establish those classifications.
The aim of the present study was to evaluate the severity of VDA in MD and to examine the association between VDA severity and other MD-related complaints.
Method
Study design and participants
The study used a cross-sectional survey design to analyze data. Permission was obtained from the Finnish Ménière Federation (FMF; Suomen Meniere-liitto) to analyse registry data that the organisation collects from its members. Finnish law does not require ethical approval for analysing and reporting registry data that was collected by the patient organization. The data were collected from responses to an extensive questionnaire on MD symptoms. The FMF has 1,453 individual members but was missing 501 e-mail addresses; hence, 952 members received the survey. Four email reminders were sent to those who did not respond to the initial request to complete the survey; ultimately, 602 members responded (i.e., 63.2%response rate) to the survey. The mean age of the study participants was 56.7 years (range 25 to 75 years). The mean duration of the disease was 12.4 years (range 0.5 to 35 years). The respondents included 477 (79.2%) females and 125 (20.8%) males, these numbers thus representing the gender distribution of FMF. In order to characterize the diagnosis of MD among FMF members, we previously evaluated diagnostic accuracy in a group of members (n = 706) and compared those data with criteria from the 1995 American Academy of Otolaryngology –Head and Neck Surgery (AAO-HNS). According to AAO-HNS, 97.0%of members had definite MD, and 2.7%had probable MD [38].
Data collection
Data were collected via an electronic questionnaire (see Appendix) that was refined and developed according to input from 12 FMF board members [33]. The questions focused on VDA-related impacts on daily life, socioeconomic issues, and complaints of MD. In this study, VDA was defined as “a short attack of sudden perturbation of postural stability that was not associated with head movement.” We classified VDA as mild when the patient experienced the sudden feeling of instability associated with tripping; as moderate when the patient could search for support with hands and prevent falling; and as severe when the patient could not prevent a complete fall.
Certain questions investigated whether the participant or anyone observing them had eye-witnessed any transient loss of consciousness (T-LoC) in connection with VDA [33]. In addition, there were six assessments, using a mixture of open- and closed-ended questions, that addressed MD complaints and daily life impacts related to VDA. In structured (i.e., closed) questions, the impact of VDA was rated on a four-point scale from no impact to severe impact. The diagnosis of migraine was based on previous medical diagnoses mostly carried out by neurologists, and four questions specifically addressed headache [25]. Three questions focused on visual aura experiences. Finally, we adopted the visual analogue scale (VAS) instrument from EQ-5D-3L EuroQol to measure the impact of a patient’s current situation on their general health-related quality of life (HRQoL) [16, 27].
Data analysis
Descriptive statistics were used to explore the data. For continuous variables, we used analysis of variance (ANOVA), when data was normally distributed, and the non-parametric Kruskal-Wallis H test, when data was not normally distributed, to study differences between groups. Chi square test and Fisher’s exact test were used to examine associations among groups for categorical variables. A p-value of 0.05 was used for interpretation of statistical significance.
Results
Association between demographic variables and VDA
VDA was experienced by 305 (50.7%) of the 602 patients. 133 (20.7%) experienced mild VDA (tripping); 80 (13.3%) experienced moderate VDA (near-fall); and the remaining 92 (15.3%) patients ex-perienced severe VDA (complete fall). ANOVA suggested no difference among the three categories for age or duration of MD, and a Chi square test (see Table 1) showed no statistically significant differences in gender distribution.
Age, duration of MD and gender distribution classified by severity of the VDA. Mean and SD are given
Occurrence and impact of VDA among patients with MD
The most commonly reported duration of VDA was only a few seconds (90%), but in some patients, it lasted for a minute or more (see Table 2). A majority (i.e., 71%) reported attacks that occurred only once a week or so, while some patients experienced VDA weekly or daily. Although the VDA usually occurred in single occasion (87%), some patients experienced a cluster of attacks (13%). We further explored the occurrence of VDA in clusters, as it has been clinically associated with benign recurrent vertigo and migraine. VDA in clusters was prevalent in subjects with falls or near falls (X2 = 8.918, p = 0.012). VDA in clusters also caused social limitations, restricted work ability, restriction of life, and anxiety. Clustered attacks were not associated with migraine (X 2 = 0.001, p = 0.976), and headache was also less frequent (X 2 = 3.913, p = 0.048). 15%of participants with VDA reported T-LoC; 7%reported it as their own experience, and 8%had an outside eyewitness to confirm.
Duration, frequency, clustering of attacks and transient loss of consciousness in VDA. Number of subjects and percentages are shown
Association of VDA with visual complaints of MD
Table 3 presents Chi square test results showing that VDA was associated with temporary visual impairments in connection with vertigo: impairments included saw tooth phenomenon, occurrence of moving black spots, part of the visual field absent, and problems watching the computer. Visual impairments increased with severity of VDA (see Fig. 1). Patients with VDA had headache and migraine more often than non-VDA patients (see Table 3).
Distribution of visual aura, migraine and headache associated with MD based on severity of VDA. Mean, SD, and Chi square test results are presented

Occurrence of visual complaints based on VDA severity. (1a) Occurrence of saw tooth in the eyes, (1b) Occurrence of black moving spot, (1c) Occurrence of absent visual field, and (1d) Visual problems with computer work. The y-axis indicatesproportion of the population affected with the complaint, and the x-axis indicates the severity of the VDA. Mean and 95%of CI are shown. (* = p < 0.05between no VDA and VDA groups).
Association of VDA with complaints of MD
Table 4 presents Chi square test results showing that, when compared to those not having VDA, MD patients with VDA experienced vertigo spells, bal-ance problems, fatigue, and hyperacusis more frequently. However, no differences between the two groups were found for tinnitus or hearing problems. Figure 2 demonstrates the impact of VDA on post-ural stability. In a Chi square test, balance problems increased with severity of VDA (X2 = 55.127, p < 0.001).
Distribution of different variables associated with MD based on VDA severity. The severity of VDA was scaled as no VDA, mild VDA, moderate VDA, and severe VDA. Mean, SD, and Chi square test results are presented

Occurrence of balance problems based on severity of VDA. Mean and 95%of CI are shown (* = p < 0.05; *** = p < 0.001).
In pairwise comparison using Fisher’s exact test, no difference was observed among patients with no VDA and mild VDA (p = 0.081) (see Fig. 2). The no VDA group differed significantly from the moderate (p < 0.001) and severe VDA groups (p < 0.001). The mild VDA group also differed significantly from the moderate (p = 0.016) and severe VDA gro-ups (p < 0.001). No significant differences were obs-erved between the moderate and severe VDA groups (p = 0.072).
Impact of VDA on HRQoL
When examining the impact of VDA on HRQoL using ANOVA, a VAS instrument with ratings ranging from 0–100 was used as the dependent variable, and VDA severity was the independent variable. We found a statistically significant difference in HRQoL between the groups (F = 12.4, p < 0.001), and the more severe VDA groups showed relatively worsening HRQoL. Bonferroni post-hoc tests showed that only the severe VDA group (i.e., patients who had fallen) differed from other groups (p < 0.001), but no differences were observed among no VDA, mild VDA, and moderate VDA groups (see Fig. 3).
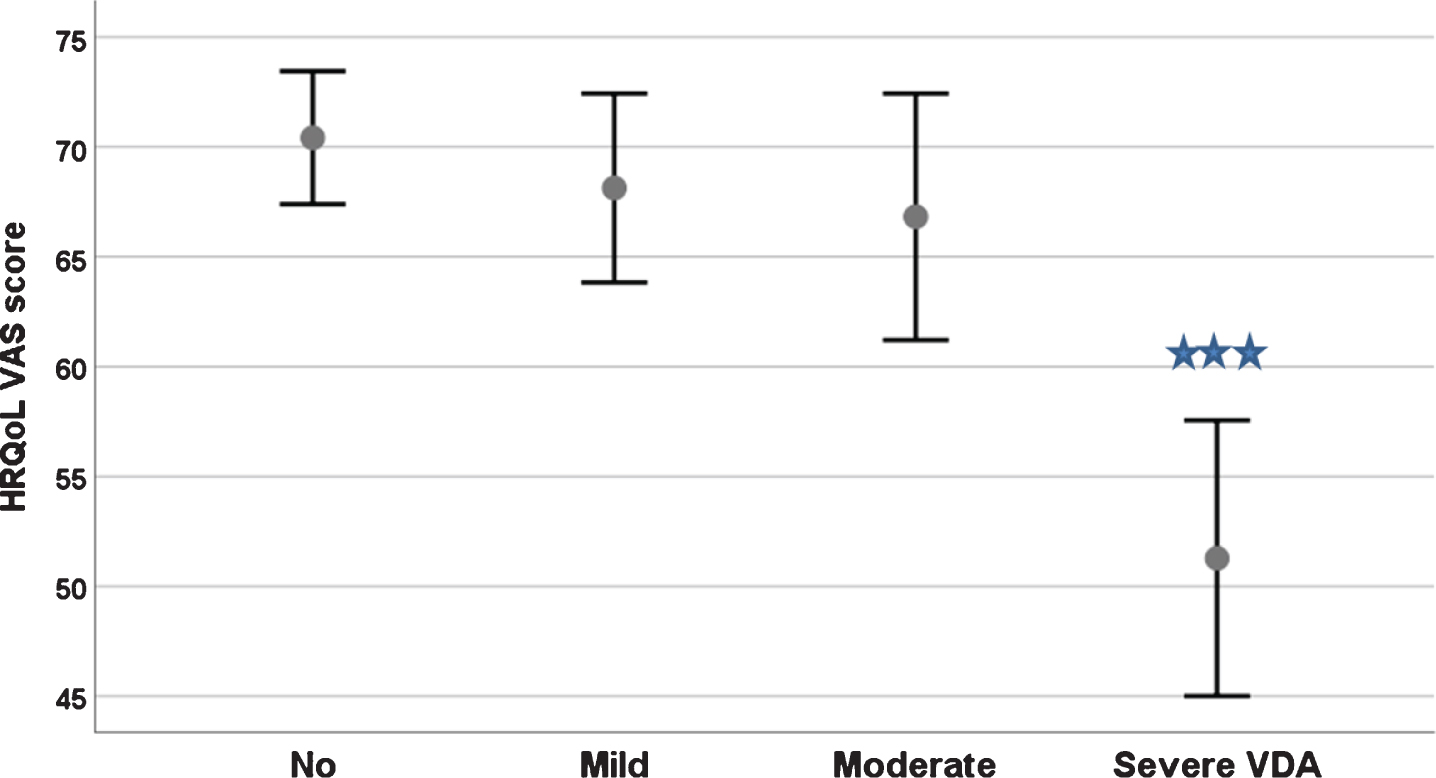
The effect of VDA severity on health-related quality of life measured using theVAS scale of EQ-5D-3L instrument. Mean and 95%of CI are shown (*** = p < 0.001).
Discussion
The current study explored VDA severity in MD as well as associations between VDA severity and MD complaints. VDA was defined as “a short attack of sudden perturbation of postural stability that was not associated with head movement.” This definition covers a wider spectrum of balance problems and differentiates the original definition of Tumarkin attacks (i.e., a limited definition that suggests all VDA sufferers experience complete falls to the ground). As the current study included milder cases, the prevalence of VDA in MD was 50.7%, which is much higher than what is reported in the literature [4 , 45]. Of these, two-thirds of the cases were mild to moderate VDA, and only one-third experienced severe VDA in which patients fell to the ground.
Further, 13%of patients with VDA experienced T-LoC (6.5%of all subjects with MD) —these numbers agree with other recently published studies [4, 29]. In half of the cases, VDA associated with T-LoC was eye-witnessed [33]. VDA attacks varied in terms of frequency and were often associated with visual complaints. Moreover, VDA impacted HRQoL, and it was associated with fatigue, increased balance problems, and anxiety. However, it is noteworthy that in the classification recommendation of MD, there are no instructions to indicate possible involvement of the otolith organ in MD [18]. Nevertheless, physicians treating MD patients should be aware and keep watch for VDA that occurs in variable degrees of severity [27]. They should also discuss with their patients the possible restrictions and injuries associated with VDA [31]. If VDA causes falls or even near-falls, the attacks should be appropriately treated.
Effect of vestibular problems on autonomic nervous system and related cognitive processes
The specific role of the otolith is to provide a gravitational reference frame with semi-circular canals, which interpret other sensory signals, to provide agile mobility, stable vision, and autonomic control of the cardiovascular and other gravity-sensitive systems [5 , 35]. This, in turn, is critical for the vestibular contribution to cognitive processes such as spatial memory and spatial orientation. Less is known about the autonomic nervous system elements such as fatigue, anxiousness, visual aura, and T-LoC [2, 39]. Our recent studies have shown that the visual complaints are common in VDA and are in correlation with T-LoC associated with MD [16, 28]. Abnormal cardiovascular responses in vestibular patients are mediated by vestibulo-sympathetic reflexes originating from otolith afferents to serve body homeostasis during rapid rise from the lying position [37], and failure can produce postural hypotony and cardio-inhibitory reflexes that trigger T-LoC events [16 , 46].
Vestibular afferents influence the visual system in many different ways. The most well-known effects after vestibular lesion are oscillopsia and changes in the visual vertical. We observed visual aura effects such as moving visual spots, saw tooth, or a partial loss of the visual field. Vestibular-induced visual auras seem to be generated by the stimulation of the otolith afferent [13]. We found it noteworthy that visual aura perceptions in the present study were not associated with migraine [6, 47].
Most physical illnesses are associated with fatigue, although it is often viewed as one of the least im-portant symptoms by physicians [17]. It is a key component in many instruments measuring HRQoL, including the 15D instrument [40] and the SF-36 instrument [21]. Fatigue is a subjective sensation of tiredness and lack of energy and is characterized by weariness unrelated to activity levels. The brain me-chanism causing fatigue is largely unknown [17]. In a population study among 9,062 repliers on fatigue symptoms, short-term fatigue (< 6 months) was rep-orted by 5%and chronic fatigue by 31%(> 6 mon-ths), whereas “chronic fatigue-like syndrome” was present only in 1%of the population [43]. In benign paroxysmal positional vertigo (BPPV), moderate fatigue appeared in about 30%of subjects [23]. Levo et al. [15] adopted a fatigue question from the 15D instrument and administered it among 728 patients with MD. In that study, 70%of subjects with MD reported fatigue, and 30%were moderately or sev-erely exhausted. In the present study, fatigue correlated with severity of VDA. We observed that 40%of the no VDA group and up to 70%of those in the moderate or severe group reported fatigue. Our findings confirm the outcome of a study by Perez-Fernandez et al. [22], who observed that patients with Tumarkin attacks were more disabled and experienced more autonomic nervous symptoms and fatigue. As fatigue is a common complaint in MD and especially in its severe form, it should be included and addressed in therapeutic procedures [15 , 31].
Balance problems
Balance problems are among the leading complaints of MD patients, and some are due to VDA and otolithic ailments. The two organs of the otolith are the utricle and saccule: the utriculus controls linear movements of the head, and the sacculus reacts to linear acceleration against gravity. Igarahsi and Kato [9] made selective lesions in the vestibular organs of squirrel monkeys and found that a lesion in the utriculus led to the most prominent changes in body posture, whereas the sacculus was not so important. Also noteworthy was that semi-circular canal ablation led to significant balance problems, indicating that signals from the otolith organ and the semi-circular canal system must collaborate to execute normal gait and balance.
Layman et al. [14] evaluated utricular and saccular function with oVEMP and cVEMP, respectively, and related these to gait in 246 subjects participating in an aging study. They found that saccular function was associated with changes in gait. The finding of significant associations between cVEMPs and gait speed is consistent with prior studies demonstrating a greater role by the saccule during locomotion [24, 44]. Thus, dysfunction of the saccule could delay information needed for multisensory integration and coordinated gait. The lack of utricular influence on gait may also reflect the anatomy and physiology of the utricle. Ramos et al. [36] electrically stimulated the otolith with prosthetic implants in two patients with bilateral vestibular function loss. The stimulation resulted in significant improvement in postural control, gait, and associated visual exploratory functions. Both maculae utriculus and sacculus are involved in translations and tilts as both of these stimulate the hair cells in a similar way [39].
The disease characteristics of MD could differ depending on unilateral or bilateral occurrence [1], although this was not considered in the current study. A bilateral involvement of the MD could theoretically lead to higher prevalence of VDA, as both ears could cause VDA. Endolymphatic hydrops can be symptomatic or asymptomatic, although MD diagnosis is based on symptoms. In MRI we previously indicated that up to 65%of patients with unilateral MD had endolymphatic hydrops also in the asymptomatic ear [32]. Huppert et al. [8] analysed the data from 46 studies (with a total of 7,852 patients) and found that the bilaterality of MD increased with longer duration of the disease (up to 35%within 10 years, up to 47%within 20 years). However, in the present study, neither age nor the duration of MD correlated with VDA, indicating that the bilaterality of MD may not explain the occurrence of VDA nor the severity of it. This topic, however, deserves to be studied more carefully.
Study limitations
The current study used a broader definition of VDA than the original Tumarkin definition and demonstrated that differing levels of VDA severity are associated with various complaints of MD. However, the study has a few limitations. First, the response rate of subjects was 63%. This means that there could be some sampling bias from including less symptomatic patients in the current study. Second, the study did not differentiate unilateral versus bilateral MD patients, which could have bearing on the interpretation of results. Researchers must consider and account for these limitations when planning future studies.
Conclusions
We evaluated the character, frequency, and severity of VDA among patients with MD. We used a novel classification system based on an expanded definition of VDA that explored mild (tripping), moderate (near-fall), and severe (complete fall) levels of VDA. The results indicated that VDA, mostly mild, occurred in 50%of the 602 patients who were members of a patient organization in Finland. In all participants with MD, 21%experienced mild VDA (tripping); 13%experienced moderate VDA (the threat of a fall unless they had been able to grab support), and 15%participants experienced severe VDA (fell to the ground as in classical Tumarkin attack). In 90%of participants, VDA rarely occurred more than once a week, and 86%had single attacks, whereas 14%had VDA in clusters. In 15%of the participants with VDA, attacks were associated with short bouts of T-LoC. VDA was associated with visual auras, reduced HRQoL, poor postural control, and fatigue. These effects should be noted by physicians and included in therapeutic procedures to treat MD patients.
Author contributions
IP conceived this study, and it was designed by VM. NP collected the data from patients with MD. This manuscript was drafted by IP. All authors critically appraised and approved the manuscript.
Conflict of interest
None to declare.
Funding
None to declare.
Footnotes
Appendix
Questionnaire
Full day job Part time job Unemployed Pension Sick leave
below 30 years 31–40 years 41–50 years 51–60 years 61–70 years over 70 y. = 6
less than 1 year 1–5 year 6–10 year 11–20 year 21–30 year Over 30 years
Female = 1 Male = 2
No Yes
No Yes
No Yes
No Yes
No = 1 Yes = 2
No Yes
No Yes
No Yes
No Yes
Free text response option
Your rating:
No Yes
No Yes
No Yes
No Yes
No Yes
The next section focuses on the vestibular drop attacks (VDA). The vestibular drop attacks are often referred to as “tumarkindrop attacks” as these are short lasting attacks during which the subject even in rest without any head movement feels that he/she is being pushed out of balance. The tumarkin attacks usually are very short lasting and their intensity varies from sudden tripping over to falls to the ground. In some rare form of attacks the subject can even become unconscious for short period of time. If you do not have Tumarkin attacks, you can stop answering the survey after answering question 12.
Not at all. In this case move to the end of questionnaire by pressing send button. Yes
No, Tumarkin attacks Few seconds = 2 A minute of more
No,tumarkin attacks Less than once a week Weekly Daily
No,tumarkin attacks Single occurrence Experienced in clusters
No,tumarkin attacks No, I have not lost my consciousness during an attack Yes, on my own opinion I have lost consciousness during an attack Yes, I have a witness who has confirmed my unconsciousness during an attack
Free text response option
No,tumarkin attacks Tripping over Without support I have fallen I have fallen
No,tumarkin attacks I have not suffered from injuries I have been injured
Free text response option
No Tumarkin attacks Do not impact in my life Impacts my life
No, tumarkinattacks Do not impair my work ability Impairs my work ability
No Tumarkin attacks = 1 Do not impact my social participation = 2 Impacts my social participation = 3
No,tumarkin attacks Does not cause fear or anxiety Cause fear or anxiety