
Abstract
BACKGROUND:
Vestibular drop attacks (VDA), also called Tumarkin otolith crises as a complication of Ménière’s disease (MD) were first described in 1936. Nevertheless, a clearer understanding of their prevalence and manifestations is needed.
THE OBJECTIVE:
of this review is to determine the frequency, correlates and consequences of VDA in MD.
METHOD:
Three databases were searched (i.e., MEDLINE, PubMed and Google Academia). A total of 1,791 references were identified, of which 18 studies were considered eligible. There was a large variation in the definition of VDA used in the studies.
RESULTS:
The frequency of VDA in MD leading to a fall to the ground varied from 3 to 19% in 9 hospital-based studies. In studies where a less restrictive definition of VDA included attacks with postural perturbation, tripping and near-to-fall situations was used the prevalence ranged from 50 to 72%. The pooled frequency of VDA leading to fall to the ground was 8% (95% CI 4 to 12%) in hospital-based studies. In these studies, VDA often occurred in severe and advanced MD whereas in cohort studies such connection was not found. Co-morbidity with migraine increased the likelihood of VDA occurrence in MD. In 3 studies syncope was recorded in connection to VDA with falls. In terms of clinical manifestation, audiometry, MRI, vestibular evoked muscle response measures indicated endolymphatic hydrops with involvement of the otolith system. The hearing loss was more pronounced, and balance was worse in MD patients with VDA than in those without. Injury associated with VDA was reported in only one study.
CONCLUSIONS:
VDA is a common phenomenon in MD, occurring even in mild MD and complicated with syncope. Some preliminary evidence suggests that VDA may lead to severe injuries.
Introduction
Vestibular drop attacks (VDA), also called Tumarkin otolith crises or Tumarin attacks, has been described as a complication of Ménière’s disease (MD) since 1936 [41]. They represent abrupt loss of muscular tone in lower extremities related to sudden otolith dysfunction in the sacculus and/or utriculus. In the otolith system, the utriculus has the force vector directing to horizontal direction and in this way control the linear movements of the head. The sacculus is lying vertically and reacts to linear acceleration against gravity. The pathophysiological mechanism of VDA has been suggested to be caused by sudden changes in pressure gradients within the inner ear in MD [6].
In some recent studies, the VDA was defined as sudden imbalance without head movement occurring in even sitting position [16, 27]. This definition of VDA covers wider spectra of balance derangements and differs from the original definition of “Tumarkin attacks” that subjects who fell to the ground. Although VDA usually does not present with loss of consciousness, vestibular syncope has been described recently in VDA [8, 29]. VDA can develop with no warning, predisposing the subject to injuries and decreasing their quality of life [30, 31].
The frequency of VDA varies greatly in different studies [9, 44]. So far there are few studies on the prevalence and characteristics of the VDA in patients with MD. A clearer understanding of the prevalence of VDA and its manifestations in MD patients is needed. The current review was aimed at determining the frequency, correlates and consequences of VDA in MD patients.
Method
Search criteria
Three databases were searched: MEDLINE, PubMed and Google Scholar (from inception to 30 April 2020). The following search terms were used as free text or controlled vocabulary (i.e. medical subject headings (MeSH)) as appropriate for each database: ‘Ménière’s disease’, ‘hydrops’, ‘vestibular’, ‘drop attack’, ‘Tumarkin crisis.’ The searches revealed 1784, 1331 and 306 results correspondingly. Further literature was sought through the reference list and citation trails of eligible studies.
Inclusion and exclusion criteria
No language or time restrictions were applied. Non-English articles were translated. All observational study designs were accepted with the exception of case-reports, studies with age and gender limits, and case series of fewer than 10 participants.
Study eligibility screening
Titles and abstracts of all references identified through the searches were screened and full-text articles of potentially relevant studies were examined by one researcher (MK) to identify those meeting inclusion criteria. Figure 1 presents the PRISMA flow diagram for the systematic review process.
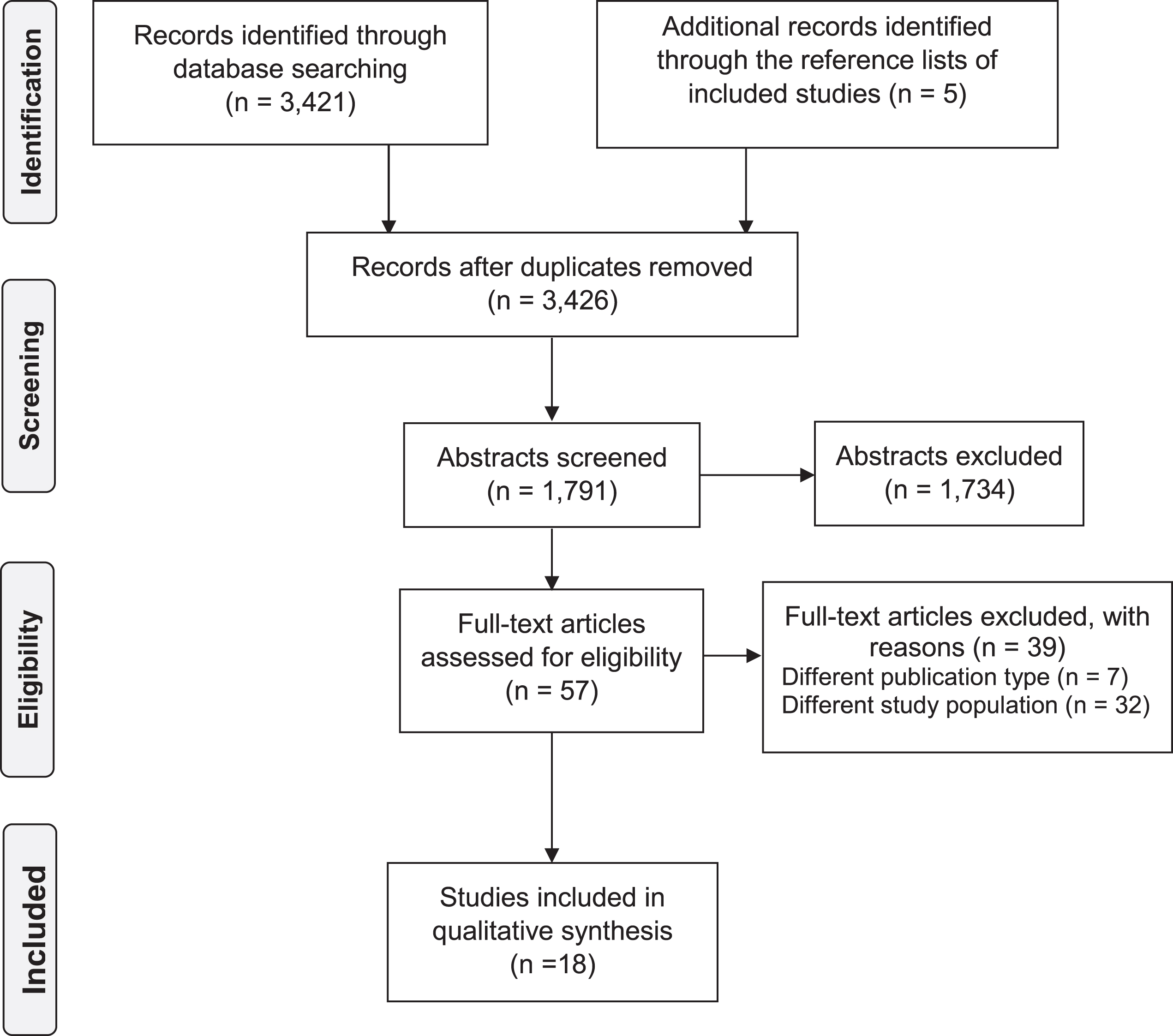
PRISMA flow diagram for the systematic review process.
Data extraction included the region, country, age of the study population, sample size, recruiting site, frequency of VDA in MD, criteria used for the diagnosis of MD, methodologies (i.e., clinical manifestation, audiometric and magnetic resonance imaging (MRI) measures) used to make the diagnosis and to identify correlates of VDA in patients with MD. Two researchers extracted data independently (MK & IP). Results were presented following the PRISMA guidelines [20]. Publication bias was assessed by inspecting funnel plots. Egger‘s tests was also conducted to assess funnel-plot asymmetry. The evaluation of the quality of the included studies was performed using a modified version of Newcastle-Ottawa scale, which assess several domains, i.e. sample representativeness and size, comparability between respondents and non-respondents, ascertainment of VDA, and statistical quality. Studies were judged to be at low risk of bias (3 points and more) or high risk of bias (less than 3 points) [37].
The overall frequency of VDA in MD in these studies was calculated. Quantitative synthesis of frequency of VDA occurrence in MD was conducted in Stata software using random effects. Meta-regression was conducted to investigate the association between frequency of VDA in MD and continuous covariates (years of publication). Subgroup analyses were performed based on the definition of VDA; criteria used for the diagnosis of MD (criteria of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) 1995), sample size (>150 participant), country where patients were recruited (Asia vs Europe and USA). Correlates and prognosis of VDA in MD were registered.
Results
The review included 18 studies [2, 44] with 2,694 MD patients, 17 [2, 44] of which were cross-sectional. As Pyykko et al. analyzed the data from essentially the same cohort in several studies, we used frequency report from only one of them [30] (see Table 1). Nine [2, 44] of those 17 cross-sectional studies were hospital-based, 8 studies [16, 26–32] were community-based and collected information using questionnaires. In the only longitudinal cohort study, patients with MD had been followed up for 6 months to 12 years [21]. When evaluated by Newcastle-Ottawa quality assessment criteria out of 5 possible points, 3 studies received 3 points, 5 studies – 4 points, 10 studies –5 points (Table 2).
Characteristics of the studies reporting the frequency of vestibular drop-attacks in Meniere’s disease
Characteristics of the studies reporting the frequency of vestibular drop-attacks in Meniere’s disease
MD – Meniere’s disease, VDA – vestibular drop-attacks, AAO-HNS – American Academy of Otolaryngology-Head and Neck Surgery, CNS – central nervous system.
Newcastle-Ottawa risk of bias scores for the 18 studies included in this systematic review and meta-analysis
MD was diagnosed in 15 studies according to guidelines the AAO-HNS [1972, 1995]. In one study, the new criteria of the Barany Society (Barany society 2015) was used. In two early studies, diagnostic criteria for MD were not clearly stated (see Table 1). In Janzen and Russel (1988) research the MD criteria for MD was not mentioned but the patients had recurrent vertigo periods with severe hearing loss in the affected ears and two of them went for endolymphatic sack surgery. The exclusion of other neurological disorders was carefully carried out. We therefore believe that in this paper the AAO-HNS criteria (1985) of definite MD were used. Baloh et al (1990) used criteria based on possible, probable and definite MD. Although the MD criteria were not directly mentioned the authors indicated that their patients had definite MD and we believe based on their reference that the authors followed the criteria of AAO-HNS (1985).
Based on the clinical criteria, VDA was defined either by falling to the ground in 10 studies or was defined less strictly as a short attack of sudden perturbation of postural instability that was not associated with head movement in 8 studies [16, 26–32]. Further the latter studies used classification of VDA: mild VDA, when patients experienced sudden feeling of instability associated with tripping off; moderate VDA, when subjects could search for support with hands, so that falls were prevented; and severe VDA, when they fell to the ground. Thus, VDA in these 8 studies covered larger spectrum of sudden otolith derangements in MD.
Funnel plot provided little evidence for publication bias (Fig. 2). Egger’s tests showed no evidence for asymmetry to suggest publication bias in the studies (P = 0.06)

Funnel plot of the meta-analysis of the included studies.
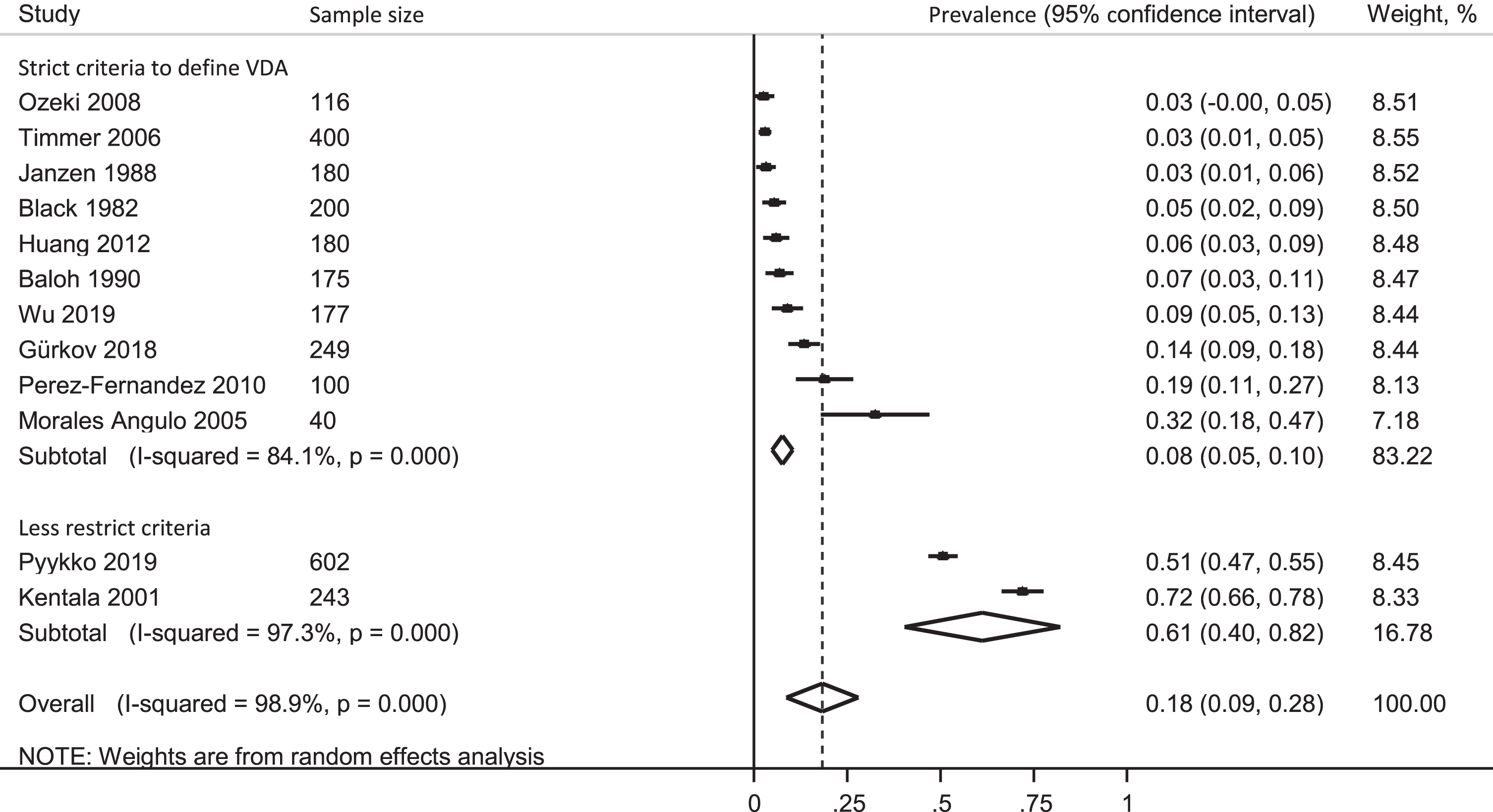
The frequency of VDA in patients with MD varied greatly from 3 to 72% depending on criteria used for diagnosing VDA and study design. The pooled frequency of VDA in MD was 18% (95% confidence interval (CI) 9% to 28%). In an attempt to identify the source of heterogeneity between studies, a subgroup analysis was performed.
First group included cross-sectional hospital-based studies which used strict criteria for VDA, requiring falling to the ground. Pooled frequency of VDA in this group was 7% (95% CI 4% to 9%). The prevalence of VDA in studies that employed wider definition, including not only falling to the ground, but also attacks of sudden loss of balance which caused only slip, varied between 51% to 72% with a pooled average of 61% (95% CI 40% to 82%) (Fig. 3). There is evidence of between group heterogeneity (p < 0.0001), indicating that the frequency of VDA was lower when using strict criteria compared with when using less restrict criteria. However, there was high level of heterogeneity between studies even within each subgroup. The only longitudinal study followed up 40 patients with MD for up to 12 years and found VDA in 32% of the cases. One study [16] reported severity of VDA: 41.6 % were mild (sense of postural perturbation); 49.1 % were moderate (falls could be prevented by searching support); 9.2 % severe impact of VDA leading to fall to the ground respectively.
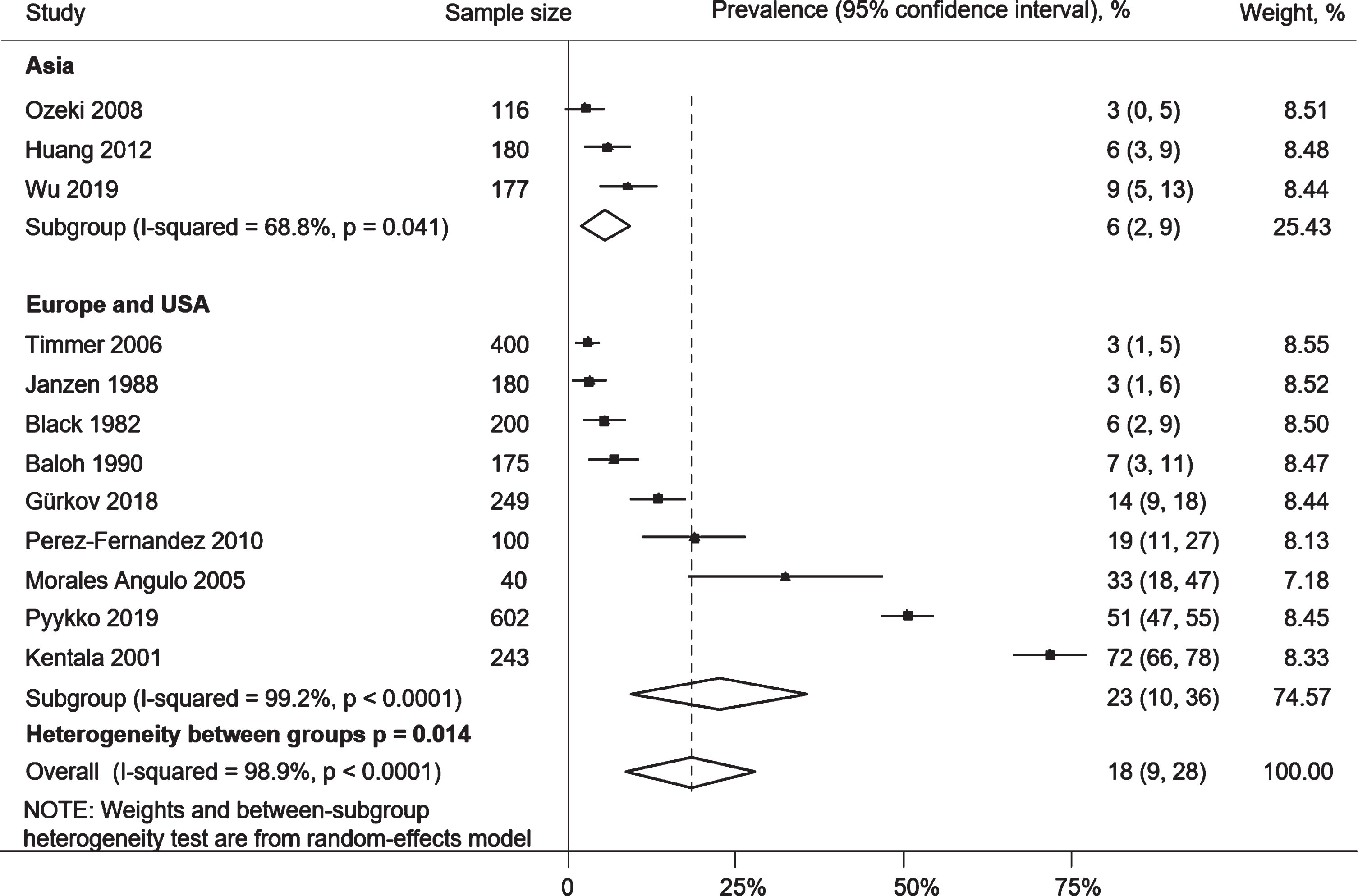
Meta-regression showed no evidence of association between the frequency of VDA in MD and years of publication (p = 0.52). Subgroup analysis revealed that sample size of the studies did not affect the frequency of VDA (p = 0.85, Fig 4). Higher frequency of VDA in MD was observed in the studies conducted in the US or Europe when compared to studies conducted in Asia (p = 0.01, Fig. 5), and in the studies where AAO-HNS 1995 diagnostic criteria for MD was used rather than other criteria (p = 0.02, Fig. 6), albeit there was high level of heterogeneity between studies within most of the subgroups.
The results of subgroup analysis of the frequency of the vestibular drop attacks in Meniere’s disease depending on the criteria used to define VDA.

The results of subgroup analysis of the frequency of the vestibular drop attacks in Meniere’s disease depending on the sample size.
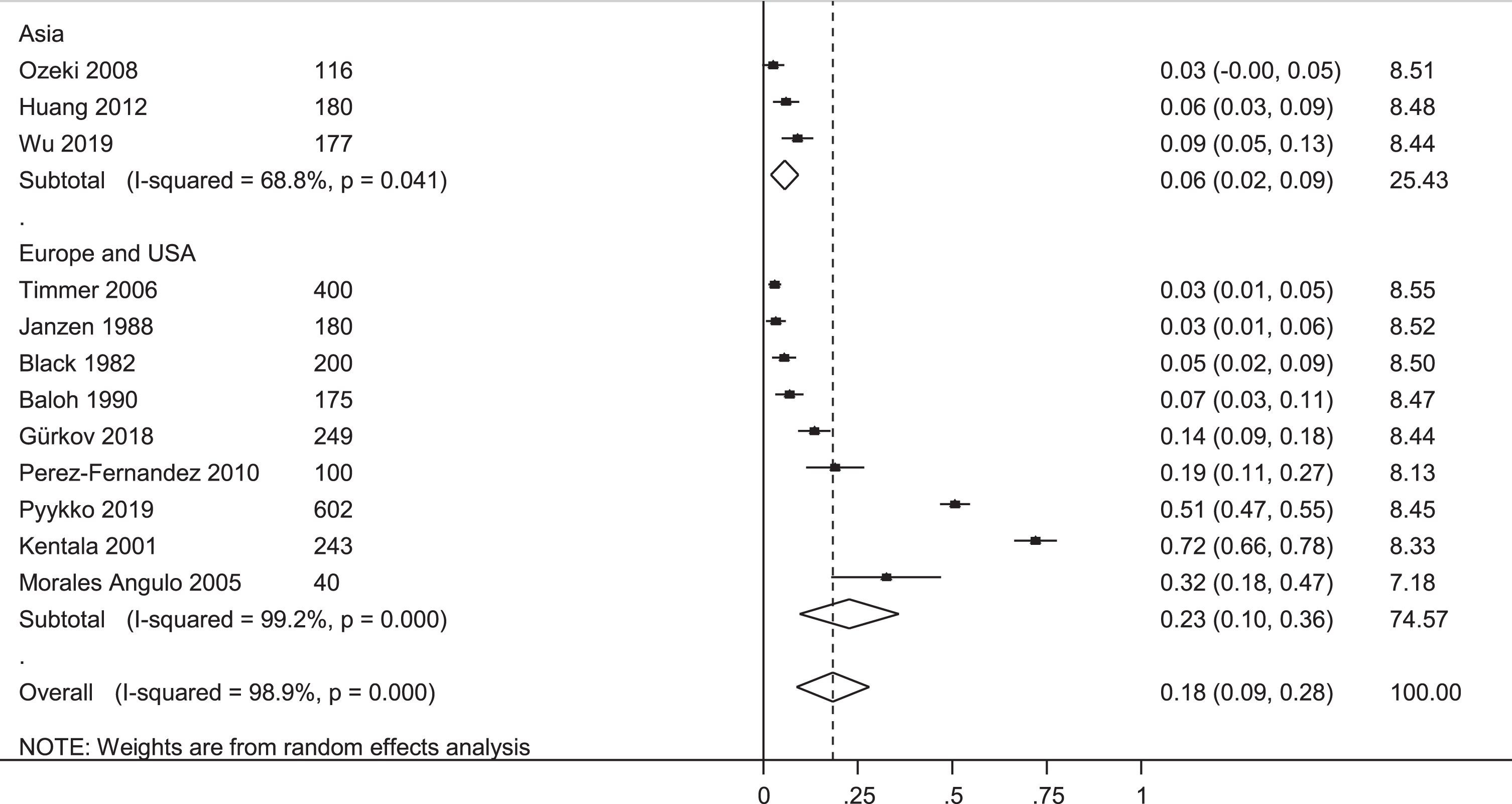
The results of subgroup analysis of the frequency of the vestibular drop attacks in Meniere’s disease depending on the region of the recruitment.
The results of subgroup analysis of the frequency of the vestibular drop attacks in Meniere’s disease (MD) depending on the criteria for MD.
Four studies excluded patients with visual aura or numbness of the face or other neurological complaint during vertigo [2, 40]. In 4 studies, visual and neurological associates with VDA was studied and compared with non-VDA patients [8, 30]. Patients with VDA had significantly more often vertigo, balance problems, fatigue, hyperacusis, visual problems especially when focusing on computer screens, unreal images of sawtooth aura and moving spots in visual field, impaired visual field, headache, migraine than those without VDA [8, 16].
Those who experienced VDA had longer MD course when comparing to those without VDA according to hospital-based studies [8, 44], but this was not confirmed by community-based one [26]. Patients with MD and VDA also had higher scores on the Dizziness Handicap Inventory (DHI) and Vertigo Symptom Scale (VSS) [25], and more severe hearing loss in terms pure-tone average in audiometric testing [25, 44], than those without VDA. Separate analysis of hearing loss at low, middle and high frequencies showed significant difference in hearing in low and middle frequencies [44]. Vestibular and cochlear symptoms at the onset of MD increased the risk of VDA later [8]. Moreover, the presence of VDA in patients with MD correlated with some EQ-5D-3L (i.e., general health related quality of life) components: motility, pain and usual activity [31].
The ratio of endolymphatic to vestibular space area on inner ear gadolinium enhanced MRI, and degree of hydrops in the apical, middle and basal turn of the cochlea were significantly higher in those who suffered from VDA [44]. Electrophysiological studies using ocular and cervical vestibular evoked myogenic potential (VEMP) to test utricular and saccular functions respectively, revealed controversial results. The amplitude of cervical VEMP (cVEMP) was reduced in more (i.e., 41%) of those with VDA in comparison to those without VDA (i.e., 18%, p = 0.01) in one study [39], whilst two studies did not find any difference between the two groups [9, 44]. The amplitude of ocular VEMP (oVEMP) was reduced in all patients with MD and VDA in one study [12], and was not associated with the presence of VDA in another study [44].
Transient loss of consciousness in VDA
Ten studies [2, 44] employed stricter criteria, defining VDA as at least one sudden fall without loss of consciousness and warning. These studies excluded patients who had syncope during VDA. Eight studies published by Pyykko’s group recruited patients with VDA and short lasting syncope [8, 26–32]. The frequency of syncope developing in connection with VDA ranged from 4 to 7 % [8, 27–29].
Outcomes
Injuries related to VDA were reported in only one study [26]. VDA had led to falling among 92 out of 133 patients. Fifty-three patients experienced injuries (38 bruises, 12 fractures, and 3 severe back injuries). Patients with MD and severe VDA were at a higher risk of experiencing a vertigo attack when driving a car [30]. One patient had multiple injuries due to a car crash. Two patients had their partners sitting beside them who prevented car accidents that could have been caused by VDA [26].
Discussion
VDA in MD is a common but underestimated problem. This review showed a scarce of longitudinal data in this area. Different VDA definitions have been used. There was significant heterogeneity in the frequency of VDA in MD patients. In cross-sectional studies 7% of patients with MD (95% CI of 4% to 9%) and in the only longitudinal study 32% had VDA that caused falls to the ground. These studies also excluded patients with MD who became unconscious during a fall. The frequency was on average 61% (95% CI 40% to 82%) when VDA definition was broadened to include tripping off and near falls.
It is clear from this review that the variability in the definition used for VDA is the main issue in determining the frequency of VDA in MD. So far, there are no accepted definitions for VDA in MD. The Barany Society subgroup has defined diagnostic criteria for vestibular paroxysmia [38]. In this classification, the working group defines short lasting (i.e., less than one minute) attacks of spontaneous vertigo of spinning or non-spinning nature. In this definition, VDA could be classified into the frame of this disorder. The consensus document of the Committee for the International Classification of Vestibular Disorders of the Bárány Society [19] on MD has not even mentioned VDA. This may be the reason why, although VDA severely impacting significant number of MD patients, has been systematically explored only in a few studies.
Two studies, which were not included in the current review (due to age limits applied in the studies), reported VDA in the elderly with MD [1, 17]. These papers are important to promote, as in elderly care VDA is usually neglected and often the attack misdiagnosed. Ten (25.6%) out of 39 patients (>65 years) with de novo MD had drop attacks [1]. VDA was one of the reasons (e.g., cardiovascular cause, stroke, epilepsy, medication) for non-traumatic sudden falls in the elderly [17]. VDA were significantly more prevalent among retired persons with MD and were related to social isolation [26]. There is no report on any gender differences.
VDA were less frequent in the studies conducted in Asia than in those from Europe or USA. In theory this could be explain by regional differences, for instances Japanese are likely to consume healthier food and lead more balanced lifestyle than people from western countries. This in turn might explain lower incidence of MD in Japan and probably more benign course of the disease and relative rarity of VDA. Studies comparing the frequency of VDA in patients with unilateral and bilateral MD could possibly shed light on the mechanisms of the former, but we have not identified studies reporting such data.
The complexities of the vestibular system are often underestimated by healthcare providers. The vestibular end organ, the semicircular canals and the otolith system, are responsible for sensing angular head motion in three-dimensional space and for providing neural inputs to the central nervous system essential for agile mobility, stable vision, and autonomic control of the cardiovascular and other gravity-sensitive systems [10, 33]. Little attention has been paid, for example, on MD associated complaints such as fatigue, visual complaints, postural and gait derangements and changes in autonomic nervous system output. Most studies excluded patients with these complaints or did not report any problems as these could have been considered to be signs of neurological disorders, psychosomatic problems, migraine or autonomic nervous system dysfunction rather than result of vestibular dysfunction [7, 36].
As expected, patients with VDA suffered from more severe and disabling MD than patients without VDA and while several authors recommended ‘wait and see’ strategy, others suggested treatment for VDA in MD. The efficacy of conservative therapy in controlling VDA is in controversy according to the limited clinical and objective measures. Limited evidence showed high remission rate using intratympanic gentamicin (ITG) injections. Liu et al. [18] retrospectively analyzed 10 cases of MD and endolymphatic hydrops and showed that VDA in 5 out of 7 cases disappeared after initial ITG course, in 2 cases VDA was controlled after an additional ITG injection. Viana et al. [42] used ITG injections in 24 ears of patients with MD to treat VDA, and reported that a total of 83.3% of ears with intractable MD and VDA achieved complete VDA symptom control after the first ITG cycle and 95.8% after further injections. Positive effect of ITG on VDA was also shown in an earlier report [23]. However, VDA were present in 19.2% [34] and 46% [15] of patients with MD and in the latter study patients with VDA demanded additional interventions such as retreatment with ITG.
In a histological study of temporal bones, Calzada et al. [4] suggested that a mechanism for VDA development in MD is free-floating otoliths and atrophy caused by injury to the otolithic membrane of the saccule and utricle. However, this hypothesis could not distinguish the mechanism of VDA from that of benign paroxysmal positional vertigo (BPPV) [43]. Inconclusive results of electrophysiological studies of VDA in MD could be partly explained by reversibility of the changes of VEMP [24].
Other than MD, VDA has also been described in other vertigo patients existing endolymphatic hydrops cases [12, 17]. Those with co-morbid VDA and endolymphatic hydrops were more likely to suffer from migraine, and the relationship between endolymphatic hydrops and migraine has been acknowledged since 18th century [22]. Several mechanisms of this association was proposed, the most popular one explains development of endolymphatic hydrops in migraine as a result of vasospasm and subsequent ischemia of the labyrinth [39]. Endolymphatic hydrops developed in animals received systematic and secondary round window challenge of keyhole limpet hemocyanin supported an inflammatory mechanism that is common in the inner ear diseases [46].
Several authors reported syncope in connection with the VDA [8, 27–29]. Others excluded syncope in their studies as syncope was not reported in the original paper of Tumarkin (1936) [41]. The same is also true for visual complaints in connection with VDA. In animal work, the abnormal cardiovascular responses is mediated by vestibulo-sympathetic reflexes originating from otolith afferents [45] and can produce postural hypotony and cardio-inhibitory reflexes that triggers transient loss of consciousness [28, 29]. In many, the vestibulo-sympathetic reflexes serve to control the circulatory hemostasis during rising up as the baroreflex function are much slower to react than the vestibular system [5, 14].
The limitation of this meta-analysis is a high degree of heterogeneity between the studies. The majority of studies were cross-sectional which could lead to underestimation of the frequency of VDA in MD. There are also likely to be other series of patients with MD, where VDA was not a focus of the study title or abstract but it is recorded as a comorbidity.
Conclusions
This systematic review and meta-analysis indicate that VDA is a common complication of MD. Three percent to 72% of MD patients had VDA depending on different VDA definitions, and the pooled frequency was 7% (95% CI 4 to 9%) in cross-sectional studies using strict definition requiring falling to the ground. The frequency of VDA in MD was 2-3 times higher in longitudinal study and studies using broadened definition. VDA often develops in severe and advanced MD patients and can be complicated with migraine and syncope. Future research should clarify how they define VDA. Better understanding of correlates will be useful in predicting the condition, diagnosis and risk reduction of sudden falls. Population-based studies are necessary to understand a true frequency of VDA in MD. Further studies should also continue elucidating the mechanisms of VDA development, so as to provide new treatment targets.
The authors report no disclosures.