
Abstract
BACKGROUND:
Cervical Vestibular Evoked Myogenic Potentials (cVEMP) is an electromyogenic measure commonly used in clinic to assess saccule function. The main parameters are peak-peak amplitude and interaural asymmetry ratio (IAR). Several non-vestibular factors may influence these parameters. Notably, a greater EMG contraction level prior to stimulation leads to an increased amplitude. As aging impacts both vestibular structures and muscle propreties, it is still a matter of debate whether the decrease in cVEMP amplitude observed in normal aging is due to EMG differences prior to stimulation or to the effect of aging on the sacculo-collic reflex pathway. At the clinical level, understanding the effect of aging on the relationship between EMG activity and cVEMP response (amplitude, asymmetry ratio) and the effect of normalization is crucial to improving the categorization of healthy versus pathological responses.
OBJECTIVE:
To investigate whether normalization modifies cVEMP amplitude and asymmetry ratios differently in younger and older heatlhy adults.
METHOD:
cVEMP recordings were conducted in 42 normal healthy participants divided in two age groups: younger (n = 29): mean = 22.79 years old SD = 1.66; and older (n = 13): mean = 69.00 years old SD = 3.61. Air-conducted cVEMP were recorded using Eclipse (Interacoustics, Denmark). The stimulus was a 95 dBnHL tone burst (500 Hz) with rise, plateau and fall time of 1 ms. cVEMP were recorded only when EMG levels were between 50μV and 150μV, using the Eclipse (Interacoustic, Denmark) monitoring system.
RESULTS:
No significant differences were observed for prestimulus EMG levels between younger and older participants (F(1,83) = 1.13, p = 0.291). However, significant differences between groups were observed for raw cVEMP amplitude (F(1,83) = 14.78; p < 0.001) and corrected cVEMP amplitude (F(1,83) = 21.85; p < 0.0001). A significant positive linear relationship between prestimulus EMG contraction level (RMS) and raw cVEMP amplitude was observed in younger participants (r2 = 0.234; p < 0.001), but not in older adults (r2 = –0.0144; p = 0.056). Finally, no significant differences between younger and older participants were observed for raw amplitude asymmetry ratios (F(1,41) = 0.124, p = 0.726) or normalized asymmetry ratios (F(1,41) = 0.726, p = 0.508).
CONCLUSION:
Our results suggest that when EMG is monitored and activation of the SCM is sufficient, the observed decline in cVEMP amplitude with normal aging does not seem to be caused by EMG differences and is therefore likely due to the known histopathological modifications of the vestibular system that occurs with normal aging.
Introduction
It is generally accepted that as we age, our sensory functions progressively decline. Accordingly, it is expected that normal aging also affects the function of the vestibular system [15, 18]. These changes are reflected in several clinical vestibular measures [9]. For example, it has been observed that the amplitude of the cervical vestibular evoked myogenic potential (cVEMP) declines with normal aging [1 , 16].
The cVEMP measures the inhibition of the back-ground EMG activity at the level of the ipsilateral sternocleidomastoid muscle (SCM) following ves-tibular stimulation [5, 6]. This stimulation evokes a biphasic potential at the level of the SCM, with a positive peak around 13 ms (P13) and a negative peak around 23 ms (N23), which can be measured with surface EMG electrodes [5]. The recording and interpretation of these potentials can be problematic as several non-vestibular factors can affect their amplitudes. Indeed, it has been observed that greater values of EMG activity of the SCM prior to stimulation lead to greater cVEMP amplitudes [1 , 13]. This quasi-linear relationship between EMG activity prior to stimulation and cVEMP amplitude has led some authors to hypothesize that the decline in cVEMP amplitude observed with normal aging could be linked to a possible difference in EMG activity level [16]. Therefore, to date, it remains difficult to ascertain whether the decline in cVEMP amplitude observed in normal aging is related to differences in EMG activity or if it does reflect the known vestibular changes associated with normal aging.
Techniques have been proposed to control for the influence of EMG variability on cVEMP amplitude. EMG levels can be controlled using either visual feedback on the degree of tonic EMG activity, or by using a blood pressure cuff [17]. This technique allows to control for the force applied during recordings in order to ensure similar EMG values across groups and conditions. It is also possible to mathematically control the effect of EMG activity by dividing either each data point on the curve, or the peak-peak amplitude value, by an estimate of the EMG contraction level prior to stimulation [10, 14]. This method, known as normalization, could help to distinguish the influence of normal vestibular aging from effects of EMG activity on cVEMP parameters such as amplitude and asymmetry ratios.
The objective of this study was therefore to inve-stigate whether normalization affects cVEMP amplitude and asymmetry ratios differently in younger and older heatlhy adults.
Methodology
Participants
Forty-two (42) healthy participants aged between 19–74 years old (mean: 39.2 years old ±21.00) took part in the study. Participants were divided in two age groups: younger (n = 29): mean age = 22.79 years old SD = 1.66 and older (n = 13): mean age = 69.00 years old SD = 3.61. Participants reported no history of vestibular disorders. They did not report any history of diabetes, neurological disorders, middle ear disorders or middle ear surgery, head trauma or neck related problems. All participants gave written informed consent prior to testing.
Protocol
The middle ear function of every participant was assessed using tympanometry (Madsen Zodiac 901). cVEMP were recorded bilaterally in all participants using Eclipse (Interacoustics, Denmark). cVEMP stimulus was a 500 Hz tone burst delivered trough insert earphones at 95 dBnHL with a stimulus rate of 5.1 Hz, a rise/fall time of 1 ms and a plateau of 1 ms. For each individual tracing, participants were in the supine position inclined approximately 30 degrees from horizontal and had to raise and turn their head away from the stimulated ear. During cVEMP recording, we monitored and stored EMG prestimulus activity over a 20 ms period prior to stimulation (measured by root mean square of prestimulus EMG). cVEMP responses were analyzed only when RMS EMG prestimulus was within 49.9μV and 150μV.
Analysis
All raw tracings were exported to a custom made Matlab program and visually inspected to eliminate possible artifacts. P13 and N23 peaks were manually identified and the different parameters were calculated as followed:
To assess the relationship between prestimulus EMG activity and raw cVEMP amplitude, we performed a linear regression analysis (linear least square fit) in both age groups. We also performed a MANOVA two groups X 3 parameters (RMS prestimulus EMG; raw amplitude and normalized amplitude) to assess any differences between groups as for EMG prestimulus, raw amplitude and the effect of amplitude normalization. Finally, a one-way ANOVA was performed to assess the presence of any significant difference between raw and normalized asymmetry ratios in both groups. A Bonferroni correction factor was applied when necessary to correct for multiple comparisions.
Results
Figure 1 shows all raw and normalized cVEMP tracings and the mean amplitude (black line) from all participants for both age groups. The upper row is the right and left tracings from younger participants and the lower row shows tracings from older participants. This figure clearly shows that younger participants present larger raw and normalized cVEMP amplitudes than older participants.

cVEMP tracings for younger and older participants of all raw and normalized cVEMP responses.The black line represents the mean of all tracings. The vertical dotted line represent onset of stimulus.
As can be seen in Fig. 2a, no significant differences were observed in prestimulus EMG level between younger and older participants [F(1,83) = 1.13, p = 0.291]. However, significant differences between groups were observed in both raw [F(1,83) = 14.78; p < 0.001] (Fig. 2b) and normalized [F(1,83) = 21.85; p < 0.0001] cVEMP amplitude (Fig. 2c).
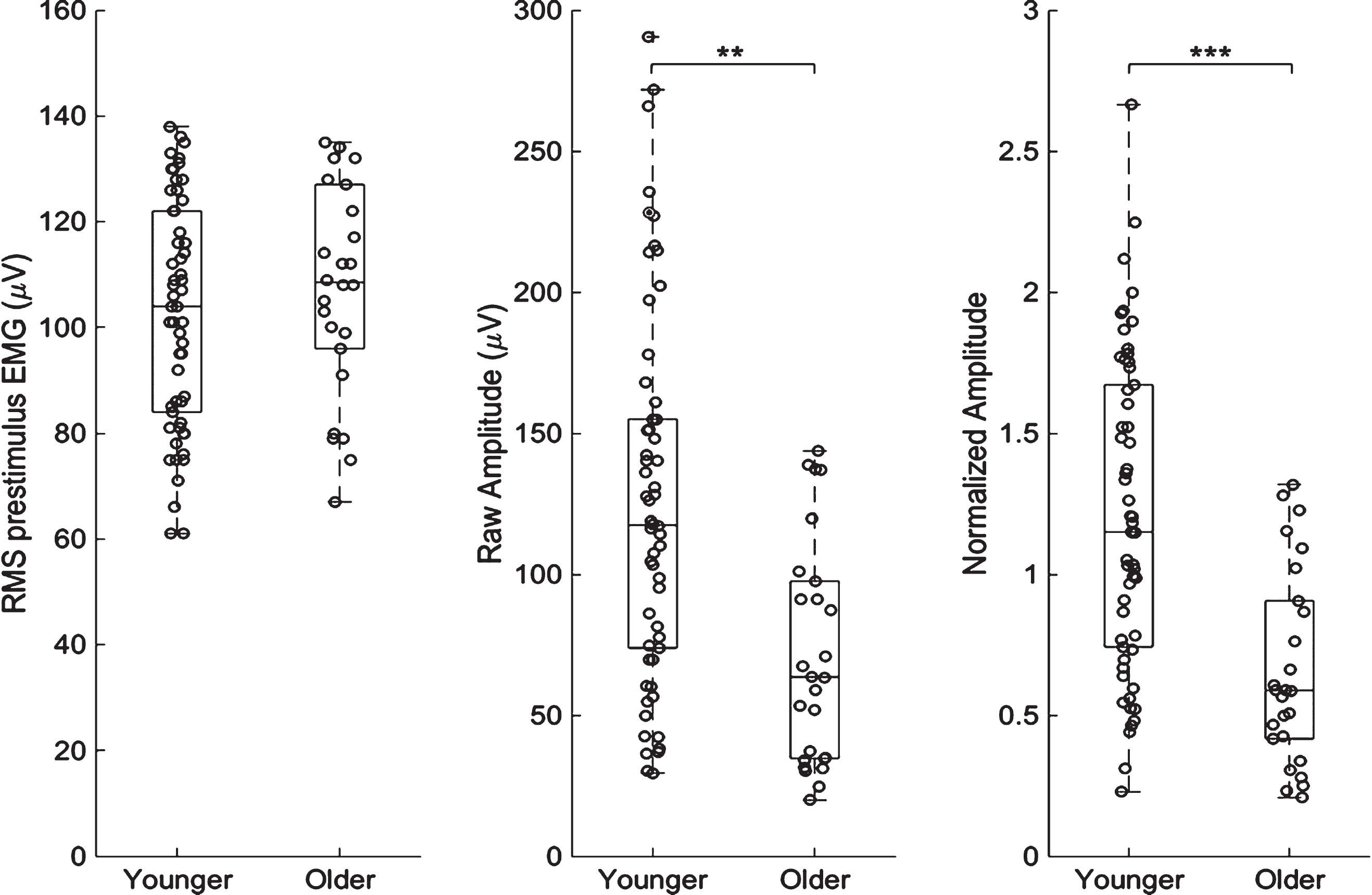
Boxplot with individual data for A) RMS prestimulus EMG, B) raw amplitude, C) normalized amplitude. Significant differences are observed between groups for raw and normalized cVEMP amplitude. ** p < 0.001; *** p < 0.0001.
In Fig. 3 we observe a significant linear relationship between raw cVEMP amplitude and EMG prior to stimulation, but only for younger participants [r2 = 0.234; p < 0.001]. In older participants, a trend suggesting that higher EMG activity could result in higher raw amplitude was observed, but did not reach statistical significance [r2 = 0.0144; p = 0.056].
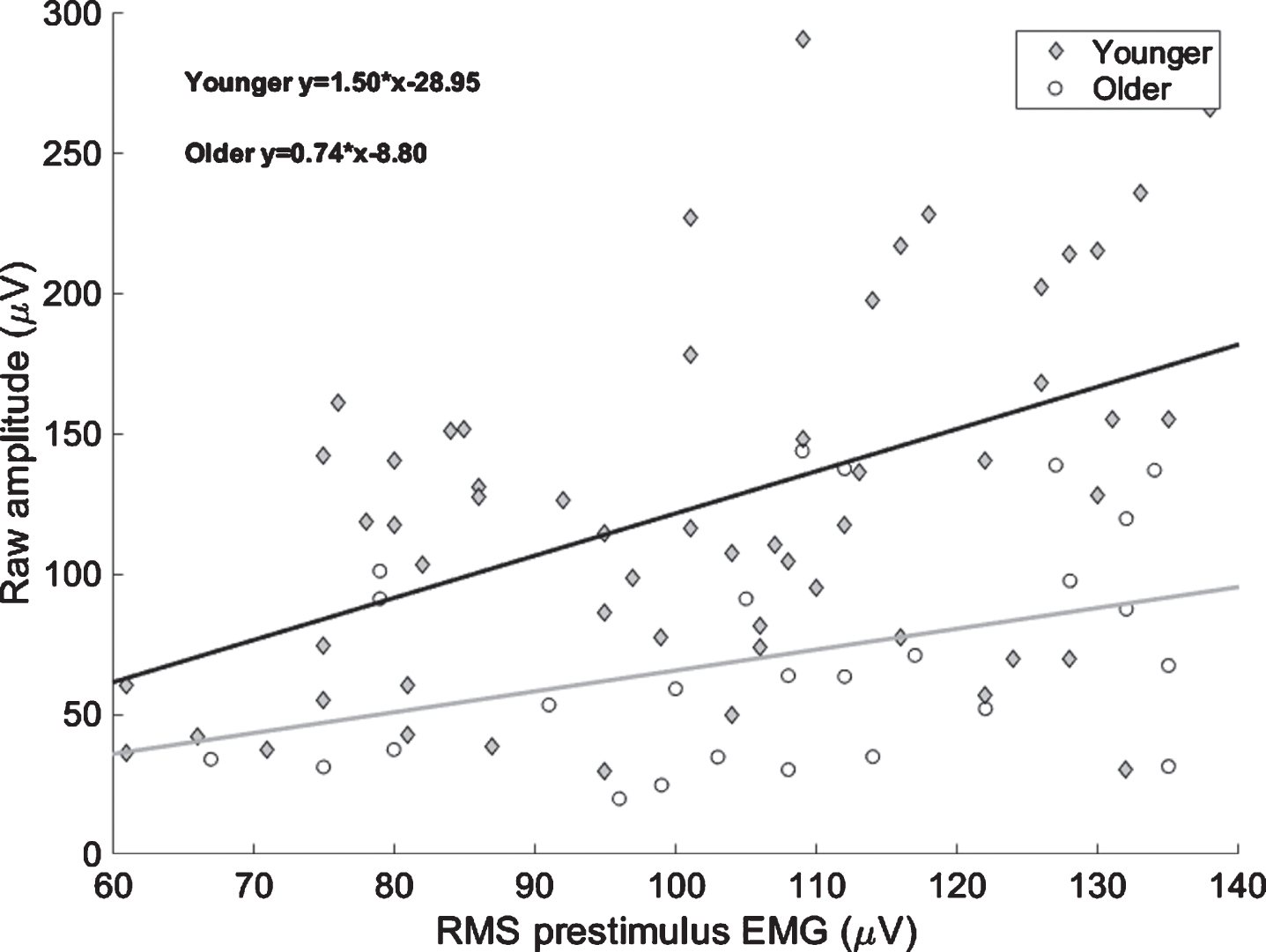
Scatter plot reprensenting the relation between RMS prestimulus EMG and raw cVEMP amplitude for younger (blue) and older (red) participants.
Finally, as can be seen in Fig. 4, no significant difference between younger and older participants were observed for raw amplitude asymmetry ratios [F(1,41) = 0.124, p = 0.726] or normalized amplitude asymmetry ratios [F(1,41) = 0.726, p = 0.508].
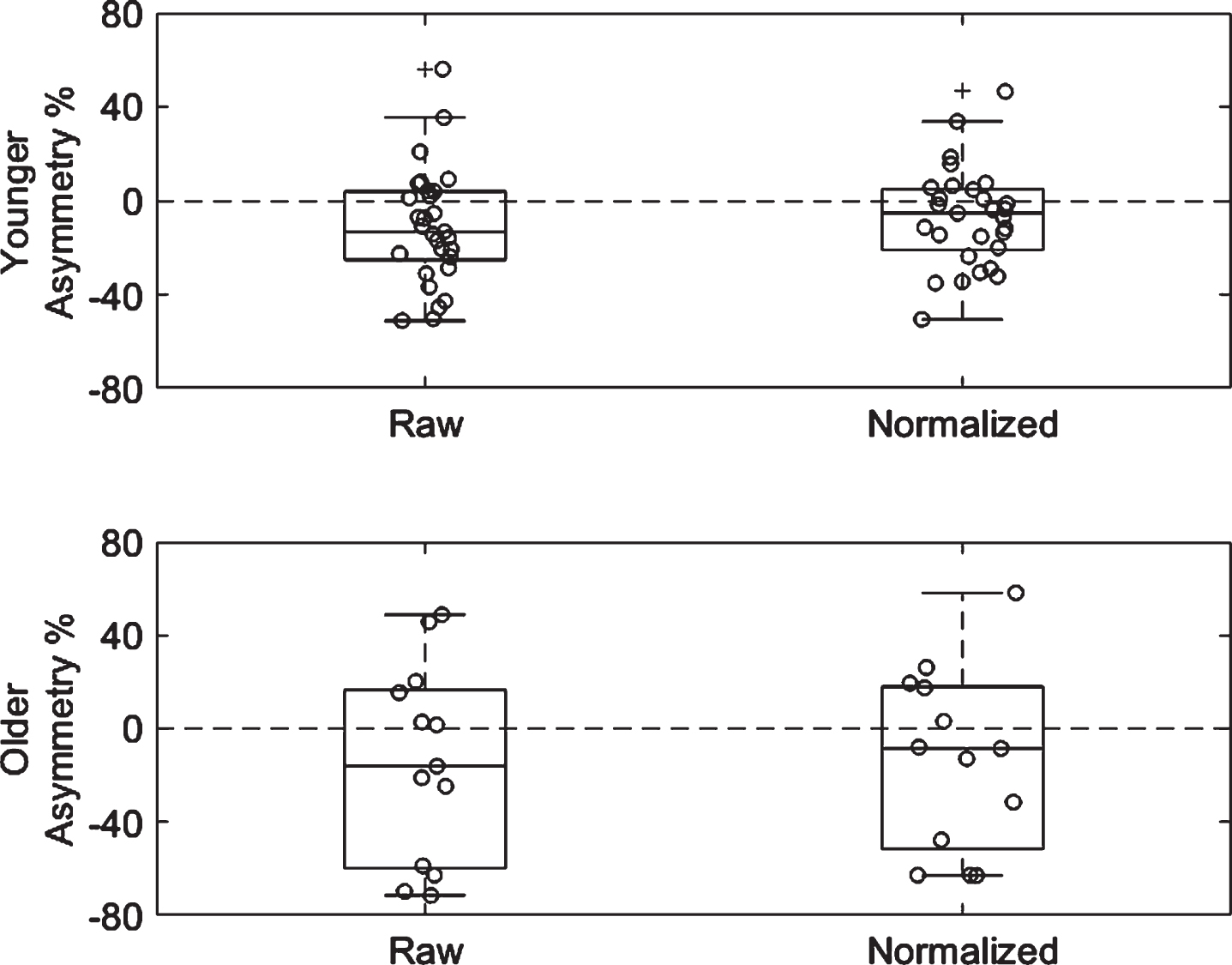
Boxplot with individual data for each group (younger; older) to demonstrate the difference between raw and normalized asymmetry ratio.
The results of the present study show that the observed decline in cVEMP amplitude associated with normal aging may not be entirely due to differences in background EMG activity. In support of this claim, we demonstrated that even though no significant differences were observed between groups for RMS prestimulus EMG level, older participants presented lower raw and normalized cVEMP amplitudes. This suggests that maintaining EMG activity within the range of 49.9μV and 150μV while activating the SCM using a rise and turn in supine position may be sufficient to control for possible EMG differences between younger and older participants. When assessing cVEMP in older adults, actively keeping EMG within a specific EMG band, may be a better option than normalization towards controlling for EMG activity Indeed, in order to normalize cVEMP amplitude, it is a necessary condition that a linear relationship be present between EMG prestimulus and cVEMP raw amplitude [3]. In this study, we demonstrated that when EMG activity is kept within 49.9μV and 150μV, this assumption is true in younger adults, but not in older adults. However, caution is needed before suggesting that EMG has no effect on cVEMP amplitude in older subjects. Indeed, the fact that a non-significant trend was observed (p = 0.056) suggests that EMG could have an influence on cVEMP amplitude, and that absence of a significant relationship may be due to the small sample size.
Our results are in line with previous studies suggesting a decrease in cVEMP amplitude with age [1 , 16]. Until the present study it was not possible to ascertain whether this decrease in cVEMP amplitude was due to the effects of normal aging on the vestibular system or rather to differences with EMG activity levels. Indeed, previous studies either did not use normalization [1 , 16], or reported only the corrected amplitude [8, 12].
The present study suggest that that the decline in cVEMP amplitude is not related to differences in EMG activity prior to stimulation. This seems to contrast with Akin et al. [1], who investigated cVEMP amplitude and EMG level in younger and older adults and suggested that the decrement in cVEMP amplitude was related to both age-related changes in the vestibular system and age-related changes in the sternocleidomastoid muscle. However, several differences between Akin’s et al. [1] and the present study may explain this discrepancy. Indeed, Akin et al., [1] used a different electrode montage to measure EMG activity. This system was a stand-alone differential surface electrode placed at the midpoint of the SCM muscle and a reference electrode, attached to the wrist, that generated much smaller EMG values. Additionally, the participants were in a sitting position and had to rotate their head to activate SCM. This technique is known to generate smaller EMG values [14]. This low EMG activity threshold may have influenced the results as non-linearities have been observed between EMG and cVEMP amplitude at these levels of EMG contraction [13]. More recent studies recommend a minimum activation of the SCM between 50μV and 80μV in order to elicit a reliable cVEMP measure [11, 13]. Moreover, even though Akin et al. [1] used a similar stimulus, they used a lower intensity than in the present study (90 dBnHL as opposed to 95 dBnHL).
The present study suggests a decline in the relationship between EMG and cVEMP amplitude with normal aging, which is supported by previous observations [2]. Similarly, we observed that aging lead to a reduction of the slope describing the relationship between EMG activity and raw amplitude, with the slope for the younger group (1.5) being twice as steep as the slope in the older group (0.74). Basta et al. [2] described a very similar ratio between the slope for younger adults (0.4527) and older adults (0.2213). We went a step further by calculating the significance of this linear regression, and determined that it was only significant for the younger group. As such, a positive relationship between EMG and raw cVEMP amplitude may only hold true for younger adults when prestimulus EMG activity is within 49.9μV and 150μV. As previously mentioned, caution is needed when interpreting the slope as it may reflect a higher variability due to the limited sample size.
It should be noted that the results of the present study only apply for EMG activity levels in the range between 49.9μV and 150μV. It is possible that different results could be found with lower or higher contraction levels. This particular range was choosen based on the work of Rosengren et al. [13] who showed that the median required contraction strength required to elicit a valid cVEMP response is 48μV.
Overall, the results of the present study demonstrate that the decrease in cVEMP amplitude observed in normal aging is the result of age-related vestibular modification and not EMG activity differences. Moreover, the absence of a significant linear relationship between EMG and cVEMP amplitude in the older group puts into question the validity of using normalization in older adults.