
Abstract
BACKGROUND:
The subjective visual vertical (SVV) test is a sensitive test of vestibular dysfunction that allows the evaluation of otolithic organs; however, with the current method, there are technical and logistical limitations that make the application of this test difficult in the conventional clinic.
OBJECTIVE:
The objective of this study is to assess the effectiveness of detecting vestibular pathology using the SVV via a new screening method.
METHODS:
A consecutive sample of 62 patients with suspected vestibular pathology was included in the study. The patients were clinically diagnosed according to the Barany Society criteria. An exploratory system was designed using a mobile application in Android that detects accelerometer oscillations and involves placing the smartphone on a rotating disk anchored to the wall. All patients underwent a SVV examination using the bucket method and the study test. A cut-off point of the ROC curve was calculated for each test, and its sensitivity, specificity, diagnostic accuracy and probability ratios for detecting vestibular pathology were analysed. The SVV results were compared using the bucket test and the study test.
RESULTS:
We observed significant differences in sensitivity between the two tests: 86.95% for the study test versus 67.4% for the bucket test (p < 0.01). In the ROC curve, an area under the curve of 0.90 was observed for the study test, with a cut-off of 2.43 for a sensitivity of 86.95% and a specificity of 93.75%.
CONCLUSIONS:
SVV testing using a smartphone placed on a rotating disk anchored to the wall offers greater diagnostic accuracy than SVV using the bucket test. Both methods are inexpensive, harmless and easily accepted by patients.
Introduction
Otolithic function is responsible for perceiving the cephalic linear accelerations to which we are constantly exposed via the force of gravity. The neuronal pathway responsible for this representation is the graviceptive pathway, which starts at the utricle and the saccule and semicircular canals and conducts impulses through the vestibular nerve to the vestibular nuclei in the pons area until its decussation in the medial longitudinal fasciculus, then proceeds towards the thalamus to end in multiple projections to the cortex [15, 23].
For the study of otolithic function, vestibular evoked myogenic potential is an option; however, it is an expensive and complex study, so its use is not widespread, and its application is not routine in vertigo queries [8]. The subjective visual vertical (SVV) test is an examination that allows evaluation of the function of the otolithic organs, especially the utricle, as a measure of the verticality perceived by the subject. SVV can be explored using various instruments. Examination using a dome with a light line in a dark chamber is expensive and difficult to apply. Since 2009, the bucket test has been validated as a simpler and more widely applicable SVV test; however, it is influenced by tremors of the examiner and by the difficulty of maintaining position during the examination with decreased accuracy [23, 35]. A variant of this method is the use of a bucket with a smartphone placed at the bottom that performs the test using a mobile application; the effectiveness of this method for distinguishing healthy patients from ill patients in the child population has been demonstrated [3]. A mobile virtual reality system [28] and a computerised system with a screen-patient interface [23] have also been used.
The SVV is a sensitive test of vestibular dysfunction. Different authors have revealed alterations in pathologies considered classically localised at the level of the semi-circular canals, which is why the study of the SVV is currently considered of great interest [2, 34]. Despite this, and due to technical and logistical limitations, SVV is not explored in conventional clinical practice. It is of great interest to study SVV through effective, harmless, fast, simple and economic tests. The main objective of this study is to determine the validity of SVV testing using a mobile application on a smartphone manually anchored to a rotating disk to detect vestibular pathology in routine clinical practice. Furthermore, the incorporation of the device anchorage to a fixed surface could improve the effectiveness of the SVV by suppressing examiner interference.
Materials and methods
Patient
The study included a consecutive sample of 62 patients treated between June and September 2019 at a specific vertigo consultation clinic at regional referral hospital. Patients are referred from primary or specialised care. The patients included in the study were first-time patients who signed informed consent. Patients with severe visual pathology, cognitive disorders and inflammatory otological diseases were excluded.
Patients were studied according to the usual protocol of the unit, and all patients with suspected vestibular pathology were examined with the Video Head Impulse Test (VHIT), and caloric tests were added in cases of suspected Meniere’s disease. We applied Baranny’s criteria as the gold standard for the diagnosis of vestibular pathology. Patients whose anamnesis, physical and/or instrumental examination were compatible with any of the diagnoses established by the Baranny society were categorized as pathological, otherwise it was categorized as normal. [1, 33]. This diagnosis was made before considering the results of the study’s tests.
Our study was approved by the Biomedical Research Ethics Committee of Cádiz.
Subjective visual vertical test
Regardless of the results, SVV was tested blindly by two different examiners. Each examiner performed one of the methods, the bucket test or the smartphone method, in order to ignore the other method results. Both tests were performed on the same day, with a 30 minute “recovery” time to avoid fatigue. The order of assessment was random.
SVV with smartphone method
The mobile application was developed for the Android system. The smartphone used was a Samsung Galaxy A5. The smartphone was anchored to a rotating disk fixed on the wall (Fig. 1) and the examiner rotated the disk clockwise and counter clockwise starting at an inclination of +/– 45° with respect to the vertical. Three measurements were made per side. The test was carried out in dark conditions, with the lights off and in the mobile screen, the patient could only see a red line in a black background to avoid the use of visual cues in the test environment. The patient was seated on a height-adjustable stool, 50 cm apart from the device, with the body and head in a neutral position. No other support was used, in order to avoid proprioceptive perception of spatial orientation. To perform the test, the examiner tells the patients that they will be shown a red line that will be slowly rotating, and asks the patient to indicate when this red line is perceived to be shown as vertical. Then, the examiner turned the disk until the patient notifies the verticality. This study has been performed using the application’s manual functioning mode. In this mode, the examiner rotates the device until the patient indicates to perceive the line as vertical, and at this point, the examiner touches the screen, and the device records the deviation of each movement. However, the device also allows for an automatic assessment mode in which, the examiner has twenty seconds to place the line in the positions notified by the patient. Then, the degrees of deviation from verticality are automatically recorded. The examiner may choose to program the device to perform two or three clockwise or counter clockwise turns. The application shows the angular deviation detected by the smartphone’s accelerometer on the screen. The results, both form manual or automatic modes, are automatically stored in the memory of the application, allowing the results of all examinations performed on the patient to be viewed and recorded elsewhere if necessary. In this study, the test was always performed in a binocular manner, averaging the results of 3 measurements of each movement [10, 25].

The smartphone anchored to a roating disk fixed on the wall.
The device used for the bucket test was made according to the instructions of Ferreira [13]. While the patient is sitting on a bench, he first places the face into the bucket and then the examiner performs three rotations clockwise and three counter clockwise from +/– 45° with respect to the vertical. The examiner records the degrees of deviation of each movement and the average of three measurements clockwise and counter clockwise is used as the final result” [10].
Statistical analysis
After the data were inspected and cleaned, statistical analysis was carried out using SPSS v25.0. First, a univariate descriptive study was performed by calculating frequencies for categorical variables and by determining central and dispersion measures and calculating extreme values (outliers) for quantitative variables.
To evaluate the study method’s effectiveness in differentiating between healthy and pathological patients, we first calculated a cut-off point using the ROC curve to dichotomise the responses, healthy or pathological, and analysed its sensitivity, specificity, diagnostic accuracy and probability ratios to detect vestibular pathology, regardless of cause. Subsequently, we evaluated the degree of agreement between the two tests for detecting vestibular pathology using the kappa index and the absolute agreement between both tests, using the intraclass correlation coefficient (ICC) in a mixed factor model with 95% confidence interval.
To categorically analyse whether their higher frequency of alteration of the test was related to the topographic or clinical diagnosis, we used the chi-square test.
Results
Demography and clinical diagnosis
Our study was conducted in 62 patients, 39 women (62.9%) and 23 men (37.1%), with a mean age of 48.64±17.50 years and a range 6 to 79 years. Forty-six patients (74.2%) had vestibular pathology, 40 (64.5%) had peripheral pathology, and 6 (9.7%) had central pathology. Sixteen patients (25.8%) did not present vestibular pathology (Table 1).
Demography information, frequency (%) vestibular patohology, topographic diagnosis and clinical diagnosis
Demography information, frequency (%) vestibular patohology, topographic diagnosis and clinical diagnosis
VPB: Benign paroxysmal positional vertigo. PPPD. Persistent Postural Perceptual Dizziness.
Regarding the ROC curve, an area under the curve of 0.90 was observed for the mobile application method, with a cut-off of 2.43 for a sensitivity of 86.95%, a specificity of 93.75% and a diagnostic accuracy of 88.71%. The next cut-off point of 2.50 decreased the sensitivity to 84.8 while maintaining the same specificity (Fig. 1). For the bucket method, an area under the curve of 0.82 and a cut-off point of 2.42 obtained a sensitivity of 67.39% and a specificity of 93.75%, with a diagnostic accuracy of 74.2%. The cut-off value of 2.54 decreased the sensitivity to 66.52% while maintaining the same specificity (Fig. 2).
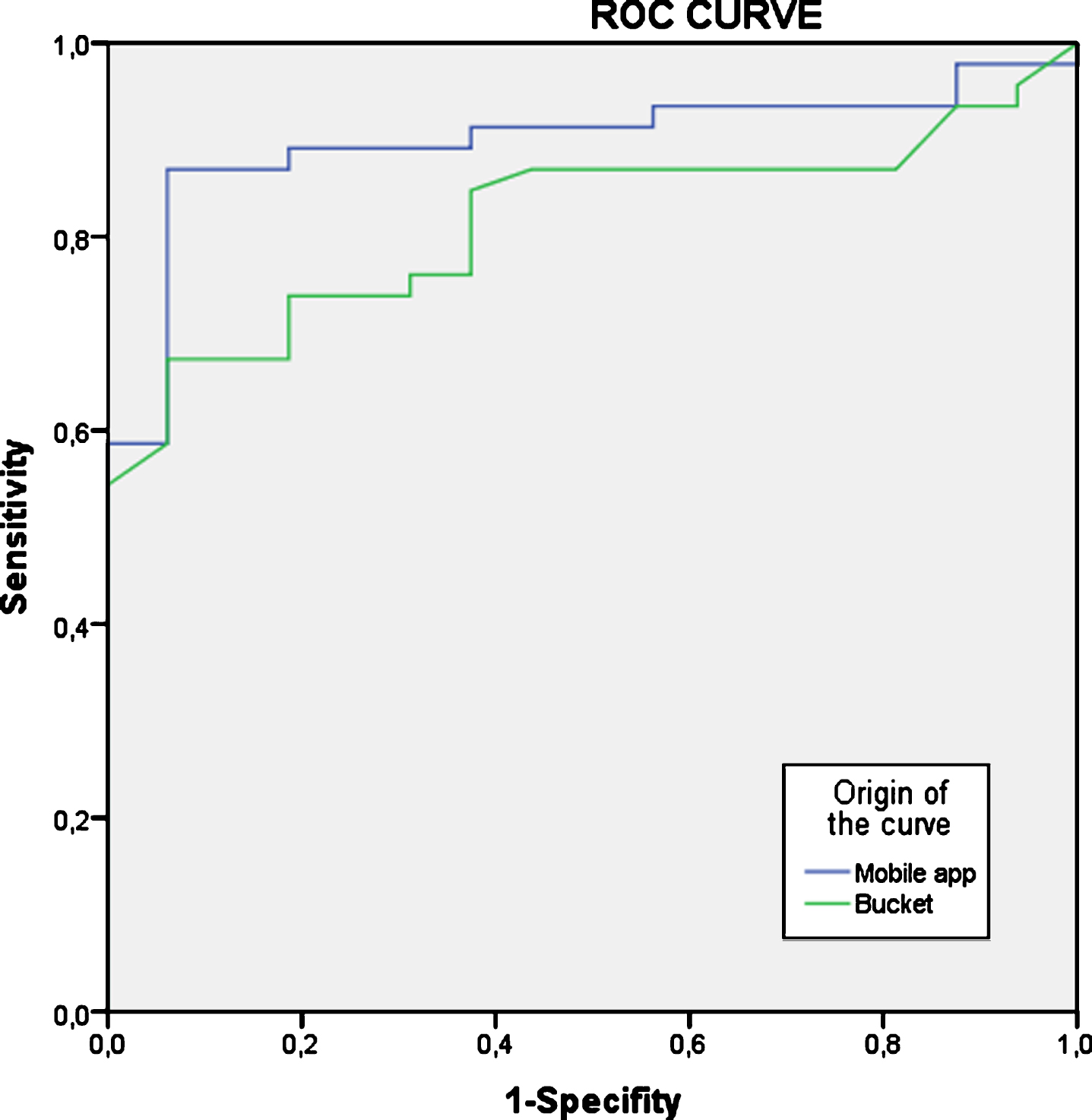
ROC Curve. AUC = Area under the curve. AUC bucket =0.82. AUC mobile application = 0.9; P = 0.14.
Taking as reference the optimal measures of the ROC curve, the sensitivity, specificity, positive likelihood ratio, negative likelihood ratio and accuracy of the mobile application was 86.95%, 93.75%, 13.9, 0.14 and 88.71% respectively. The sensitivity, specificity, positive likelihood ratio and negative likelihood ratio of the bucket was 67.4%, 93.75%, 10.8, 0.35 and 74.2% respectively. There was a significant difference between the two test methods in their sensitivity and accuracy (McNemar test) and negative likelihood ratio (regression model approach proposed by Gu and Pepe) [16] (Table 2).
Comparison between the mobile application and the bucket diagnostic tests
AUC = Area under the curve. *Sensitivity, Specificity and Accuracy (McNemar Test), LR (Regression model approach proposed by Gu and Pepe) [14]. AUC (DeLong et al.)[9].
The comparison between the mobile application and the bucket results compared to the gold standard are shown in Table 3. The concordance between the two tests was 79%, with a Kappa index of 0.58, which implies moderate concordance. The intraclass correlation coefficient was 0.91 (0.80 to 0.95), confirming an excellent absolute agreement.
Comparison between the mobile application and the bucket results compared to the gold standard
With respect to the topographic and clinical diagnoses, the results are shown in Table 4. There are no significant differences in the sensitivity of the app to detect central or peripheral pathology (87.5 versus 83.3). Similarly, there are no significant differences in sensitivity with the bucket method (67.5 versus 66.7) (Table 4).
Positive results in patients with vestibular pathology
In no case did the examination have to be interrupted; both methods were very well tolerated by the study population. The duration of the test was always less than four minutes.
Our study shows that SVV testing performed through a mobile application on a smartphone anchored to a rotating support can simplify and perfect the SVV testing technique as this testing method is economical, simple to perform, rapidly administered and easily accepted by patients. The data from our study indicate that the mobile application test can be used to detect or rule out the existence of vestibular pathology in a high percentage of patients.
The selection of a consecutive sample of study patients in a real-world scenario reflects the appropriateness of the sample, since the healthy participants were referred from primary or specialised care with unconfirmed but suspected vestibular pathology; to date, mobile application studies have been designed using cases and controls, with the biases that patient selection may imply.
The most frequent pathologies detected in our study (persistent perceptual-postural dizziness, Meniere’s disease, benign paroxysmal positional vertigo (BPPV), vestibular neuritis and vestibular migraine) guarantee the applicability of the mobile application testing method since these are the most frequent diagnoses in vestibular pathology in any environment.
Due to the characteristics of the study patients and the scheduled consultation, there were no cases of urgent pathology, and it is expected that the capacity of the present testing method to detect urgent issues at a primary care consultation is even greater than that demonstrated in the present study. Another possible bias is the delay in being referred from or cited by primary care, which can affect the detection of patients with BPPV in spontaneous remission or with vestibular neuronitis in the recovery phase. All these possible biases decrease the ability to detect pathology, which gives greater validity to our results. Although the applicability of the study test to acute patients should improve sensitivity, which depends on the prevalence of different degrees of disease in the patient group, we believe that the percentage of patients who would benefit from such an examination would probably decrease, since in this phase, the clinical examination results are the main interest.
Fixing the smartphone to a rotating disk reduces factors that can cause inaccuracy. The bucket test is simple and inexpensive; however, it is influenced by tremors of the examiner and by the difficulty of maintaining position during the examination [23], which decrease accuracy. In addition, in paediatric patients, the application of this test method is occasionally difficult, and test acceptance is reduced [23]. The SVV test performed according to the procedure described in our study, eliminates the previously mentioned factors; additionally, it uses a cell phone device, which children are familiar with and may not perceive as a threat. Furthermore, children may find challenging, uncomfortable, invasive and/or intimidating to have to place their face into the bucket (a narrow and dark space), so we believe this new tool could be better accepted and applied in this particular population group. In addition, the automatic generation of test results by the accelerometer avoids with subjectivity that could affect the result. In our study we only included 4 patients under 12 years old, larger study would be needed to evaluate the method acceptance in this population.
Studies carried out by other authors placing the smartphone at the bottom of the bucket do not solve the problems mentioned with this test, but they do show its ability to detect peripheral vestibular pathology in children [3].
Our study, in agreement with those of other authors, found frequent alteration of the SVV test results in patients with the most common vestibular pathologies: persistent postural-perceptual dizziness, diagnosed or probable Meniere’s disease, diagnosed or probable BPPV, vestibular neuritis and vestibular migraine [6].
Several authors have confirmed the validity of SVV testing for monitoring certain vestibular pathologies, especially in BPPV [6, 26], vestibular neuronitis [5, 30], Meniere’s disease [11, 18] and vestibular migraine [2], correlating the restoration of the SVV with the recovery of the disease. Our study was conducted with a different objective and included patients at different stages of disease progression; no repeated measures were performed for evaluation purposes.
Although in quantitative analysis the absolute agreement measured by the ICC was excellent, the quantitative differences in the results, to characterize it as normal or abnormal might be minimal. This explains how in our categorical analysis, rendered only a moderate concordance between the two SVV tests, since the greater sensitivity of the mobile application prevented a greater concordance.
We must mention as a limitation of this study that the SVV with the bucket test and the smartphone application were performed without a pre-established order and therefore, it was not the same for each patient, we didn't randomize it. However, the examiners waited 30 minutes to perform each method in order to avoid the fatigue.”
Given the characteristics described and the results of our study, SVV testing through the mobile application is useful as a screening test to detect vestibular pathology, in line with some reports [3, 6]. Other authors have found discrepancies in the usefulness of SVV tests, which may be due to the test method used and the study sample selected [7].
Conclusions
SVV testing through a mobile application on a smartphone mounted on a rotating disk anchored to the wall offers great diagnostic accuracy to detect vestibular pathology, surpassing the results of the bucket method.
The test developed in our study is an inexpensive, harmless examination that is easily accepted by patients.
Due to its diagnostic accuracy, economy, harmlessness, rapid administration and acceptance by patients, we consider this SVV test a valid method for screening for vestibular pathology.
Compliance with ethical standards
Conflict of interest
All authors have no conflicting interest to report
Ethical approval
Our study was approved by the Biomedical Research Ethics Committee of Cádiz. Informed consent was obtained from each individual participant.