
Abstract
Abstract.
From a biomechanical point of view, the process of Benign paroxysmal positional vertigo (BPPV) includes 2 fluid¯solid coupling effects: the interaction between particles and endolymph and the interaction between endolymph and cupula. The interaction between the canaliths and the wall would affect the coupling effects. This study aimed to investigate the entire process of cupula motion caused by canaliths motion and the influence of canalith particles composition. A biomechanical numerical model was established to simulate the canalith falling process and study the influence of canalith diameter, number, and initial falling position on cupula movement. Simultaneously, the relationship between cupula displacement and the nystagmus signal was analyzed in BPPV patients. The results revealed that the particle velocity was proportional to the particle diameter. The pressure difference between the two sides of the cupula was directly proportional to the canalith diameter and number. The degree of vertigo was positively related to the slow angular velocity of the nystagmus and, therefore, reflected canalith number and diameter. The BPPV latent period and vertigo duration were inversely related to particle diameter. Thus, the number of particles, particle radius, and initial falling position affected cupula movement, which was reflected in the nystagmus.
Keywords
Introduction
The vestibular structure of the human inner ear is directly related to balance. BPPV is caused by a mechanical dysfunction of the vestibular system in the inner ear. Canaliths can disturb the normal operation of the semicircular canals. When the head is in a specific position, the canalith moves owing to gravity and drives endolymph movement in the semicircular duct, leading to cupula displacement. The contradiction between the motion information perceived by the human eye and the inner ear can ca-use dizziness and simultaneously induce nystagmus [15]. From a biomechanical point of view, this process includes two fluid-solid coupling effects: the interaction between particles and the endolymph and the interaction between the endolymph and cupula. BPPV usually occurs in the posterior semicircular duct because it is positioned lower than the other two semicircular ducts [1, 27]. Currently, there is no effective method to directly detect canalith movement or cupula displacement. A common clinical BPPV diagnostic method involves the detection of information regarding nystagmus using electronystagmography. The angular velocity of the nystagmus is proportional to cupula displacement [16, 19]. Previous studies have investigated the pathogenesis of BPPV from a biomechanical perspective. Hain et al. [6] established a mathematical model of the semicircular duct to study the pressure difference between the two sides of the cupula when canaliths move in the semicircular duct. The pressure difference between the two sides of the cupula is small when the canalith moves in the ampulla; this is considered the latent stage. When the canalith enters the narrow duct, the pressure difference begins to increase; thus, the volume displacement of the cupula increases and nystagmus begins to appear. The dispersion of a clump of canalith creates more nystagmus. Rajguru et al. [17] established a three-duct mathematical model to study the motion of the cupula when canalith particles move in the duct. Their model predicts duct responses to the diagnostic Dix-Hallpike maneuver [22]. The latency and response magnitudes obtained were consistent with the clinical observations. Zdravkovic [26] established a parametric model and a real geometric model of the membranous semicircular duct of patients to study the distribution of endolymphatic velocity, sh-ear force on the wall, and force on the crest. Other researchers [5, 13] established mathematical models of BPPV to study the interaction between particles and fluids and determine the mechanism of canalithiasis. Boselli [2] established a computational model to quantitatively analyze fatigue in BPPV patients. Additionally, many studies have been performed in animal models of BPPV [9, 21].
To further study BPPV, it is essential to establish a three-dimensional finite-element model of the vest-ibular system to simulate the entire process of cupula motion caused by canalith motion. In the present study, a three-dimensional finite-element numerical model of the membranous semicircular duct was established, based on adult inner ear imaging data, to determine the influence of particle number, particle radius, and initial falling position on cupula motion. Cupula motion was compared with the nystagmus signal, as assessed by electronystagmography, to st-udy their relationship. The results presented herein may help to obtain more information about the condition during clinical diagnosis.
Materials and methods
According to the structural imaging data of the membranous semicircular duct in the right inner ear of a healthy volunteer (female, 67 years, no history of ear disease, no abnormal anatomical structure) pro-vided by [8], a three-dimensional model of the mem-branous semicircular duct was reconstructed as shown in Fig. 1(a). The model comprised three semicircular ducts and three cupula. As BPPV mainly involves the posterior semicircular duct, only the posterior semicircular duct model was extracted to study the movement of the canalith in the duct. These results can also be applied to study the horizontal and upper semicircular ducts. The posterior semicircular duct model was meshed using Workbench software, as shown in Fig. 1(b). The membranous semicircu-lar duct was represented as a fluid area, divided by 56,517 tetrahedral elements and 12,789 nodes. The cupula was represented as a solid area divided by 6,837 tetrahedral elements and 1,724 nodes. The membranous structure of the semicircular duct was assumed to be a rigid boundary, the endolymph was assumed to be an incompressible Newtonian fluid, and the cupula was assumed to be a linear elastic structure because its deformation is much smaller than its original size. The material parameters of the endolymph and canalith are shown in Table 1. The ANSTS-Workbench V14.5 was used to solve the fluid-structure coupling process in the BPPV onset period. The ANSYS FLUENT 14.5 is used to calculate the canalith motion and the micro flow of the endolymph. The “transient structural” package is used to calculate the cupula displacement caused by the micro flow of endolymph. The two modules work together to complete the fluid–solid coupling calculation. To study the influence of the semicircular duct structure on BPPV, a regular circular duct model with the same diameter, D, as the ampulla of the semicircular duct was established and meshed, as shown in Fig. 1(c). The cupula motion, caused by canalith movement in the circular duct, was simulated and compared with the results of the real model.
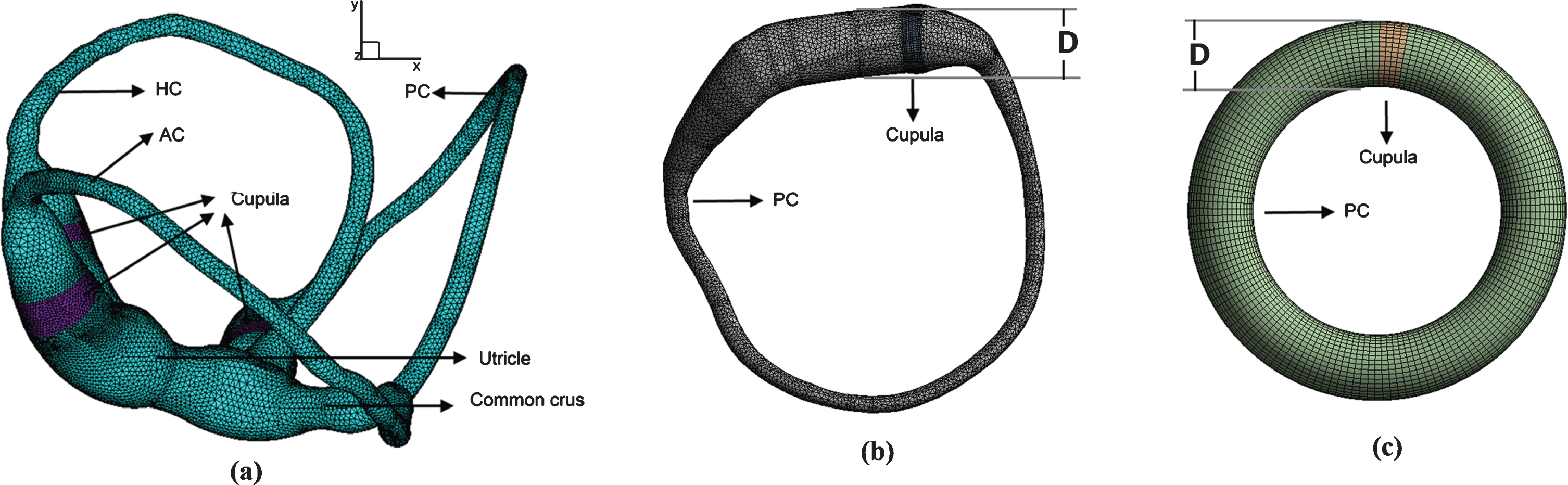
A three-dimensional model of the membranous semicircular duct. (a) Numerical model of the three ducts. (b) Numerical model of the posterior semicircular duct. (c) Numerical model of a duct with a circular section.
Physical parameters for BPPV
In this study, the number of canalith particles was varied from 1 to 27, their diameter was varied from 10 to 90μm, and the shape factor was varied from 0.1 to 1. The shape factor is described as the surface area ratio of particles with the same volume
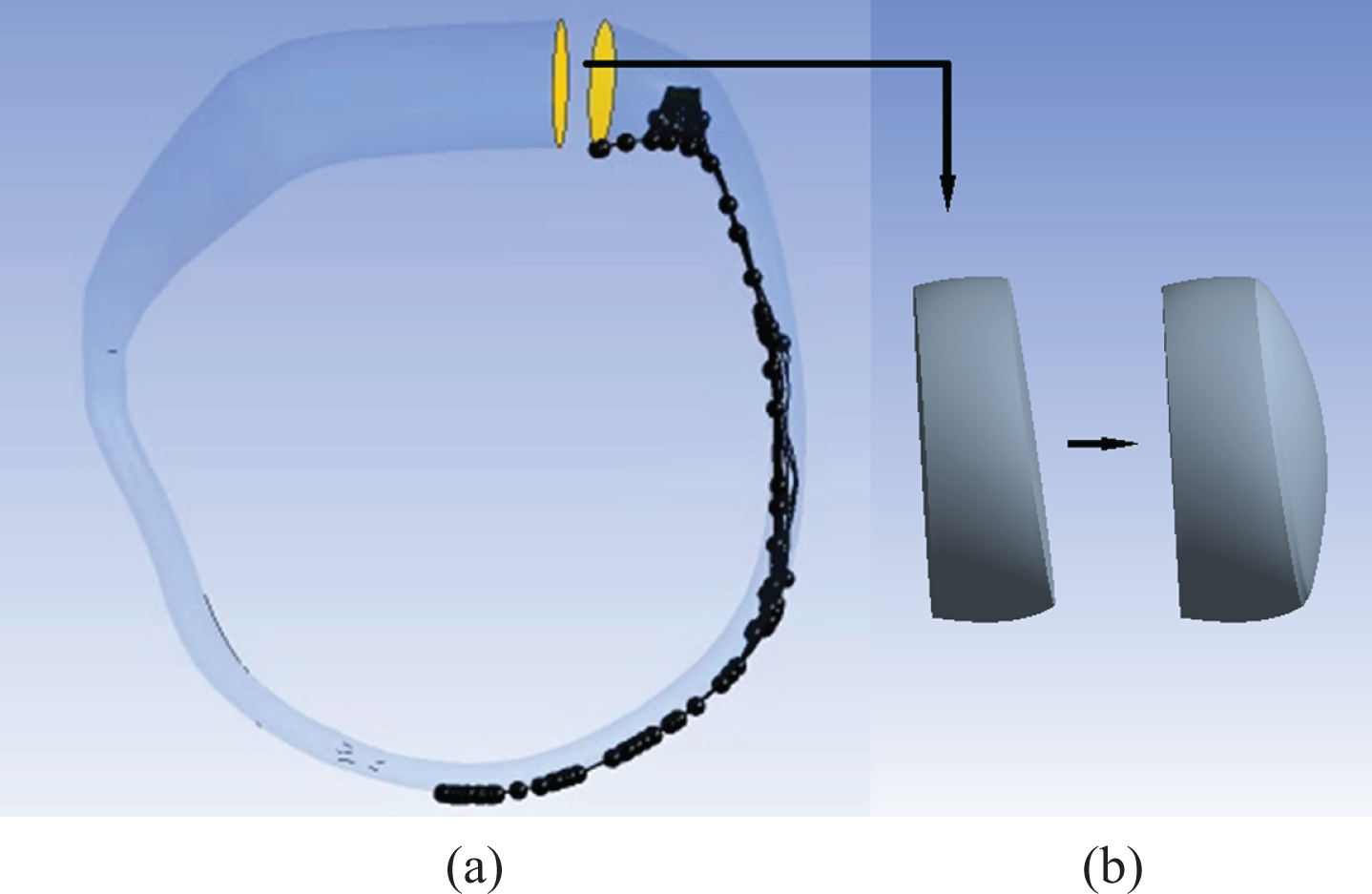
Fluid-solid interaction of the canaliths, endolymph, and cupula (a) Canaliths fell from the ampulla and moved in the endolymph. (b) Owing to the action of the endolymph, the cupula was displaced.
The governing equations of the fluid zone include continuous equation (1) and dynamic equations (2). The governing equations of the solid zone include cupula equilibrium (3). Equation (4) represents the equilibrium equation of the canalith particles moving at a uniform speed in the endolymph. Equation (5) represents the relationship between the drag force and velocity of particles. Equations (4), (5) are simplified equations to illustrate the influence of some main forces, such as force of gravity, buoyancy force, and drag force, which play a major role in the whole process of canaliths movement. The nystagmus is caused by the deviation of the cupula due to the pressure difference between the both sides of the cupula, and the pressure difference is not only related to the influence of canaliths, but also related to the shape of duct. Equation (6) represents the relationship between the pressure difference and the shape of duct [19]. Equations (7)-(9) are the continuity conditions of force, displacement and velocity at the fluid–solid coupling interface, respectively.
In equations (1)–(2), v represents the fluid vector velocity, ρ
f
represents the fluid density, σ
f
represents the stress tensor, μ represents the viscosity of the endolymph, p represents the pressure and f
f
represents the volume force.
ρ
s
is the density of the cupula, d is the cupula displacement, σ
s
is the stress tensor, and ɛ is the stain tensor. In the above symbols, the subscripts f and s indicate the fluid and solid zones, respectively.
F
g
is the particle weight, F
b
is the particle buoyant force, F
d
is the total drag force of the fluid to the particles, R is the radius of the canalith particles, u is the velocity of the canalith movement, ρ
p
is the density of the canalith, and ρ
f
is the density of the endolymph. When the particle falling speed increases to a certain extent, the sum of the total drag and buoyancy forces is equal to the force of gravity, as shown in equation (4), and the particles then move at a uniform speed in the fluid, as shown in formula (5). In equation (6), ΔP is the pressure difference between both sides of the cupula, b
d
is the radius of duct, r
p
is the radial distance of the particle from the duct centerline, and the vector epoints along the (local) duct centerline.
At the interface between cupula and endolymph, each point’s force, displacement, and velocity are the same. d f is the displacement of the endolymph zone at the coupling boundary, d s is the displacement of the cupula zone at the coupling boundary, n f is the normal direction of the boundary of the endolymph zone, and n s is the normal direction of the boundary of the cupula zone.
The boundary conditions at the duct wall were defined as follows: the duct wall of the model was assumed to be rigid. A no-slip velocity condition (V = 0) was applied to the wall.
Numerical analysis of BPPV with different parameters
The influence of canalith number, radius, and initial falling position on cupula displacement was analyzed using Fluent 14.5 software. BPPV occurs after the position of the patient’s head changes and a latent period. Therefore, the semicircular duct was fixed to study canalith movement caused by gravity. When the patient moved from the sitting to the sup-ine position, the canaliths began to fall from the ampulla owing to gravity. The initial movement of canaliths in the membranous labyrinth was slow. As the force of gravity on the canaliths was greater than the endolymphatic buoyancy force, its falling speed gradually accelerated and the drag force of the end-olymph increased, as shown in equation (5). When the canaliths falling speed reached a certain value, the sum of the buoyancy and drag forces from the endolymph was balanced with the force of gravity on the canaliths, as shown in equation (4); subseque-ntly, the canaliths moved at a uniform speed. When canaliths fell onto the outer duct wall, they slid along the outer duct wall and slowed down to a resting position. Some canaliths first fell onto the inner duct wall, then slid down the inner wall, and continued to move in the endolymph.
Cupula displacement was related to the pressure difference on both sides of the cupula, whereas the pressure difference was related to canalith speed. When the canalith speed was low, the interaction fo-rce with the endolymph was small, the pressure difference (ΔP) on both sides of the cupula was also small, and the cupula displacement was minor. When the canalith speed increased, the interaction force increased, which increased the ΔP and cupula displacement. When the canaliths made contact with the outer wall of the duct, their velocity decreased, resulting in a decrease in ΔP. The Cupula displacement then decreased toward equilibrium. Figure 3 shows the variation in ΔP on both sides of the cupula and the cupula displacement with time caused by the movement of a single 30-μm-diameter canalith in the semicircular duct. The ΔP and cupula displacement curves were relatively similar, being smaller at the initial moment and then increasing with time, reaching a peak value at approximately 6 s, and then gradually decreasing to zero.
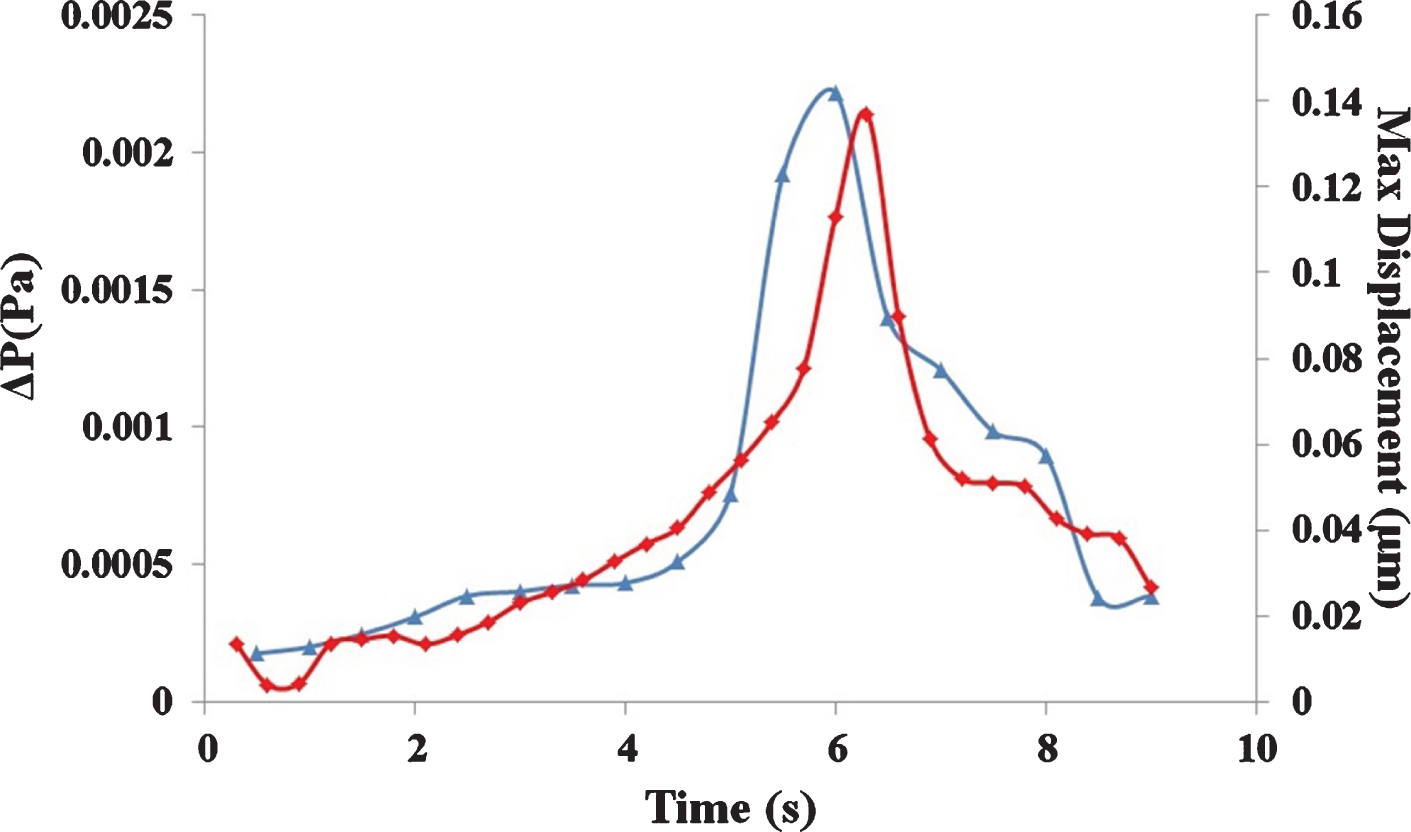
Variation in cupula displacement and the pressure difference (ΔP) on both sides of the cupula with time, caused by the movement of a single canalith with a 30-μm diameter in the semicircular duct.
The movement of canaliths with different diameters had different effects on the endolymph and cupula displacement. Figure 4 shows the cupula displacement with time caused by the movement of single canalith particles with different diameters in the duct. Larger canalith diameters resulted in larger peak cupula displacement values, shorter times required to reach the peak value, and shorter cupula movement times. Canaliths with larger diameters fell faster in the endolymph. Canaliths with a 10-μm diameter fell for more than 40 s. Canaliths with a 30-μm diameter fell for approximately 9 s, whereas those with a 90-μm diameter fell for approximately 2 s.
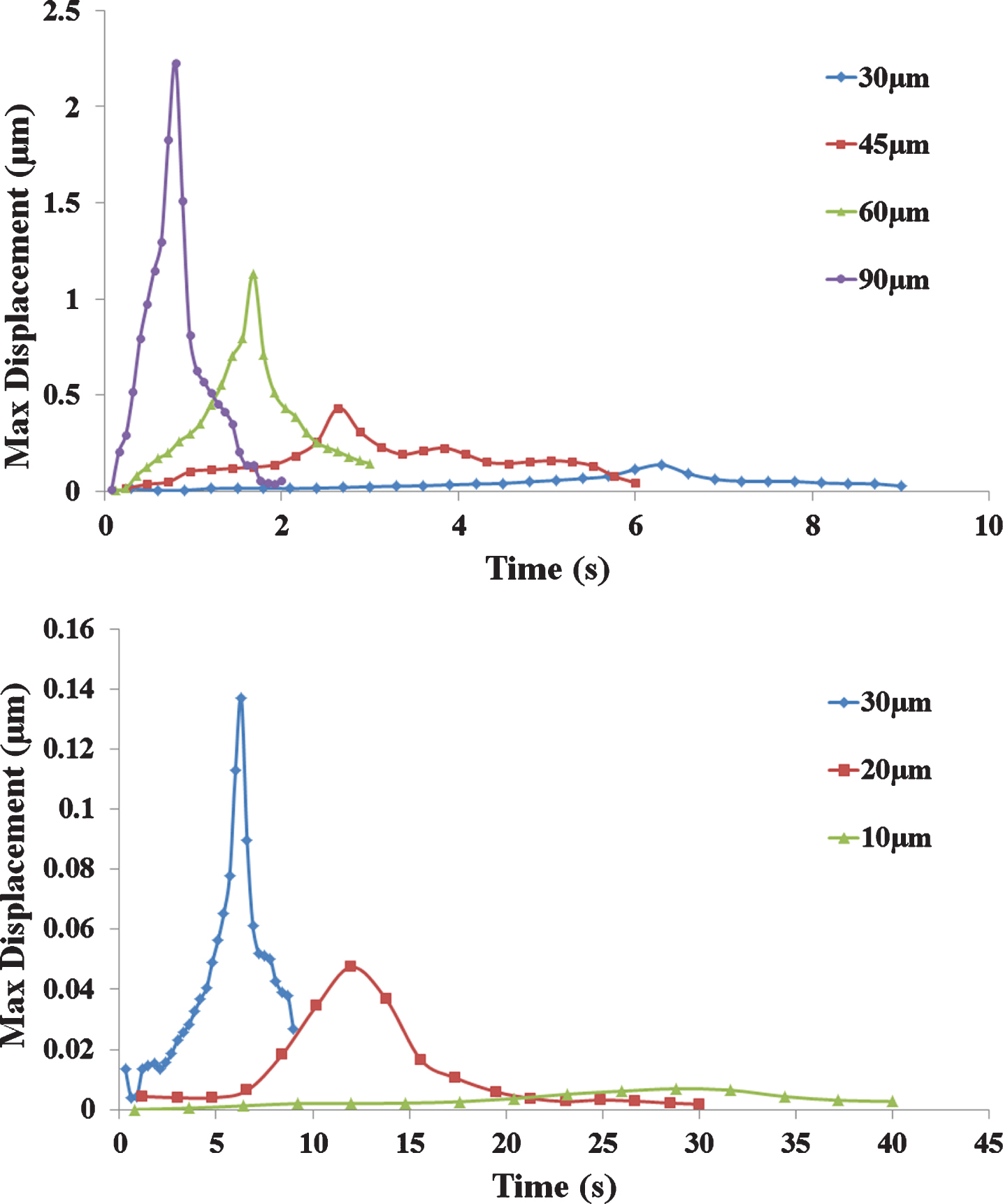
Cupula displacement caused by the movement of a single canalith with different diameters in the semicircular duct.
Considering the influence of canalith number, the particle diameter was set as 30μm and the particle nu-mber was set as 1, 8, and 27. Figure 5 shows the cupula displacement curve caused by the movement of 1, 8, and 27 canaliths in the endolymph. As the nu-mber of canaliths increased, cupula displacement was greater, but the time to reach the peak displacement value decreased. The time to reach the peak cupula displacement value was approximately 6 s and 5 s for 1 and 27 canaliths, respectively. Under the condition of the same total mass (1μg), the influence of particles with diameters of 90, 60, and 30μm on cupula displacement was compared. It can be seen from Fig. 5 that the total duration of falling of small diameter particles is longer, and the displacement of the cupula caused by small particles is larger than that caused by large particles.
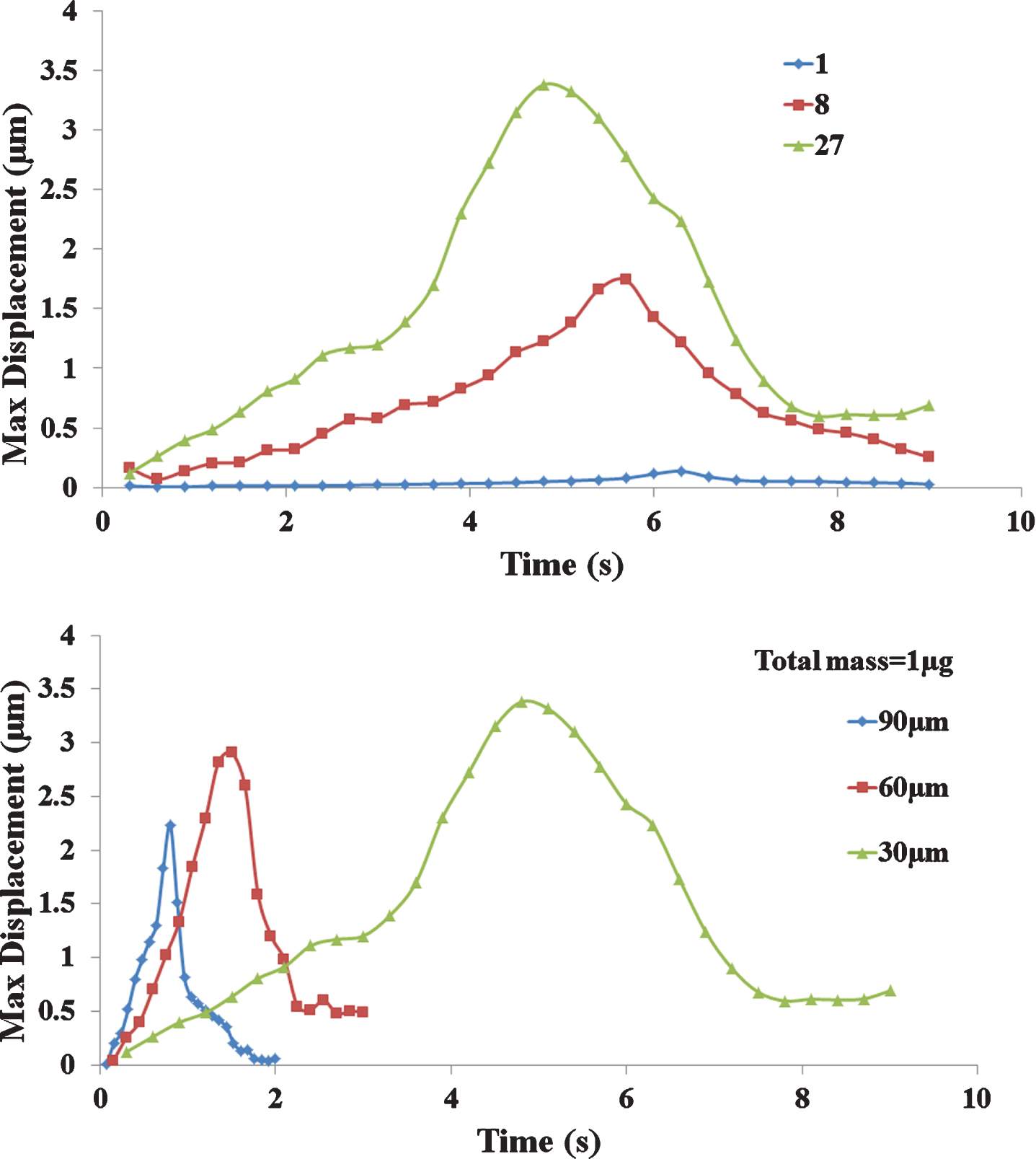
Cupula displacement caused by the movement of different numbers of canaliths in the semicircular duct.
The shape of the membrane labyrinth of the semicircular duct also affected the cupula response to canalith movement. Figure 6 shows a comparison of the cupula displacement caused by a single 30-μm-diameter canalith moving in a real semicircular duct and in a circular duct of equal diameter. There was significantly less cupula displacement caused by canalith movement in the equal-diameter circular duct than in the real semicircular duct. The initial cupula displacement was slightly greater than the displacement over the subsequent few seconds, which may be because the canalith was initially located relatively close to the cupula. In the circular duct, the time to reach peak cupula displacement was prolonged to approximately 7 s.
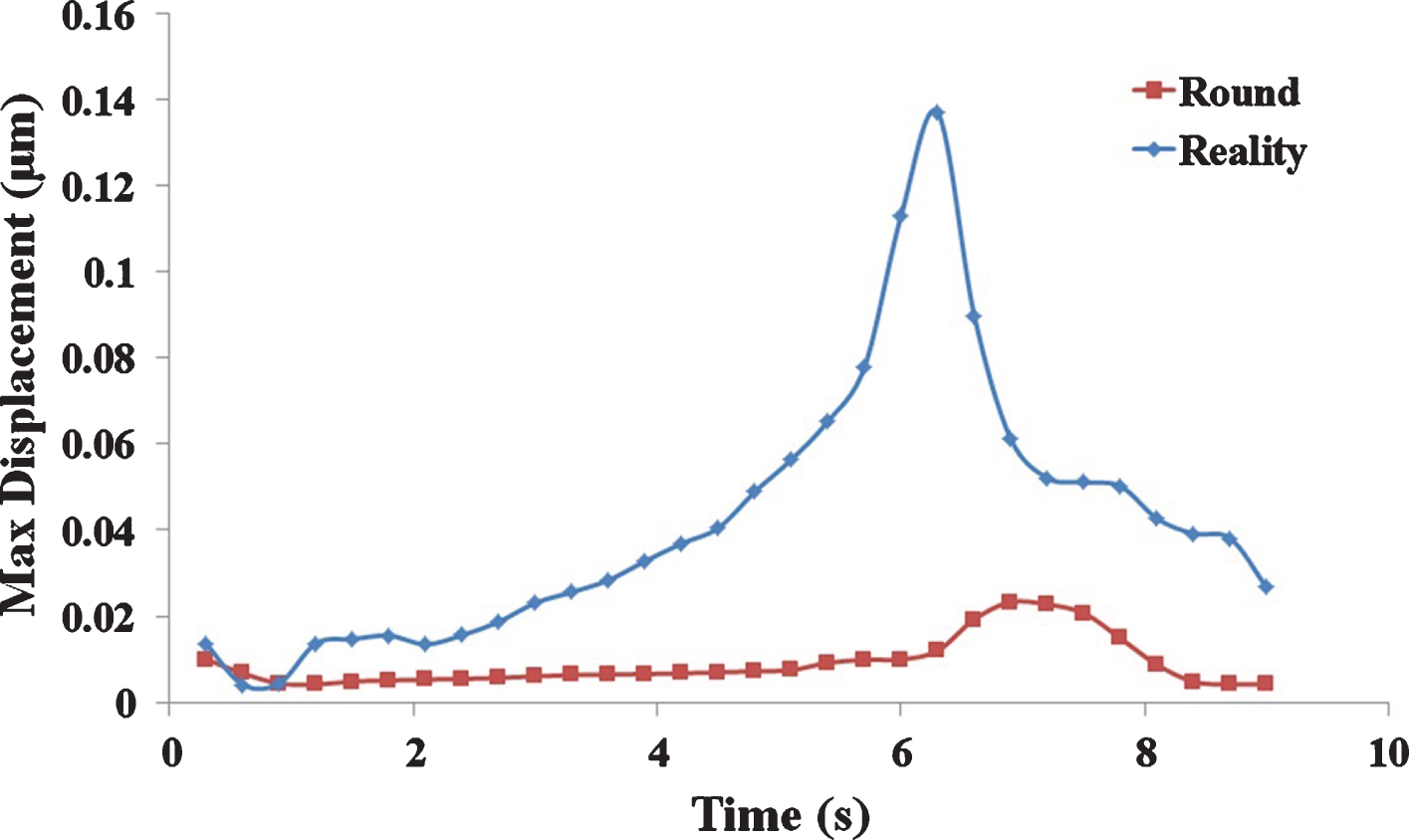
Influence of the membrane labyrinth shape of the semicircular duct on cupula displacement caused by a single canalith of 30-μm diameter.
Canaliths have elliptical shapes. Therefore, the canalith shape parameter was adjusted to study the influence of canalith shape on cupula displacement (Fig. 7). The previously calculated shape factors of the canaliths were all 1, indicating a circular shape. The canalith shape factor was then adjusted to 0.5, 0.1. With the decrease in the shape factor, the canalith became more slender and the peak cupula displacement value decreased slightly, but the time to reach the peak value and the duration of canalith motion in the semicircular duct significantly increased (Fig. 7).

The influence of canalith shape on cupula displacement.
Figure 8 shows the effect of different body positions on cupula displacement. When moving from the sitting to supine position, canaliths fell from the ampulla; when moving from the supine to sitting position, canaliths fell from the duct. The time taken to attain the peak value was more when canaliths fell from the ampulla than when they fell from the tube (Fig. 8). However, the initial cupula displacement was less when the canaliths fell from the ampulla.
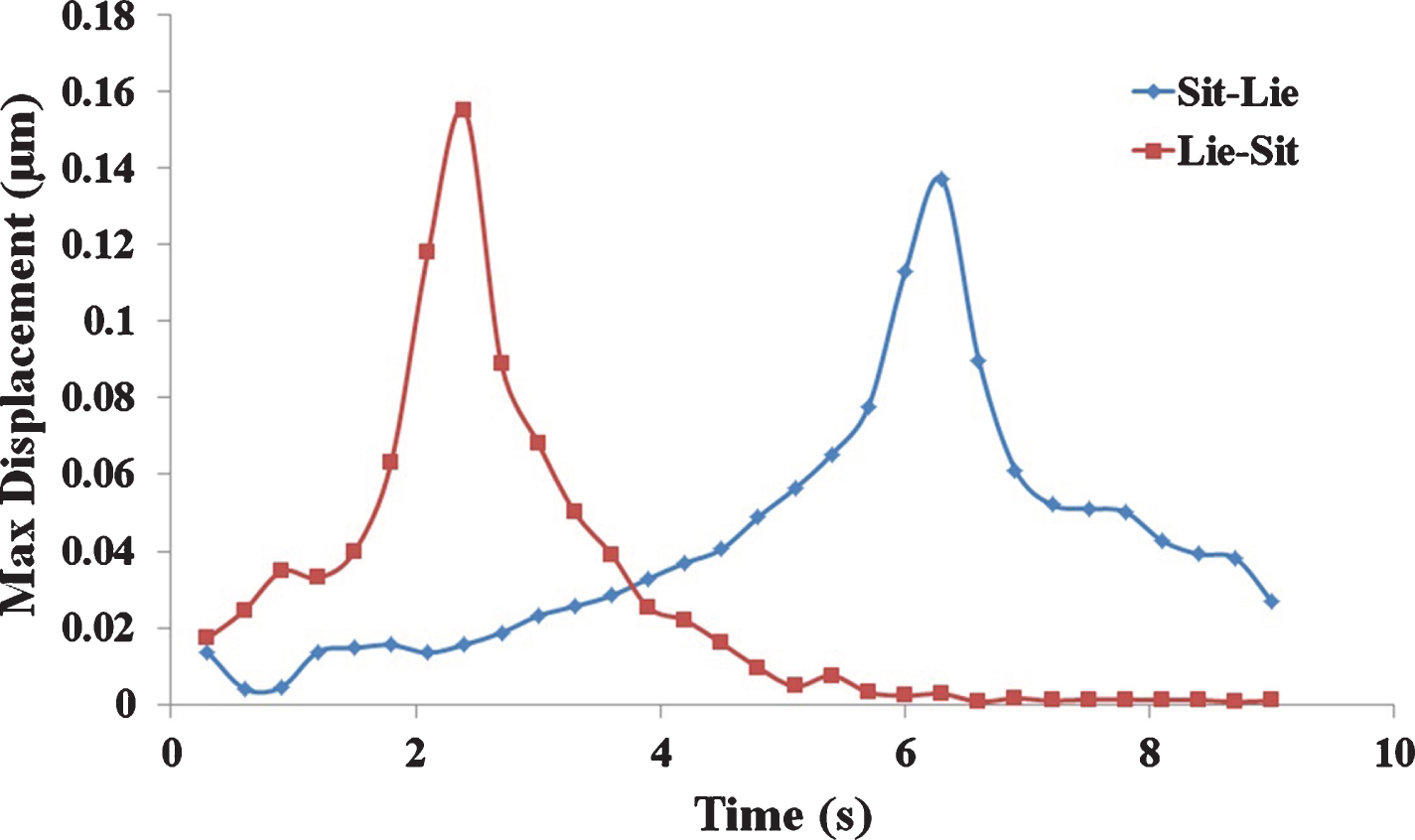
The effect of different body positions on cupula displacement.
A nystagmus test was performed on patients with BPPV to understand nystagmus at disease onset (Fig. 9). The slow angular velocity in the images was extracted to study the eye movement characteristics of BPPV patients. Figure 10 shows a slow angular velocity curves of a typical nystagmus in a patient with BPPV. The posterior semicircular duct was the affected duct when the patient moved from the sitting to the supine position. Weak nystagmus began to appear in the early stage, but the slow angular velocity was generally less than 5 °/s, and the patient did not experience vertigo. At approximately 13 s, the slow angular velocity suddenly increased to approximately 30 °/s, and the patient experienced strong vertigo. From 23 s to 34 s, the patient closed his eyes owing to excessive vertigo, and nystagmus was not observed. The intense nystagmus ended after approximately 40 s, but weak nystagmus was detected, wit-hout vertigo. During the entire process, the nystagmus was very irregular, with the slow angular velocity of approximately 20–40 °/s, the highest to 70°/s, and the amplitude of variation was large.

Nystagmus in BPPV patients.
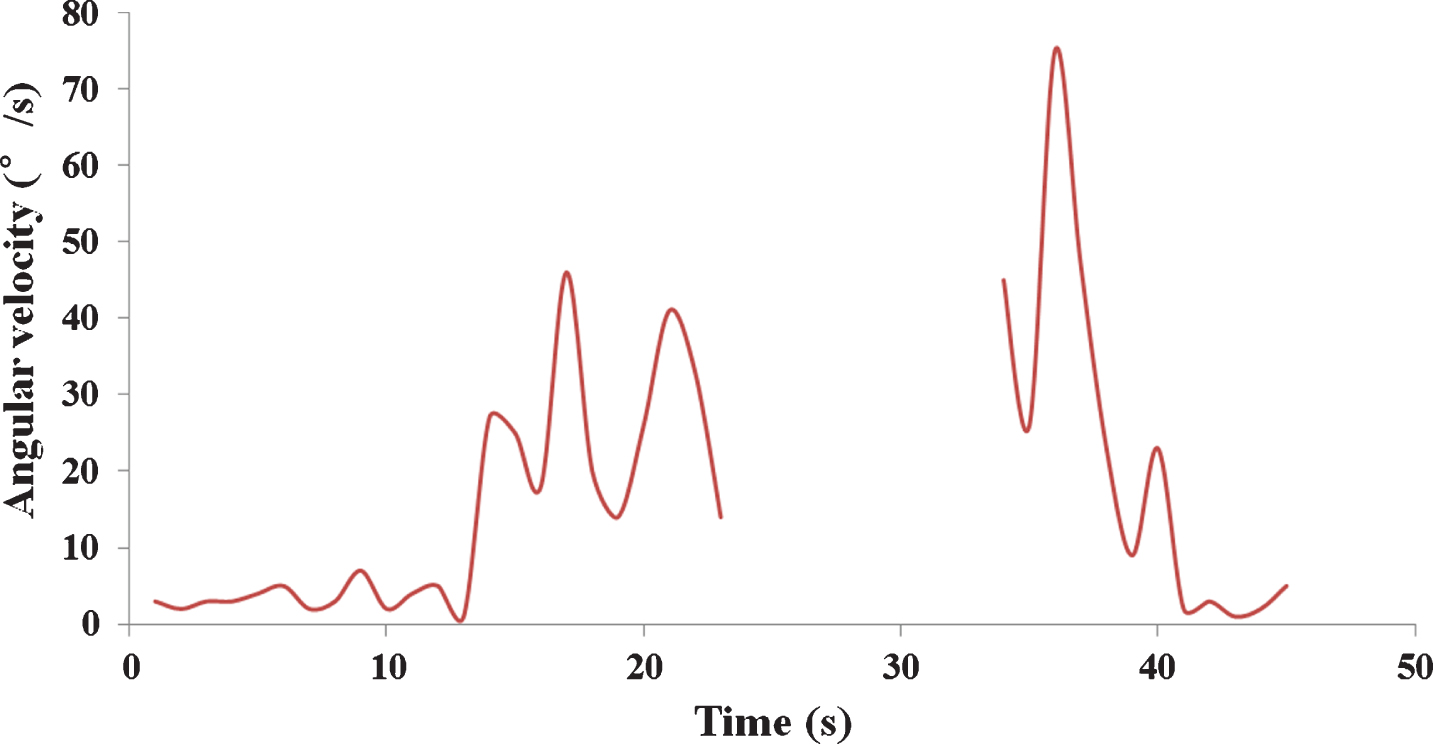
Slow nystagmus angular velocity curves of the nystagmus in a BPPV patient when moving from the sitting to supine position.
Figure 11 shows the slow angular velocity curves of nystagmus of a patient with BPPV when moving from a supine to sitting position. The posterior semicircular duct was the site of onset. As the patient sat up, an intense nystagmus began, with a duration of approximately 10 s. The slow angular velocity of the nystagmus was approximately 20 °/s, but it reduced to less than 10 °/s after 10 s. Electronystagmography data from other BPPV patients showed different latencies, durations, and slow angular velocities. However, they were all directly related to canalith movement.
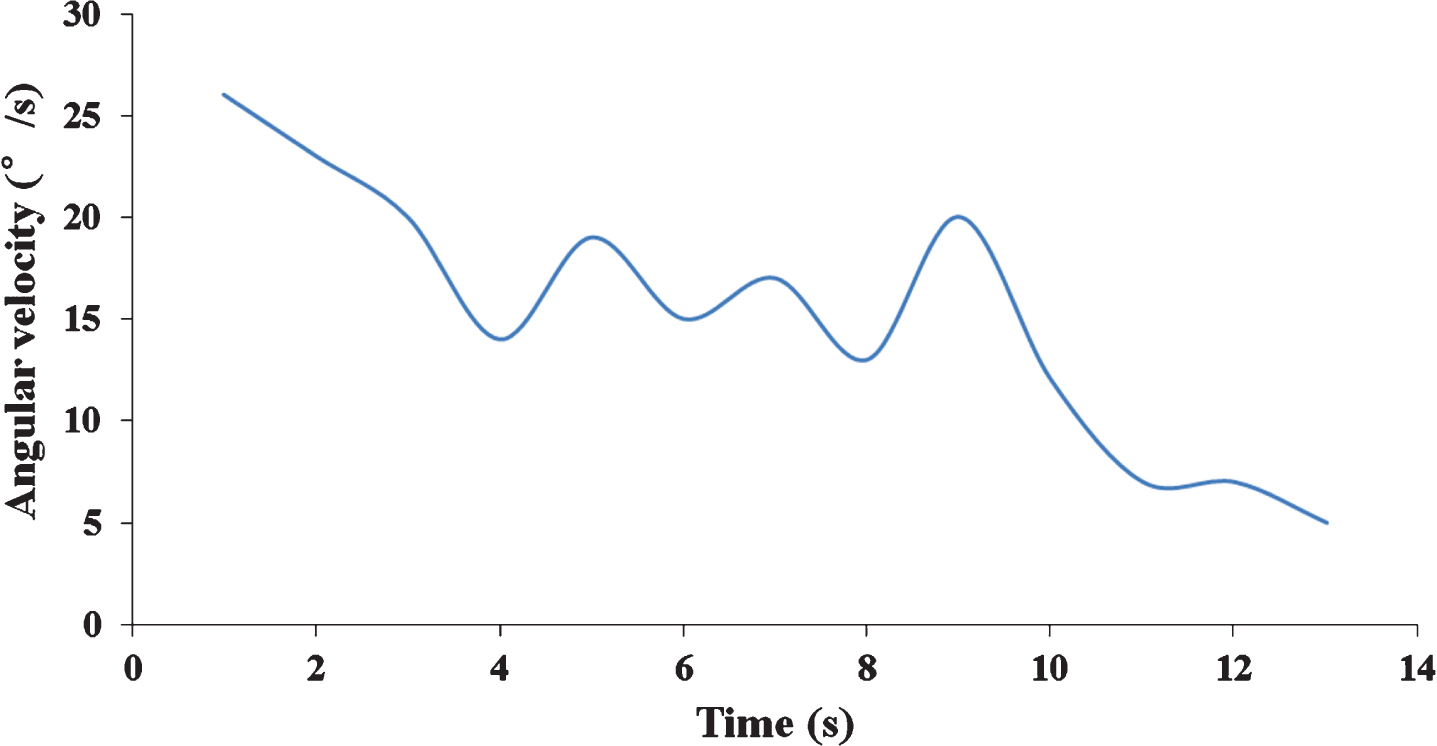
Slow angular velocity curves of the nystagmus in a BPPV patient when changing from the supine to sitting position.
The model constructed in the present study was based on previously reported data [8], and the facticity of the model was found to be reliable. Moreover, the numerical results of cupula displacement caused by the movement of 30-μm particles in the semicircular duct were similar to previous experimental results [14], which indicated that the calculations of the model were also reliable. The real radius of the canaliths is approximately 0.5–15μm, with an average of 7μm [3]. As shown in the Fig. 5, the settling duration of particles with a diameter of 10μm is much longer than that of particles with a diameter of 30μm, and the whole movement process lasts for more than 40 s, which is consistent with the real situation. The calculation results for the different numbers of otoliths with the same mass are also consistent with Rajguru’s. The model calculations showed the movement of different numbers and sizes of canaliths in the semicircular duct. The force produced by the moving canaliths on the endolymph was transmitted to the cupula, resulting in ΔP on both sides of the cupula, whereas ΔP was related to the canalith diameter and speed. Owing to the different initial canalith falling positions, some near the inner side may touch the inner wall first, as described by Hain [6], resulting in changes in canalith movement. When they fell onto the inner wall, they slid down along the inner wall and their falling speed decreases. After passing along the inner wall, their speed in the endolymph increased again until they fell onto the outer wall. The movement pattern of the cupula caused by canalith falling was consistent with the nystagmus pattern obtained through clinical testing, in that the slow angular velocity increased initially and then decreased. When BPPV patients change their head position and the canaliths start to move in the ampulla, cupula displacement is minor and the slow angular velocity of the nystagmus is low. Patients do not experience vertigo during this period of time, which we propose corresponds to the latent period. With increased canalith speed, the cupula deviation reaches a certain degree, which leads to the deflection of sensory cilia and the transmission of an electrical signal. The patient then experiences vertigo and an intense nystagmus is observed, which we propose is the onset stage. Cupula displacement varied with time, which was in accordance with the results of Djukic [4].
When the number of canalith particles was greater, the ΔP and cupula displacement patterns caused by canalith movement were similar to the above results. As the number of canaliths increased, the force on the endolymph increased and the ΔP and cupula displacement increased. However, from the displacement curve, although the latent period and the duration of BPPV changed, the degree of these changes was not significant. Under the condition of the same total mass (1μg), the canalith particles with a large diameter will fall into the bottom of the membranous labyrinth at a rapid pace. Because the whole movement time is short, the force acting on the cupula cannot reach the maximum displacement; therefore, the displacement of the cupula is limited. When the canalith particle diameter became larger, the duration of movement in the endolymph was shorter. From the displacement curve, the latent period and the duration of BPPV were also shorter. However, owing to the large canalith diameter, the contact area with the endolymph increased and cupula displacement caused by canalith movement significantly increased. Therefore, it can be inferred that when the canalith reaches a certain size, patients may have almost no latent period, and they will experience vertigo immediately after the head position changes, which has also been observed in clinical cases.
We observed that the diameter of the circular duct was larger, the diameter of the non-ampulla part of the actual semicircular duct was smaller, and cupula displacement caused by canalith movement in the circular duct was smaller in the simulation results of the circular duct model than in the actual semicircular duct. This indicates that cupula displacement is also affected by the diameter of the semicircular duct, with a smaller diameter resulting in greater cupula displacement. In other words, the pathogenesis of BPPV is directly related to the geometric structure of the semicircular ducts.
From the numeircal results, it can be inferred that the influence of canalith shape on cupula displacement is small, but its influence on falling duration is clear. This may be due to the fact that the small shape coefficient will increases the Stokes drag force and then reduces the falling speed of canaliths. Hence, the peak time of cupula displacement and falling duration increased.
According to the simulation results of body position change, when a patient moves from a sitting to supine position, the canaliths start to fall from the expanded ampulla; therefore, the cupula displacement was initially minor. This represents the latent period during which the patient does not experience vertigo. It was not until the canaliths fell to the thin duct that cupula displacement began to significantly increase, and the patients began to experience vertigo. When the patient moved from a supine to sitting position, the canaliths gathered in the thin duct began to move, and the patient experienced vertigo. This is because the movement of canaliths in the thin duct is more likely to cause cupula displacement, which is consistent with the results of a previous study on the influence of duct diameter. According to the test results of clinical cases, when a patient moved from a sitting to supine position, there was a latent period, and the vertigo duration was long (approximately 27 s). When the patient moved from a supine to sitting position, with almost no latent period, vertigo immediately occurred and lasted approximately 10 s. These test results were consistent with the results of the numerical simulation.
This study established the relationship between movement of canaliths in the endolymph with cupula displacement. The relationship between cupula displacement and nystagmus has previously been shown [16, 23]. This may help clinicians rough estimate the component of canaliths through nystagmus and further understand the patient’s condition. In the present study, the effect of velocity storage [20] was not considered, and only the influence of mechanical factors was considered.
Currently, the standard treatment for BPPV involves resetting the canaliths by rotating the head in a certain manner to cause the fallen canaliths to return to the utricle. When patients rotate their heads, the canaliths no longer affect the movement of the endolymph. However, under certain conditions, the canaliths may reenter the semicircular duct from the utricle, leading to disease recurrence. BPPV is a self-limiting and self-healing disease. The current explanation for this is that the vestibular dark cells and endolymph absorb the canaliths [11, 25]. The significance of this study is that it combined the movement of canaliths in the endolymph with nystagmus. The size of canaliths can be roughly inferred from the nystagmus. Assuming that all canaliths have the same diameter, canalith size can be inferred from the latent period and vertigo duration. Smaller canaliths result in a longer latent period and vertigo duration, and vice versa. If the canaliths are composed of particles with different diameters, the larger particles will fall first and the nystagmus will show a short latent period and a long duration. This is an ideal situation. However, the real situation may be more complicated [18]. In the present study, the effect of velocity storage [20] was not considered, and only the influence of mechanical factors was considered. However, the actual law should be similar to the results of this study. A relationship between cupula displacement and nystagmus has previously been shown [16, 19]. We can infer the size and number of canaliths through nystagmus. This would help clinicians predict the time required for the complete digestion of canaliths in the endolymph and determine the self-healing time.
Conclusions
From the above numerical analysis and the results of the nystagmus experiment, we can see that the composition of canalith particles affected the movement of the cupula, which was reflected in the nys-tagmus. The particle velocity was proportional to its diameter, and the pressure difference between the two sides of the cupula was directly proportional to the diameter and the number of canaliths. The latent period of BPPV was related to the particle diameter, with larger particles resulting in shorter latent periods. The duration of vertigo was also related to the particle diameter with larger particles, resulting in shorter vertigo duration. The latent period was also related to body position. When moving from a sitting to supine position, the particles moved from the expanded ampulla, and the latent period was relatively long. When moving from a supine to sitting position, the particles moved in the duct, and the latent period was relatively short.
Footnotes
Acknowledgments
This study was funded by the National Nature Science Foundation of China (11572079, 11772087, 31500765).
The authors have no conflicts of interest to disclose.