
Abstract
BACKGROUND:
The etiology and mechanism of persistent geotropic horizontal direction-changing positional nystagmus (DCPN) are still unclear. Whether this pattern of nystagmus is a subtype of benign paroxysmal positional vertigo (BPPV) remains controversial.
OBJECTIVE:
The goal of this study was to observe the clinical characteristics of persistent geotropic horizontal DCPN involving the lateral semicircular canal.
METHODS:
The analysis was performed to participants with episodic positional vertigo in our clinic from 2014 to 2021. Participants were included via positional test. We observed and summarized the distribution data, vertigo history, follow-up tests, and recurrence situations of 189 persistent geotropic horizontal DCPN participants.
RESULTS:
The mean age at the first time showing of persistent geotropic horizontal DCPN was 56±14.7 and more women than men were affected by persistent geotropic horizontal DCPN (female-to-male ratio 2.4 : 1). Overall, 58.7% (57/94) of participants who came for the first-week follow-up test were asymptomatic. Thirty-three participants experienced recurrence (female-to-male ratio: 4.5 : 1). Fifty-three (28.0%) participants experienced the conversion of the patterns of DCPN in the history, the follow-up tests and the recurrence compared to the first showing of persistent geotropic horizontal DCPN. 24(12.1%) participants still experienced persistent geotropic horizontal DCPN attack in the follow-up tests and the recurrences without benign paroxysmal positional vertigo history.
CONCLUSION:
Persistent geotropic horizontal DCPN affected more women than men. The persistent geotropic horizontal DCPN that with conversion to transient geotropic horizontal DCPN or to persistent apogeotropic horizontal DCPN might be a subtype of BPPV or in a stage of BPPV process. However, the persistent geotropic horizontal DCPN without conversion might be an independent disease that is not related to BPPV.
Keywords
Introduction
Benign paroxysmal positional vertigo (BPPV) that characterized as episodic vertigo and nystagmus is caused by fragments of degenerating otoconia that move freely in the semicircular canal (canalolithiasis) or are attached to the cupula (cupulolithiasis) and thereby displace the cupula, producing asymmetric vestibular stimulation that leads to vertigo and nystagmus [7]. Lateral semicircular canal BPPV (LSC-BPPV) is the most common type of BPPV second to posterior semicircular canal BPPV (PSC-BPPV).
The subtypes of LSC-BPPV depend on the direction-changing positional nystagmus (DCPN) in the supine roll test (SRT) [24]. The geotropic variant due to canalolithiasis of the posterior part of the LSC shows a transient (< 1 min)geotropic horizontal DCPN, the apogeotropic variant due to canalithiasis of the anterior part of the LSC near the cupula shows a transient apogeotropic horizontal DCPN, and the apogeotropic variant due to cupulolithiasis or heavy cupula shows persistent (> 2 min) apogeotropic horizontal DCPN. However, persistent geotropic horizontal DCPN is thought to be caused by the lower specific gravity of the LSC cupula than its surrounding endolymph, namely, the light cupula. Previous studies [9, 27] have illustrated the clinical characteristics of the persistent geotropic horizontal DCPN: intractable barbecue roll maneuver, spontaneous resolution tendency (in one week), and ease of recurrence.
The etiology and mechanism of the persistent geotropic horizontal DCPN are still unclear. Several hypotheses have been proposed. The light debris cupulolithiasis hypothesis [4, 9] states that light particles attach to the lateral semicircular cupula and cause the cupula to move upward. However, the identification of light particles has not been reported thus far. The light cupula hypothesis is derived from the positional alcohol nystagmus (PAN) described by Aschan [1]. The heavy endolymph hypothesis assumes that the density or viscosity of endolymph rises due to peripheral hypofusion, labyrinth bleeding, inflammation, or hormone imbalance [5, 15]. Kim [13] proposed the density hypothesis, wherein the density discrepancy between the peri- and endolymph might account for the light cupula. However, none of these hypotheses can perfectly explain this phenomenon. Whether the persistent geotropic horizontal DCPN is a subtype of BPPV remains controversial.
The purpose of this study is to observe and summarize the distribution and clinical characteristics of participants with the persistent geotropic horizontal DCPN to further understand this phenomenon.
Methods
Participants
This study included participants with persistent geotropic horizontal DCPN (n = 189, female:134, male:55, mean ages:56 years) who were diagnosed at our institution between May 2014 and May 2021 with chief complaints of episodic positional vertigo. We investigated the demographic data, vertigo history, follow-up tests. Meanwhile, we observed the subtypes of a recurrent vertigo attack for at least 1 year. Participants were asked to revisit the clinic, if they experienced a recurrence of vertigo. The study was approved by the Institutional Review Board of our hospital.
Positional test
An experienced technician performed the positional test (must be minimum of SRT) on participants with eyes open using an infrared video-nystagmography goggle. We recorded nystagmus and vertigo symptoms.
Supine roll test SRT: the participant was in the supine position with the head inclined forward at an angle of 30°. The head was turned to the right and kept in the right-ear-down position for 2 min to determine whether the nystagmus was transient or persistent, and then head was turned towards the left and kept in the left-ear-down position for 2 min to determine whether nystagmus was transient or persistent.
The bow and lean test [6]: the participant sat on the edge of a treatment table with the head bow forward over 90° and kept in the bowing position to observe the direction of nystagmus. Then the participants leaned the head backward over 45° and kept in the leaning position to observe the direction of nystagmus.
The seated supine test [26]: the participant was in seated position to investigate the spontaneous nystagmus. Then the participant was briskly brought from the seated position to the supine position with the head inclined forward at the angle of 30° to observe the direction of nystagmus.
Dix-Hallpike test: the participant was in seated position with head turn right/left at an angle of 45°.Then the participant was quickly brought down to the supine position with the neck extended 30° below horizontal to observe the direction of nystagmus.
Four patterns of DCPN were recorded. The persistent geotropic horizontal DCPN (PGHDCPN), the persistent apogeotropic horizontal DCPN(PAHDCPN), and the transient geotropic horizontal DCPN (TGHDCPN) in SRT, the bow and lean test and the seated supine test. The transient torsional vertical DCPN(TTVDCPN) in Dix-hallpike test.
Exclusion criteria
Cochlear symptoms related to vertigo. Central nervous system disorder and abnormal results on cerebral image. History of head trauma.
Inclusion criteria
The persistent geotropic horizontal DCPN demonstrated the following positional nystagmus: With or without weakly pseudospontaneous nystagmus beating toward the unaffected side in an upright seated position [2]; Persistent geotropic horizontal DCPN > 2 minutes in SRT; Seated supine test: persistent nystagmus beating toward the healthy side in the supine position; Bow and lean test: leaning nystagmus beating toward the healthy side in a head-up position, and bowing nystagmus beating toward the affected side in a nose-down position; The nystagmus stops when the head is slightly turned (15–40°) to the affected side in the supine or prone position. This point has been referred to as the neutral point, zero zone, neutral position, null plane, and null point [8, 14]. The side of this point is considered the affected side.
Definition of recurrence
We defined recurrence as a vertigo attack (regardless of subtype and affected side) occurring more than two weeks after the complete remission of previous vertigo. Complete remission means that the symptoms and positional nystagmus disappeared completely. We counted the recurrence time from 2 weeks after the complete remission of the last vertigo [11].
Follow-up tests
No special treatment was provided to these participants. We asked the participants to revisit the clinic in the first, second, and third weeks after their first-time show of the persistent geotropic horizontal DCPN. We also asked the participants to revisit the clinic whenever they experienced a recurrence of positional vertigo. We investigated the time of recurrence and determined the subtypes of a recurrent positional vertigo attack for at least 1 year. The participants completed all the positional test stated above.
Definition of converted DCPN
We defined converted DCPN as the conversion of patterns of DCPN in the history, in the follow-up tests and in the recurrence compared to the first showing of PGHDCPN. We counted the converted DCPN involving different semicircular canals and the different affected sides.
Manifestations in follow-up tests.
3.1 Distribution and clinical data (Table 1)
Table 1 shows the distribution and clinical data of the 189 PGHDCPN participants. More women than men were affected. More than half of the participants (51.3%) were older than 60. The affected side showed no difference between the left and right sides.
distribution in persistent geotropic horizontal DCPN participants
distribution in persistent geotropic horizontal DCPN participants
One hundred and twenty (63.5%) PGHDCPN participants had an episodic positional vertigo history, among which 11 showed TGHDCPN (lateral canalolithiasis), 5 showed PAHDCPN (lateral cupulolithiasis or heave cupula), 12 showed TTVDCPN (posterior or anterior canalolithiasis), 5 showed combined TGHDCPN+TTVDCPN, and 87 had positional vertigo but with non-observable nystagmus in positional test.
vertigo history of persistent geotropic horizontal DCPN participants
vertigo history of persistent geotropic horizontal DCPN participants
TGHDCPN = Transient Geotropic Horizontal DCPN. PAHDCPN = Persistent Apogeotropic Horizontal DCPN. TTVDCPN = Transient Torsional Vertical DCPN.
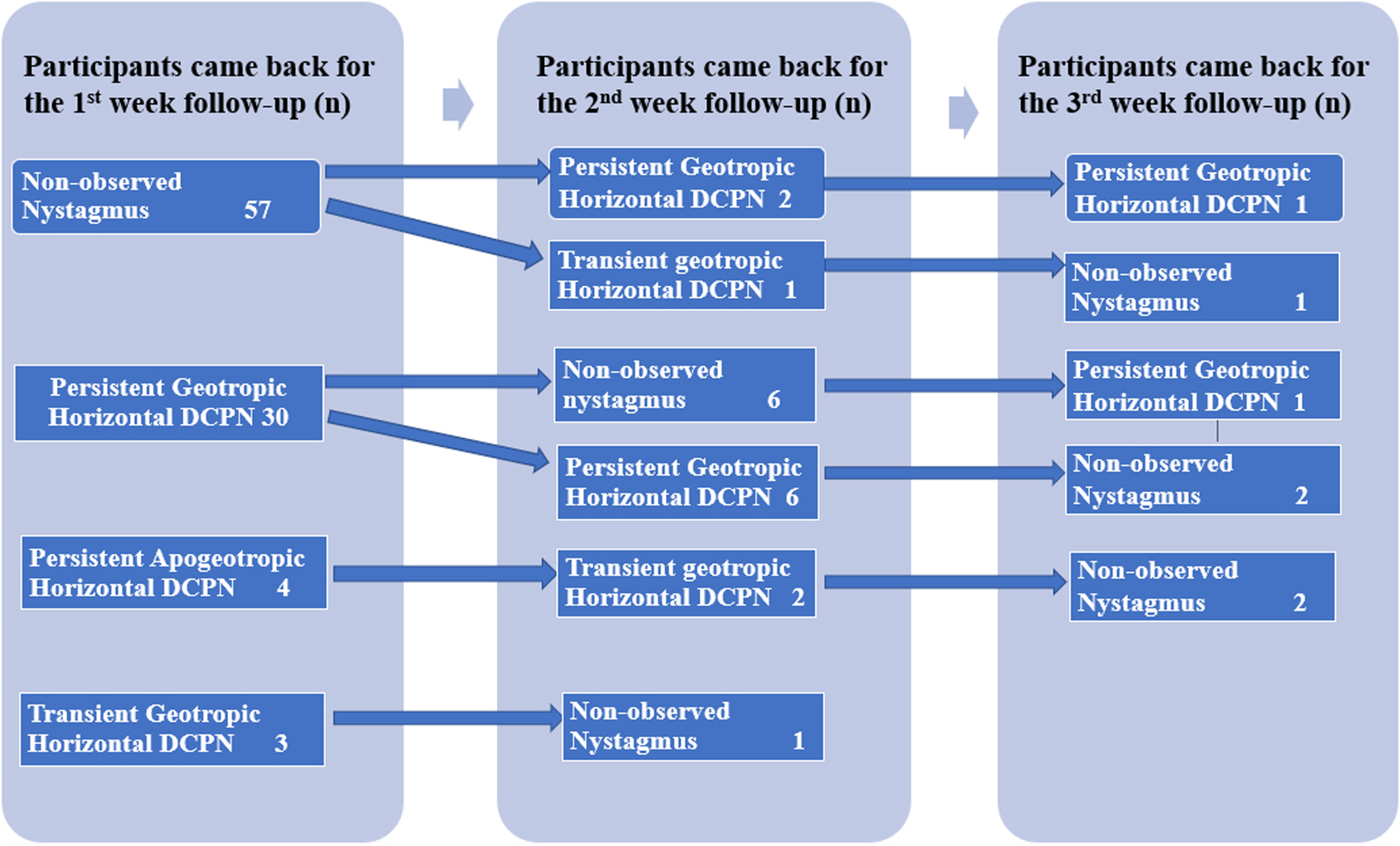
Ninety-four participants returned for the first-week follow-up test. Among which 57 were asymptomatic and absent nystagmus on positional tests. Thirty participants showed persistent geotropic horizontal DCPN, with 29 showing the same affected side and one change to the contralateral side. Four participants showed PAHDCPN. Three participants showed TGHDCPN.
Eighteen participants returned for the second-week follow-up test, and among which 7 were asymptomatic and showed non-observable nystagmus on positional tests. At the same time, 3 participants who were asymptomatic at the first-week follow-up again showed positional vertigo and nystagmus, compatible with PGHDCPN in two participants and with TGHDCPN in another participant.
Seven participants returned for the third-week follow-up test, and only 2 female participants still showed PGHDCPN with the same lesion side.
Recurrence (Table 3)
Thirty-three participants (17.4%) experienced the first recurrence with a recurrence time from 0.5 months to 60 months. More women than men experienced recurrence (female:male = 4.5 : 1). Thirteen experienced PGHDCPN recurrence with an average recurrence time of 8.1 months, one experience PAHDCPN recurrence with recurrence time of 14 months, three experienced TGHDCPN with average recurrence time of 23 months, ten experienced TTVDCPN with average recurrence time of 19.6 months, and six experienced positional vertigo with non-observable nystagmus in the positional test, with an average recurrence time of 20.6 months.
Patterns of DCPN in thirty-three participants who experience recurrences
Patterns of DCPN in thirty-three participants who experience recurrences
NO. = the serial number of the cases in this study. F = female; M = male; R = right; L = left. PGHDCPN = Persistence Geotropic Horizontal DCPN; TGHDCPN = Transient Geotropic Horizontal DCPN; PAHDCPN = Persistent Apogeotropic Horizontal DCPN; TTVDCPN = Transient Torsional Vertical DCPN;Other vertigo = positional vertigo withnon-observable nystagmus.
Six participants experienced a second recurrence. Of these six participants, two experienced PGHDCPN (who showed TTVDCPN in the first recurrence), two experienced TGHDCPN, one experienced PAHDCPN+TTVDCPN and one experienced TTVDCPN The patterns of DCPN are shown in Table 3.
Fifty-three participants experienced the conversion of the patterns of DCPN in the history, in the follow-up tests and in the recurrence compared to the first showing of PGHDCPN. Although the conversions were multiple, we concluded four conversion types: (1) 24 participants experienced conversion between TGHDCPN and PGHDCPN (11 showed TGHDCPN converted to PGHDCPN, 5 showed TGHDCPN+TTVDCPN converted to PGHDCPN, and 8 showed PGHDCPN converted to TGHDCPN). (2) 10 participants experienced conversion between PGHDCPN and PAHDCPN (5 showed PAHDCPN converted to PGHDCPN, 4 showed PGHDCPN converted to PAHDCPN, and 1 showed PGHDCPN converted to PAHDCPN+TTVDCPN), (3) 25 participants experienced conversion between PGHDCPN and TTVDCPN (9 showed TTVDCPN to PGHDCPN, 5 showed TGHDCPN+TTVDCPN converted to PGHDCPN, 8 showed PGHDCPN converted TTVDCPN, and 3 showed TTVDCPN converted to PGHDCPN and to TTVDCPN again) (4) 1 participants experienced the conversion among PGHDCPN, TGHDCPN and PAHDCPN. The patterns of DCPN conversion are shown in Table 4.
Participants that experience conversion of patterns of DCPN
Participants that experience conversion of patterns of DCPN
No. = the serial number of the cases in this study. F = female; M = male; R = right; L = left. PGHDCPN = Persistence Geotropic Horizontal DCPN; TGHDCPN = Transient Geotropic Horizontal DCPN; PAHDCPN = Persistent Apogeotropic Horizontal DCPN; TTVDCPN = Transient Torsional Vertical DCPN;Other vertigo = positional vertigo with non-observable nystagmus.
In this study, the distribution data of the PGHDCPN were similar to those of BPPV reported previously. The mean age of the onset of PGHDCPN participants was 56 years, which was slightly older than previous studies reporting a mean age of 49.3 to 52.8 [22, 25] for BPPV. More than half of the PGHDCPN participants (52.3%) were older than 60, consistent with the age characteristics of BPPV. It was previously reported that BPPV had a peak age of onset in the sixth decade for idiopathic BPPV [3]. More women than men are affected by PGHDCPN (female-to-male ratio 2.4 : 1). The ratio is slightly higher than BPPV, reported as 1.5–2.2 : 1 [16]. The basis of the female preponderance in BPPV is not known but may be related to osteoporosis, migraine, or both [23]. The higher female ratio in PGHDCPN than BPPV indicated that osteoporosis might play a more important role in the PGHDCPN. Ichijo et al. [12] reported that BPPV predominantly affects the right labyrinth in both sexes. This preponderance is due to the laterality of the sleeping position. However, our study found that the side preponderance of the PGHDCPN was not as prominent as BPPV, which might be attributed to the fact that sleeping position is not always the same each night, and ordinary people turn over in bed many times per night.
Of the participants who came for the first-week follow-up test,60.6% were asymptomatic and showed non-observable nystagmus in positional test. Previous studies reported that the remission rates of PGHDCPN (light cupula) in the first-week follow-up were 42.9% [3] and 70.4% [22]. The etiology of spontaneous remission of PGHDCPN is due to the dissolve of the light debris or the compensation of the specific gravity of the endolymph. However, the remission rates at 1 week are variable maybe due to the different time of the symptoms prior to being treated.
Data on the recurrence rate of PGHDCPN are scarce. Seo [19] reported 33% based on 27 light cupula (PGHDCPN) cases, and Ichijo [11] reported 72.3% based on 34 light cupula cases. However, in our study, the recurrence rate of PGHDCPN was only 17.1%, which war much lower. Although we asked participants to revisit if they experienced a recurrence of vertigo, not all of them came. The reasons are multiple: some participants will not come back for the vertigo when they knew that the disease was not a big problem, or they might go to other hospital. Meanwhile, the observation time was not long enough. Therefore, we might have underestimated the recurrence rate. Previous studies reported that all types of BPPV and LSC-BPPV recurrence were 7% –56% [18] and 20% –38.5% [19], respectively. When compared to BPPV, we found that the recurrence of the PGHDCPN was lower but much closer to that of LSC-BPPV. Previous studies reported that sex did not impact BPPV recurrence [14, 22]. However, we found that more women than men experienced recurrence, and the sex ratio of PGHDCPN recurrence was nearly two times higher than the sex ratio of prevalence (4.5 : 1 vs. 2.4 : 1). Except for the osteoporosis and the migraine states above, the reason for the female preponderance in recurrence may also due to the higher rate of revisit for the women.
The patterns of DCPN in the history, in follow-up tests and in the recurrence were not always the same as the first showing PGHDCPN. Conversion of the patterns of DCPN had been reported previously. Ichijo [11] reported that 9/33 light cupula changed to cupulolithiasis or heavy cupula in recurrence. Shin [21] reported the conversion between persistent geotropic and apogeotropic DCPN in patients with sudden hearing loss and cupulopathy. He concluded that these two groups’ clinical characteristics during conversion were different. In our study, conversion of patterns of DCPN were observed in 28.0% of PGHDCPN participants. The mechanism of the conversion phenomenon is unclear. We speculated the followings to be the potential causes behind this phenomenon. 1.The otolith particles that attached to the cupula or in the LSCC subsequently change into light debris because of degeneration or decalcification. This might explain the conversion of TGHDCPN to PGHDCPN. 2 the light debris in the LSCC experienced increase of density due to concentration or gathering. This might explain the conversion of PGHDCPN to TGHDCPN or the conversion of PGHDCPN to PAHDCPN. So, we assumed that these two types of PGHDCPN with converted tendency might be a subtype of BPPV or in a stage of BPPV process. 3 a change in the specific gravity of the endolymph due to over-compensation. This might explain the conversion between PGHDCPN and PAHDCPN. As for the conversion between PGHDCPN and TTVDCPN (posterior/ anterior canalolithiasis) might not be the same diseases because the affected canals are different. We should observe for longer time to figure out this phenomenon. Furthermore, 24(12.1%) PGHDCPN participants still experienced PGHDCPN attack in the follow-up tests and the recurrences without BPPV history. We speculate this non-converted type of PGHDCPN might be an independent disease that is not related to BPPV. However, longer periods should be observed to ensure that the PGHDCPN patterns will not change. Meanwhile, we speculated that if the time interval between the DCPNs is relatively long and each DCPN occurs abruptly rather than gradually, the conversion phenomenon might also be explained by simple independent attack even if the affected side and semicircular canal is same.
The affected sides differed in the converted PGHDCPN participants. Of the 53 converted PGHDCPN participants, 28.3% (15/53) differed in the affected sides, In a strict sense, the different affected sides relapse may not be the same disease. However, it happens sometimes. The phenomenon was also seen in BPPV. Perez et al. [18] reported that 37% of BPPV recurrences affected the contralateral ear. Shigeno [20] showed that 17% of BPPV recurrences were on the opposite side. These phenomena indicate that these converted PGHDCPN participants have some constitution that produces pathological debris similar to the BPPV participants.
Limitations
Some limitations of our work should be underlined. First, this study was started from 2014. Due to the limited previous understanding of light cupula, we did not collect complete clinical information, such as detailed vertigo histories; take other vestibular function tests; or observe the episode duration or relationship of PGHDCPN to migraine, sudden sensorineural hearing loss (SSHL) and central vertigo. Second, many participants were lost to follow up. As a result, the recurrence rate was probably heavily underestimated.
Conclusion
PGHDCPN affected more women than men. PGHDCPN that manifested conversion to TGHDCPN or to PAHDCPN might be a subtype of BPPV or in a stage of BPPV process. However, the PGHDCPN without conversion might be an independent disease that is not related to BPPV.
Footnotes
Acknowledgments
This work was supported by the National Key Research and Development Program of China (No. 2020YFC2005202).