
Abstract
BACKGROUND:
Serum otolin-1 is an inner ear protein exclusively expressed in otoconia and cells of vestibule and cochlea. Serum otolin-1 is found to be quantifiable in patients with BPPV. Low Vitamin-D is associated with pathogenesis of BPPV. Since otoconia degeneration contributes to BPPV, lack of Vitamin-D may impact otoconia structure and integrity.
OBJECTIVE:
We aimed at studying the s.otolin-1 as biomarker and significance of vit-D in BPPV.
MATERIAL AND METHOD:
23 patients in test and control groups respectively were chosen within the age of 20 to 65 years. All the patients were diagnosed using Dix Hallpike menouver and head roll test, patients were treated with appropriate Canal Reposition Menouver (CRM).
RESULTS:
Serum Otolin-1 levels among the test ranged from 366 to 882 pg/mL with mean of 585.17 pg/mL whereas in control group ranged from 223 to 462 pg/mL with mean of 335.26 pg/mL. Mean Vitamin-D levels among the test group was 22.67 ng/mL (Range = 6.3–68.4) and that of control 15.43 pg/mL (Range = 5.4–27.7) respectively. The relationship between the serum Otolin-1 and Vitamin-D was not statistically significant.
CONCLUSION:
Otolin-1 levels is increased in BPPV patients and is sensitive in BPPV, specificity needs to be validated. Role of vitamin-D with respect to inner ear proteins needs further investigation.
Introduction
Benign paroxysmal positional vertigo (BPPV) is an irritating disease of peripheral labyrinth characterized by sudden spinning sensation lasting less than a minute that occurs typically with head position changes. Worldwide, it has a lifetime prevalence of 2.4% and a one-year prevalence of 1.6% [4, 31]. It has been well established already that BPPV is caused due to dislodgement of otolith from the otoconial membrane into the semi-circular canals [15]. The otoconial membrane covers the macula of vestibule of inner ear and is made up of numerous inner ear proteins, among which the chief constituents are otolin-1 and otoconin-90 [7, 15]. Otolin-1 is assumed to participate with the other glycoprotein molecules to form a cross-linkage in order to stabilize and strengthen the otoconia [7, 32]. Thus, it has been hypothesized that since otoconial degeneration is the hallmark in BPPV, there should be an increase in the otolin-1 levels in the inner ear microenvironment and subsequently in the peripheral circulation following an attack of BPPV [21].
BPPV is mostly diagnosed with a Dix-Hallpike test or a supine head roll test. The sensitivity and specificity of the Dix-Hallpike test are 79% and 75% respectively (Halker et al 2008) [12]. Jacquelien Droset. al reported a sensitivity of Dix Hallpike as 80% [9]. This means that with an as good test as Dix Hallpike, BPPV may be missed clinically in those patients who are negative for the test. A complete foolproof diagnosis may not be able to be made in every case of BPPV, making them visit the health care centers multiple times. Hence a reliable biomarker can ease this procedure and accurately diagnose the disease. Efficacy of Epley’s range from 75–80% in conversion of DHP positive to negative. Sometimes, a patient may be labeled as an atypical BPPV and may require more than one reposition maneuver for treatment [6, 25]. A biomarker for otoconial degeneration can help as a potential diagnostic modality, therapeutic targeting as well as prognostication and therapeutic response monitoring for this otherwise unfathomed structure from a clinical perspective.
There has been adequate evidence in the literature stating the role of insufficient levels of vitamin-D in BPPV and its recurrence [1, 27]. The majority (about 90%) of the Indian population fall under the “insufficiency and deficiency level” range [2, 18]. Also, the low bone mineral density in osteoporosis and elderly have a strong association with the BPPV [27]. Reduced vitamin D levels results in disruption of calcium, resorption of calcium carbonate in the otoconia, and increased osteoclast differentiation and calcium phosphate resorption, respectively [5]. Resorption of calcium (demineralization) results in the fragmentation of otoconia and increased vulnerability to BPPV. However limited evidence says that vitamin-D is not related to the pathogenesis of BPPV and its recurrence [16, 17]. In osteoporosis, some studies conclude that there was no significant difference between the test and controls hence suggesting that low vitamin-d may be a coincidental finding rather than a risk factor [16].
Owing to the controversial role of vitamin-D in BPPV, we aim to study its role in the disease of interest in an indirect way that if there is a substantial destabilization of otoconia in BPPV patients leading to release of inner ear markers in the peripheral circulation. Could this process be determined by the vitamin-D levels or not. Hence we tried to see whether vitamin-D levels are affecting the stability of the otoconia in the inner ear, by correlating it with the disease and inner ear marker levels.
Methods
This prospective cross-sectional case-control study was performed in the Department of Otorhinolaryngology and Head & Neck Surgery in collaboration with the Department of Cardiac Biochemistry & the Department of Biochemistry. The study was carried out after approval from the Institutional Ethical Committee (IECPG-413/30.08.2018, RT-9/27.09.2018). The study groups were divided into Test and Control groups with 23 subjects in each group respectively. The number of subjects in each group was decided based on existing literature [21]. The inclusion criteria for test subjects were: Age group between 20–65 years Recurrent attacks of positional vertigo lasting < 1 min Dizziness not attributable to any other disease
A control was defined as an age matched (+/–2 years) with no symptoms of dizziness. Exclusion criteria for both groups were: Subjects not within prescribed age limit. Subjects with comorbid conditions hypothyroidism/diabetes/hypertension, chronic liver/kidney diseases Subjects who have had previous ear surgeries/vestibular sedative drug intake/neurological conditions to remove the confounding factors.
Both groups were examined and blood samples were collected after obtaining informed written consent. The diagnosis was made by the peculiar sym-ptoms of BPPV in history & positive Dix-Hallpike, supine head roll test. Additional otoscopic evaluation, tuning fork and audiometric evaluation and complete neurological evaluation were done to rule out other causes of dizziness. VNG test was done wherever required. Venous Blood samples were obtained from the subjects for analysis.
Human otolin-1 was assessed in serum samples by Enzyme-Linked Immunosorbent Assay (Cat No: MBS772738; MyBiosource, San Diego, California, United States) which employs the principle of biotin double antibody sandwich technology as per the instruction manual. A series of a standard solution containing a precisely known concentration of otolin-1 was used to prepare a standard graph. Standards and samples were loaded on antibody-coated plates, the conjugate reagent was added to the wells, covered and gently shaken and was kept incubated at 37°C for 60 minutes. After the incubation, the plates were washed multiple times. The absorbance (Optical Density OD) of the plate was measured at 450 nm wavelength. According to the OD value of samples, the concentration of the corresponding sample was calculated using the linear regression equation of the standard curve.
For vitamin D evaluation, The samples were stored at –80 degrees until the time of analysis. The levels of 25-hydroxy vitamin-D levels were assessed by chemiluminescence method (Liaison, Diasorin). The LIAISON® 25-hydroxyvitamin D Assay (DiaSorin) uses chemiluminescent immunoassay technology. Specific antibody to vitamin D was used for coating magnetic particles (solid phase) and vitamin D was linked to an isoluminol derivative. During the incubation, 25-hydroxyvitamin D was dissociated from its binding protein and competes with labelled vitamin D for binding sites on the antibody. After the incubation, the unbound material was removed with a wash cycle. Subsequently, the starter reagents were added and a flash chemiluminescent reaction is initiated. The light signal was measured by a photomultiplier as relative light units and was inversely proportional to the concentration of 25-hydroxyvitamin D present in samples. Two levels of quality controls were run with every batch
Statistical analysis
STATA 15.0 statistical software was used for data analysis. Data was recorded on a pre-designed proforma and managed on an excel spreadsheet. All the entries were checked for any possible keyboard error. All quantitative variables were assessed for approximate normality and summarized as Mean±SD or median (Q1, Q3). Independent sample t-test was used to compare serum otolin levels in the two genders separately for intervention and control groups. Spearman correlation was used to correlate Serum otolin levels with vitamin D levels. p-value < 0.05 was considered as statistically significant.
Results
A total of 46 subjects were recruited for the study (23 test and 23 control) who met the selection criteria. The age group among the Test subjects ranged from the 24 years to 65 years, with mean age of 46.3 years with 74 % females and 26% males. The control group subjects’ ages range from 22 years to 65 years with a mean age of 41.82 years with 78% females and 22% males respectively. The female to male ratio in the Test and Control group were 2.8:1 and 3.6:1 respectively. There were more post menopausal women than pre or perimenopausal ones in both Test and Control groups. Table 1 represents various parameters of the study.
Showing various parameters of Test subjects of the study
Showing various parameters of Test subjects of the study
The mean duration from the recent attack of BPPV to the time of sample collection was 2.45 days. Among the test subjects, the predominant etiology of BPPV was idiopathic in about 87% followed by post-traumatic which was 13 %. The mean serum Otolin-1 of those diagnosed post-traumatic BPPV was 609 pg/mL and that of idiopathic BPPV was 597.38 pg/mL.
The 83% were diagnosed as posterior canal BPPV and 17% were diagnosed as horizontal canal BPPV. The mean serum Otolin-1 in the P’SCC BPPV was 599.3 pg/mL and in H’SCC BPPV was 516.25 pg/mL respectively.
After the patients were treated with appropriate canal reposition procedures, about 3 patients exhibited canal shift and re-entry phenomenon. Of the 3 patients, 2 were diagnosed as posterior canal BPPV who were previously treated for horizontal canal BPPV. 1 patient had a canal shift from posterior to horizontal on a subsequent visit.
The mean serum otolin-1 among the BPPV was found to be 585.179 pg/ml as compared to control subjects with mean levels of 335.260 pg/ml (Table 3). The serum Otolin-1 level was ranged from 366–882 pg/ml in the test group whereas the range was 223–462 pg/mL in the control group. More than two-thirds(> 66%) of test group subjects were having serum otolin levels higher than those of age matched control subjects. Comparison of serum Otolin-1 levels between test and control subjects was found to be statistically significant with a (p = 0.0000).
The serum level of vitamin-D among test subjects ranged from 6.3 to 68.4 ng/mL with a mean of 22.67 ng/mL, while it ranged from 5.4 to 27.7 ng/mL with a mean of 15.43 ng/mL in control group (Table 3).
As per the patients’ history, there were 14 patients with a history of 2 or more attacks in the past. The number of attacks of BPPV ranged from 2 to 8 with a median of 5 attacks. Out of 23 patients who underwent CRP, 12(52.1%) had a recurrence, which was defined as subjects presenting with symptoms of BPPV in same canal after atleast 2 weeks of initial CRP. These subjects required one or more CRPs in subsequent visits. Table 2 shows serum Otolin-1 levels among the Test subjects.
Showing various Otolin-1 levels among the subjects
A statistically significant results were not obtained when the mean serum otolin-1 and mean Vitamin-D levels of those subjects who required multiple CRP (mean Otolin-1 = 666.9 pg/mL, mean Vitamin-D = 24.92 ng/mL)were compared with those who did not (mean Otolin-1 = 496 pg/mL, mean Vitamin-D = 20.21 ng/mL), a p values of 0.613 and 0.966 were obtained respectively for the same.
Serum Otolin-1 was not found to be significant with respect to age among the test(Otolin-1 v/s sex, p = 0.5303) and control groups (Otolin-1 v/s sex, p = 0.7734) respectively.
It was found that the majority of subjects in the test group belong to insufficient levels 13 (56.5%) followed by deficient and sufficient levels each 05 (21.7%). A similar observation was made in the control group with 18 (78.2%) belonging to insufficient level followed by deficient level 05 (21.7%) (Table 3). When Vitamin-D was compared with age and sex separately in both test and control groups respectively, there was no statistical significance found (p > 0.05). It was noted that the mean vitamin-D values in test subjects (22.67 ng/mL) was higher than that of the control subjects (15.43 ng/mL). Among the test subjects, four outliers were having vitamin-D values more than that of the average of the rest of the observations (52.1 ng/mL, 68.4 ng/mL, 52.9 ng/mL, and 42.8 ng/mL) belonged to the sufficient levels of vitamin-D. When these observations were eliminated, the mean of serum vitamin-D values reduced to 16.06 ng/mL which was comparable to that of the mean value of control subjects.
Showing Vitamin-D levels among subjects
A comparison of serum otolin-1 and vitamin-D of test and control subjects were made to see if there was any correlation of inner ear biomarker with the vitamin-D. (Fig. 1). A two-sample Wilcoxon Rank-Sum test was applied and the result was found statistically insignificant with Spearman’s correlation coefficient values of 0.1671, p = 0.4460 and –0.3114, p = 0.1480 in test and control groups respectively. The spearman’s correlation coefficient values after eliminating the 4 outlier subjects was 0.047 for test subjects with p = 0.8500.
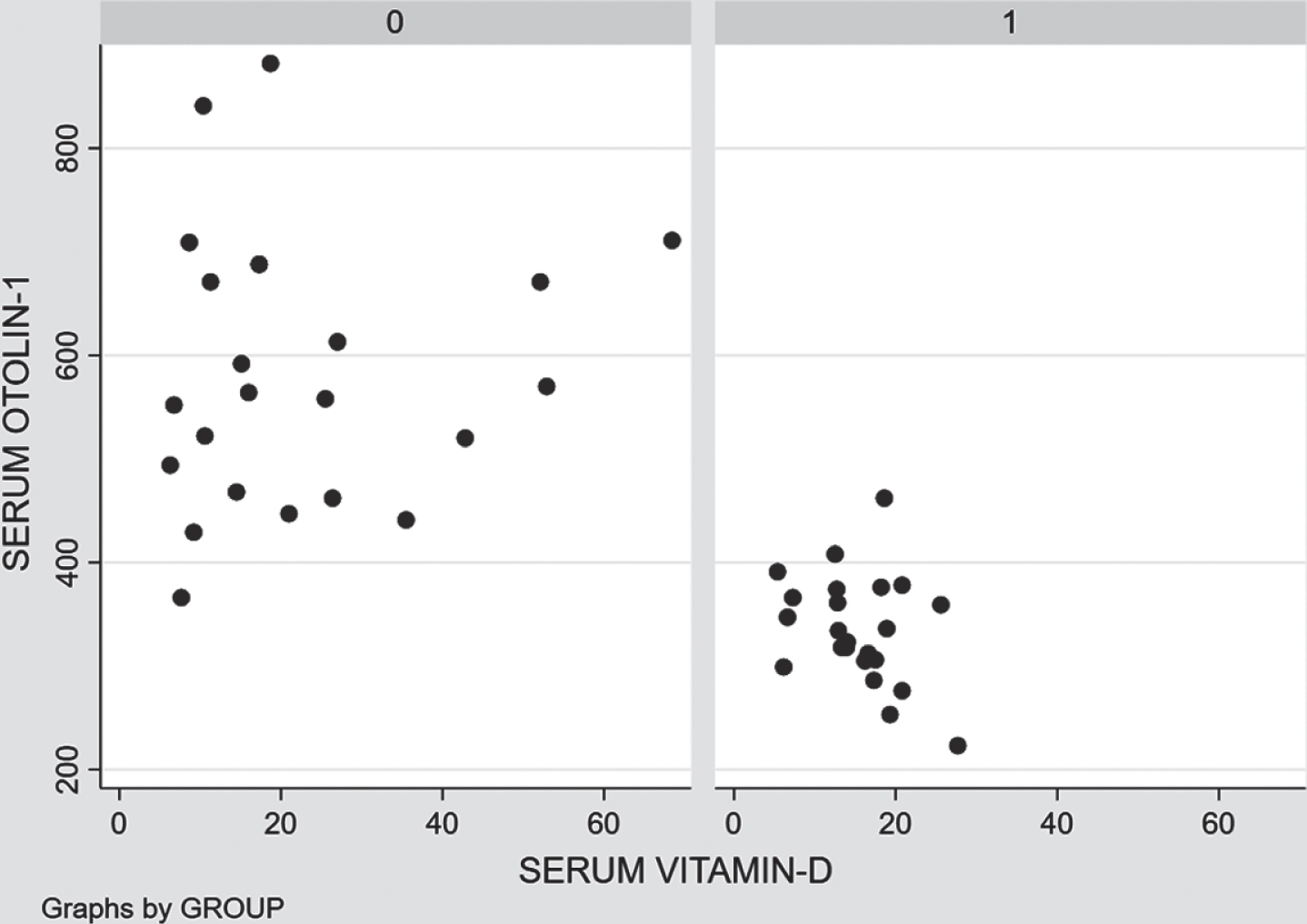
Scatter plot showing a correlation between otolin-1and Vitamin-D levels among Test group(0) and Control group(1). Spearman’s correlation coefficient values of 0.1671 and –0.3114 in test and control groups respectively.
In a situation when the Dix Hallpike test is negative or if there are contraindications to perform the test, the diagnosis of BPPV may be cumbersome to the clinician owing to the non-feasibility of doing the test and relying upon an alternate test [12]. A trained otorhinolaryngologist or neurologist may be required to carry out these tests, which is not always the ideal scenario in a country like India. Also after the canal reposition maneuver has been done, the patient may be required to undergo a repeat test to confirm the effectiveness of treatment. All these lead to an indirect economic burden over the patients due to multiple visits to clinics or hospitals. Hence there is a need for exploring the terrain of inner ear biomarkers, which may ease the diagnosis of the disease perhaps even disease modification if we are lucky. Even though this is a costly venture in the initial stages, once the role of inner ear proteins such as otolin-1 has been fully understood, the benefits may outscore the investment. With this hope, we conducted this study to explore the role of otolin-1 in BPPV. Since there is only limited evidence available in the literature regarding the otolin-1 and also owing to the cost factor for the test of analysis, we recruited BPPV patients who were positive for positional tests and tested their serum for otolin-1.
In our study, the mean duration of 2.45 days from the recent attack of BPPV to the time of sample collection for otolin-1, we were able to obtain significant results. Similarly, Wu et al. [28] reported a mean duration of 5.38 days for the sample collection for analysis of otolin-1. Owing to the fact that half-life of otolin-1 is unknown, this mean duration of sample collection in our study was likely sufficient enough since significant results were obtained. However, there is still a need for elucidating the half-life and the peripheral metabolism of these specific inner ear proteins in future studies for a better understanding of their behavior.
K. Parham et al. and Wu et al. [21, 28] showed that there was a significant rise in the levels of serum otolin-1 in the peripheral blood in BPPV patients as compared to normal. Our study supports the literature that there are indeed raised levels of otolin-1 in BPPV patients than that of controls following an attack of BPPV. We reported a significant otolin-1 level in BPPV patients compared to that of controls similar to Wu et al. [28] study.
A majority of our subjects were female patients belonging to the peri and post-menopausal age group. The pilot article Parham et.al reported a mean serum otolin-1 levels of 590 + /–45 pg/mL among 14 postmenopausal patients. Similarly, in our study, we had 9 postmenopausal females whose mean otolin-1 was 609.88 pg/mL which was significantly higher than that of controls. The deficiency in estradiol may be the risk factor [23].
The etiology in majority of our subjects was idiopathic BPPV followed by traumatic. We found that there was no significant difference between the otolin-1 levels among the idiopathic and post-trau-matic BPPV. This shows that the inner ear markers are not affected by the difference in the etiology of BPPV. However, the subjects belonging to our post trauma BPPV group were of low-velocity head injury, none requiring any hospital admission. Hence a definite assumption cannot be made unless the inner ear marker has been checked in patients with a high-velocity head injury requiring ICU care. Learning this difference may not affect the treatment outcome of the patient but may play a role in therapeutic monitoring of the inner ear health and explaining the prognosis to the patient post recovery from the primary injury.
Similarly, we had predominant subjects having posterior canal BPPV than horizontal canal BPPV. Although there is no evidence in the literature available, we tried to see if there was any association between the canal involved and the etiology of BPPV in the test group. No significant results were obtained. However, a definite comment cannot be made based on this study since the sample size was smaller. Larger predesigned studies may be able to answer this difference even though theoretically there may not be a significant difference in the amount or extent of damage to otoconia that occurs in PC-BPPV and HC-BPPV since the underlying pathophysiology for both the types remains the same.
The existing literature showed that the serum otolin-1 levels increases & vitamin D level reduces with advanced age [26, 29], especially after 70 years of age. To overcome this confounding factor in the current study, the cut-off age limit was set at 65 years of age. Within this preset age limit, we did not find any significant difference between the age and serum otolin-1 suggesting that the otolin-1 is more affected by the disease process rather than age in a middle-aged adult patient. Similarly, we did not find any significance between the sex and otolin-1, neither did the Parham et.al or Wu et.al groups. We found that otolin-1 was raised in the disesed individuals irrespective of the sex, even though BPPV is more prevalent in females.
52% (12 subjects) of those diagnosed with BPPV had a recurrence (symptoms of same canal involved, presenting after 2 weeks of initial treatment) of symptoms after having treated with an appropriate reposition maneuver. When these patients’ serum otolin-1 was compared with those whose symptoms did not recur, there was no significance obtained. However, the comment on the status of recurrence of BPPV and inner ear biomarkers could not be explained to the most satisfactory level in this study because the change in the trend of inner ear markers was not evaluated through the different stages of the disease. ie: the blood sample was drawn at only one point of time when the patient initially presented with symptoms at the time of recruitment to the study. A more appropriate meaning could have been obtained if the analysis was done at different stages of the disease. Larger sample size studies focussing on the activity of inner ear proteins in different stages of BPPV will probably answer this question in the future.
Canal shift and re-entry phenomenon are known to occur in patients undergoing reposition maneuvers as a treatment in BPPV [8]. We compared the corresponding otolin-1 and vitamin-D of those patients who had canal switch and those who did not, and the results were insignificant. A larger study and a long term follow up may be required to know the relationship between the inner ear marker and the canal switch post-treatment of BPPV.
The mean serum vitamin-D levels of the test group (22.671 ng/ml) were higher as compared to the control group (15.437 ng/ml), which may be attributed to the 4 outlier observation in the Test group individuals who had their vitamin-D levels more than the rest of the observations (belong to sufficiency levels) due to which there was an increase in average among the test. Upon eliminating the outliers, the mean vitamin-D levels of the test group individuals were comparable to that of the control group. The average in the test group dropped down from 22.67 ng/mL to 16.06 ng/mL. Mean vitamin-D values of both test and control groups belong to an “insufficiency and deficiency level” category, which does satisfy the criteria that the majority (about 90%) of the Indian population fall under the “insufficiency and deficiency level” range [20–24]. Our study did not focus to elicit the cause behind the low vitamin-D levels among the subjects, but sunlight would have played a major role. Probable reasons for low sunlight exposure in the subjects of our study would be an urban lifestyle, indoor working environment, and a possible social reason among the Indian female population. Larger study samples might give a better perspective on this subject.
The mean Vitamin-D levels of our test and control subjects did not have any statistically significant result when compared to age or sex. This may probably lead to a hypothesis that low levels of vitamin-D may require a contributing factor like osteoporosis and old age to potentiate the age-related degeneration of otoconia thus leading to BPPV [27, 29].
Further, there was no significance found between the vitamin-D levels and the otolin-1 protein. Parham et al. [20] showed that there was negative correlation between serum Vitamin-D and Otolin-1 in subjects above 70 years age, whereas in our study, among the test subjects (under age 65 years), we found that vitamin-D and otolin-1 had a positive correlation but was not statistically significant. Our study failed to provide the reason behind the increased Vitamin-D (within sufficient levels) among test subjects compared to control subjects and its role in BPPV. The probable cause for this would be a overall prevalence of low Vitamin-D among the general Indian population.
There are no studies in the literature which has tested the recurrence of BPPV with the levels of inner ear protein. We compared serum otolin-1 and vitamin-D between those requiring multiple CRP and those who did not, and there was no statistical significance obtained. The probable reason could be that the blood sample was drawn at only one point of time when the patient initially presented with symptoms at the time of recruitment. If a repeat sample of blood was analyzed for otolin-1 during the subsequent recurrent episodes to compare with the initial value, it would have helped better at understanding the fate of marker due to each attack of BPPV and thus can quantify the severity of the disease.
The research on the inner ear proteins is still in its preliminary stages, hence not much is known about the pharmacodynamics and pharmacokinetics of otolin -1. The half-life of the serum otolin-1 is not known, hence it cannot be predicted as to how long the inner ear proteins that are released into systemic circulation and will be available for the analysis. So far in the literature, it has not been described regarding the time for which the sample has to be collected from the BPPV patients for the analysis of the inner ear protein. Hence there is a need for focussing further studies on the peripheral metabolism of these specific inner ear proteins. Also the inner ear proteins may behave differently in different vestibular disorders and idiopathic sensorineural hearing loss and other diseases which needs further investigation.
Conclusion
This study has successfully explained the proposed hypothesis and aim of the study upon which the further foundation was laid that the serum otolin-1 may be a potential biomarker in BPPV patients. However, the role Vitamin-D with respect to inner ear biomarker could not be well explained in this study, a similar study in a general population whose mean Vitamin-D are within sufficient levels may provide a much better perspective to this aspect. The role of the otolin-1 in other inner ear disorders and the conditions predisposing to BPPV should be addressed in future studies.
Footnotes
Acknowledgments
Mr Mao Bhartiya –Audiologist, Department of Otorhinolaryngology and Head and Neck Surgery, All India Institute of Medical Sciences, New Delhi
Mr Mohan –Minor OT assistant, Department of Otorhinolaryngology and Head and Neck Surgery, All India Institute of Medical Sciences, New Delhi
Dr Sudhasini Panda –Research Fellow, Department of Biochemistry
Dr Shivam Pandey –Statistician, Department of Biostatistics, All India Institute of Medical Sciences, New Delhi
Conflicts of interest
No Conflicts of interest regarding this article.
Funding
This study was not funded by any Government or Private funding agency.