
Abstract
BACKGROUND:
Auditory cues might play a role in postural control.
OBJECTIVE:
The primary aim of this study was to investigate the association between white noise and head-shake (HS) related changes in postural sway.
METHODS:
Fifty healthy adults underwent Synapsys Posturography System (SPS) evaluation. The posturography (PG) evaluation consisted of two protocols: sensory organization test (SOT) and SOT with head-shake (HS) (HS-SOT). The standard SOT protocol of SPS involves a battery of six postural conditions. In the current study, participants underwent only four SOT conditions. The participants were asked to stand barefoot on the SPS platform (static platform and foam). The SOT standing conditions were as follow: (1) firm surface (force platform only) with eyes open (SOT1); (2) firm surface with eyes closed (SOT2); (3) foam surface (which was positioned on the force platform) with eyes open (SOT4); and (4) foam surface with eyes closed (SOT5). For the HS-SOT protocol, we asked the participants to move their heads left and right (i.e., yaw head rotation) in the mentioned SOT conditions. Each postural condition was 10 seconds long. Both SOT and HS-SOT postural conditions were conducted across the two hearing modes of silence and noise. To achieve our aims, comparison of sway parameters between SOT and HS-SOT, and between hearing modes were considered.
RESULTS:
White noise was associated with a reduction in postural sway. The reduction observed in sway area, sway amplitude, and sway frequency. Moreover, HS significantly increased postural sway in all HS-SOT conditions compared to their SOT equivalents (i.e., HS-SOT1 compared to SOT1, etc.). The presence of white noise was associated with a decrease in the HS-related increase in postural sway.
CONCLUSIONS:
Considering the results, this study adds to the body of literature suggesting that white noise contributes to postural control, and the implications of this for rehabilitation need to be further investigated.
Introduction
Postural control is a complex sensorimotor and cognitive skill that requires the integration of multisensory information from visual, vestibular, somatosensory, and auditory systems [10, 25]. Posturography (PG) is a method for quantitatively assessing an individual’s postural control using a force-plate technology [4]. By analyzing the center of pressure (COP), PG measures the direction, amplitude, velocity and frequency of postural sway [6]. The Sensory organization test (SOT) protocol of PG involves a battery of conditions for assessing the person’s ability to effectively use visual, vestibular, and/or somatosensory inputs to maintain postural control while standing on a force platform [20].
The contribution of somatosensory, vestibular, and visual inputs to postural control is well documented [23]. As has been demonstrated, a fourth neural input (i.e. auditory cues), also contributes to postural control [3, 32]. However, the literature concerning the association between auditory cues and postural control is inconsistent. Several studies used earplugs to reduce auditory cues in healthy adults. They resulted in an increase [12, 32] or no change [2] in postural sway. Moreover, studies regarding the relationship between stationary narrowband noise/pure tone and postural control were somehow inconsistent and showed an increase [24], a decrease [7, 28] or no change [19] in postural sway. Furthermore, studies of moving and rotating sounds showed increased [1, 29] or reduced postural sway [8, 32].
Nevertheless, these studies have investigated the association between white noise and postural control only through eliminating or disturbing visual and/or somatosensory inputs (i.e., standing on the floor or foam with eyes open or closed). The Head-shake (HS) SOT (HS-SOT) is a modification to the standard SOT, which is primarily used to identify impairments in a subject’s ability to effectively use vestibular inputs for postural control while simultaneously moving the head [4]. It uses dynamic head movements around body axes, including yaw, pitch, and roll head rotations which challenge the vestibular system by generating a vestibular stimulus in addition to that generated by the subject’s sway [20, 21]. In the study by Paloski et al. [22], dynamic head movements in the pitch and roll planes resulted in increased postural sway.
Horizontal head movements, among the others, are more likely relevant to the routine activities of daily life [20]. Because we steer and guide our changes in locomotion direction with horizontal eye and head turns, horizontal movements make up a substantial portion of the head movements associated with daily postural control activities [20].
Given the above, the first aim of the current study was to further investigate the association between auditory cues and postural control in normal adults using stationary white noise. More importantly, we aimed to challenge the postural control system by disturbing vestibular cues (i.e., using HS in the yaw axis) to study the relationships between white noise and HS-related changes in postural sway (i.e., vestibular disturbance’s influence on postural control).
Subjects, materials and methods
Study design
This comparative cross-sectional study conducted in the Audiology Ward of Rofeideh Rehabilitation Hospital, Tehran, Iran. All participants were college students and willing to participate (Convenience sampling). The Ethics Committee of University of Social Welfare and Rehabilitation Sciences (USWR) approved the study protocol (ethical code: IR.USWR.REC.1398.073), and the study was performed according to the Declaration of Helsinki and amendments (2013).
Subjects
Fifty healthy individuals (32 females and 18 males; age range of 18–35y) with a mean age, weight, and height of 25.84 years (3.89), 69.40 kg (± 11.43), and 172.49 cm (± 8.71), respectively, participated in this study. The participants signed a written informed consent, and completed a medical history form. The participants reported no previous history of vertigo, dizziness, imbalance, or falls. All subjects underwent otoscopy, impedance audiometry (AT235, Interacoustics, impedance audiometer), speech and conventional pure-tone audiometry (PTA over 250 to 8000 Hz; AC440, Interacoustics Denmark audiometer), vestibular bedside examinations, including Romberg and tandem stance tests, and video head impulse test (VHIT) (Synapsys VHIT, SYNAPSYS, Inventis Company, Italy). The results of the auditory and vestibular assessments were normal in all the participants. After instructing, the subjects underwent PG evaluation.
PG evaluation
The participants were assessed using Synapsys Posturography System (SPS) (SYNAPSYS, Inventis Company, Italy). The participants were asked to stand barefoot on the SPS force platform, with their feet parallel and apart (using a triangle-shape foot positioner), and their hands by their sides in 8 postural scenarios. The SPS force platform includes three pressure sensors and is capable of capturing successive positions of the center of pressure at 100 Hz. The 8 postural scenarios included 4 SOT and 4 HS-SOT conditions across two different hearing modes in a semi-anechoic room. This semi-anechoic room was part of the hospital’s audiology ward, which is used for research when the environment is somewhat calmer. Whilst the semi-anechoic room used in our study provided a sound-limited environment, some low-level ambient sound was also produced by the hardware used during the study. Moreover, there was some background noise in the environment. Ambient noise is any sound other than the sound being monitored (primary sound). The sound level of the room (due to the hardware and environmental sounds) was about 40–45 dB dBA, as was measured by SLM (TES-1358C, Obsnap Instruments, Taiwan). The hearing modes were: A) Silence mode: the semi-anechoic room without white noise; and B) Noise mode: the same semi-anechoic room with white noise (10–10000 Hz) presented from a front loudspeaker (0° azimuths) 100 cm away (at 75dBA) as long as each postural trial (15 seconds).
The SOT standing conditions were as follow: (1) firm surface (force platform only) with eyes open (SOT1); (2) firm surface with eyes closed (SOT2); (3) foam surface (which was positioned on the force platform with the length, width, and height of 50, 50, and 6 cm, respectively) with eyes open (SOT4); and (4) foam surface with eyes closed (SOT5). For HS-SOT test, we asked the participants to move their heads left and right (i.e., yaw head rotation) in the mentioned SOT conditions. Figure 1 is a schematic of the person’s position in the present study.
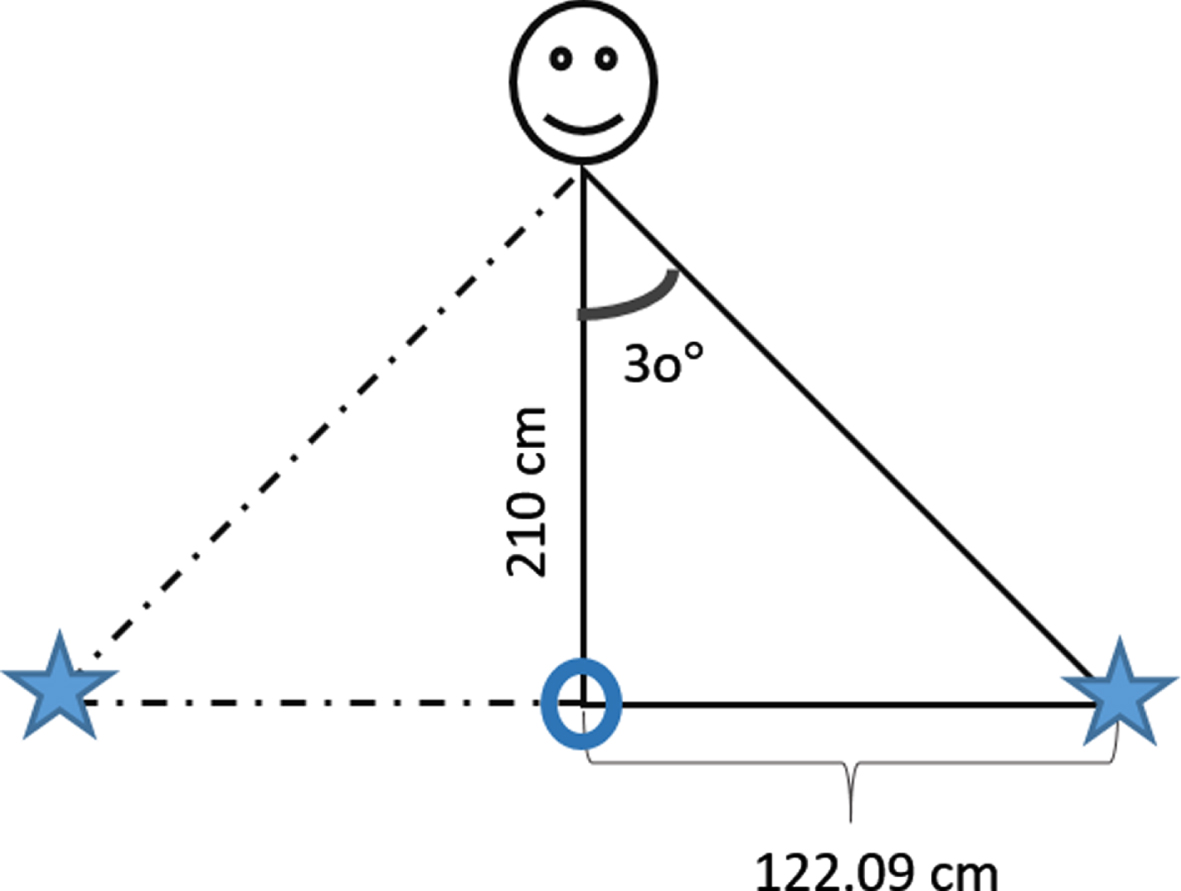
The peak point of the triangle is the location of the individual on the platform, and the base of the triangle is the wall in front of the person. The other two apexes of the triangle that have been marked with an asterisk are the points that were marked on the wall in front of the participant to determine the range of individual’s head motion. According to the distance of the person from the wall (210 cm) and the change of the person’s head angle from the middle line (±30°), the range of the head motion was calculated.
To unify the speed of the head movement among individuals, we used a researcher-made amplitude modulation (AM) sound with a frequency of 2 Hz. The AM sound was presented only in the training stage (the first 5 seconds of each HS-SOT condition) to help the participants adjust the speed of their head movement with the speed of the stimulus. The order of the silence examinations was SOT1, HS-SOT1, SOT2, HS-SOT2, SOT4, HS-SOT4, SOT5, and HS-SOT5, respectively. After that, the noise examinations performed in the same order.
In total, each participant completed 32 trials. Each standing condition (16 items) was repeated two times and the average value of each postural condition for each participant was retained. The exact time of each postural trial was 10 seconds with a pre-stimulus time of 5 seconds to prepare the participant (the training stage). Following each condition, a break of 15 seconds was considered while the person was standing in her place on the platform. Moreover, after the silence examinations, the participants were given a 5-min rest.
Following an acquisition, the SPS program laun-ched a series of calculation. The parameters of postural sway including sway area (SA) of the COP, anterior-posterior (AP) and lateral (LAT) (i.e., medio-lateral) amplitude (or displacement), and AP and LAT Fast Fourier Transform (FFT) in three frequency areas (Low: 0–0.5 Hz, Medium: 0.5–2 Hz, and High: 2–20 Hz) evaluated in all postural conditions across both hearing modes. SA is the area of the participant’s COP displacement during the time of recording (i.e. 10 sec). AP and LAT amplitudes are the mean positions of the person’s COP in the AP and LAT planes, respectively, during the recording time. FFT is the amount of sway energy in the mentioned frequency areas in AP and LAT planes during the recording time (in terms of mm2.s).
To investigate the association between white noise and postural control, we compared the mentioned sway parameters of the SOT and HS-SOT conditions between the two hearing modes (i.e., SOT1 in noise with SOT1 in silence, HS-SOT1 in noise with HS-SOT1 in silence, etc.) (Please see part 3.1.2, Tables 1–4, Fig. 2-Fig. 3).
Comparison of sway area between different postural conditions
Comparison of sway area between different postural conditions
Comparison of sway area between noise and silence hearing conditions
Comparison of mean AP amplitude between noise and silence hearing conditions
Comparison of mean LAT amplitude between noise and silence hearing conditions
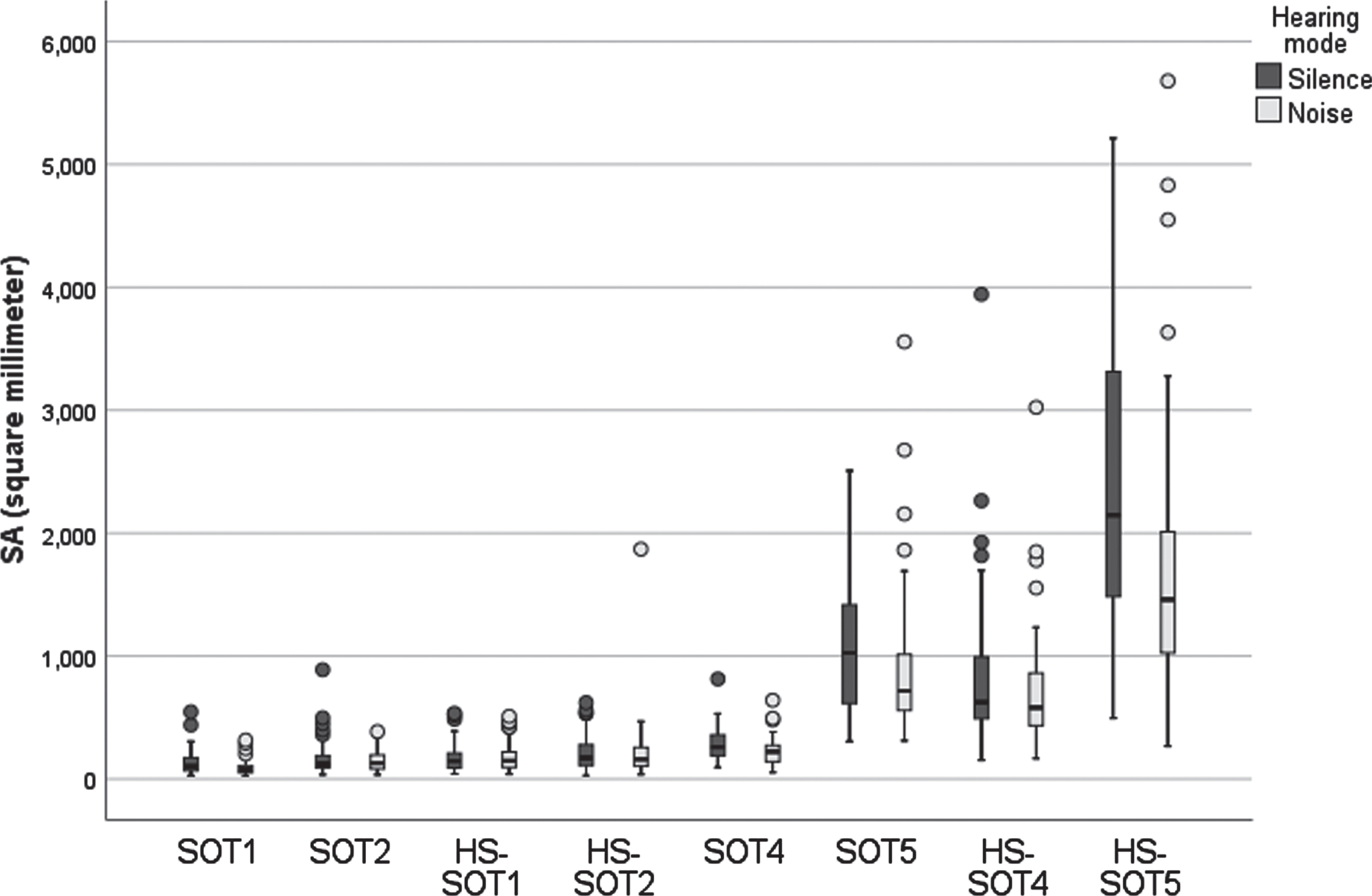
Box plot of SA in eight SOT and HS-SOT postural conditions across two hearing modes of silence and noise.
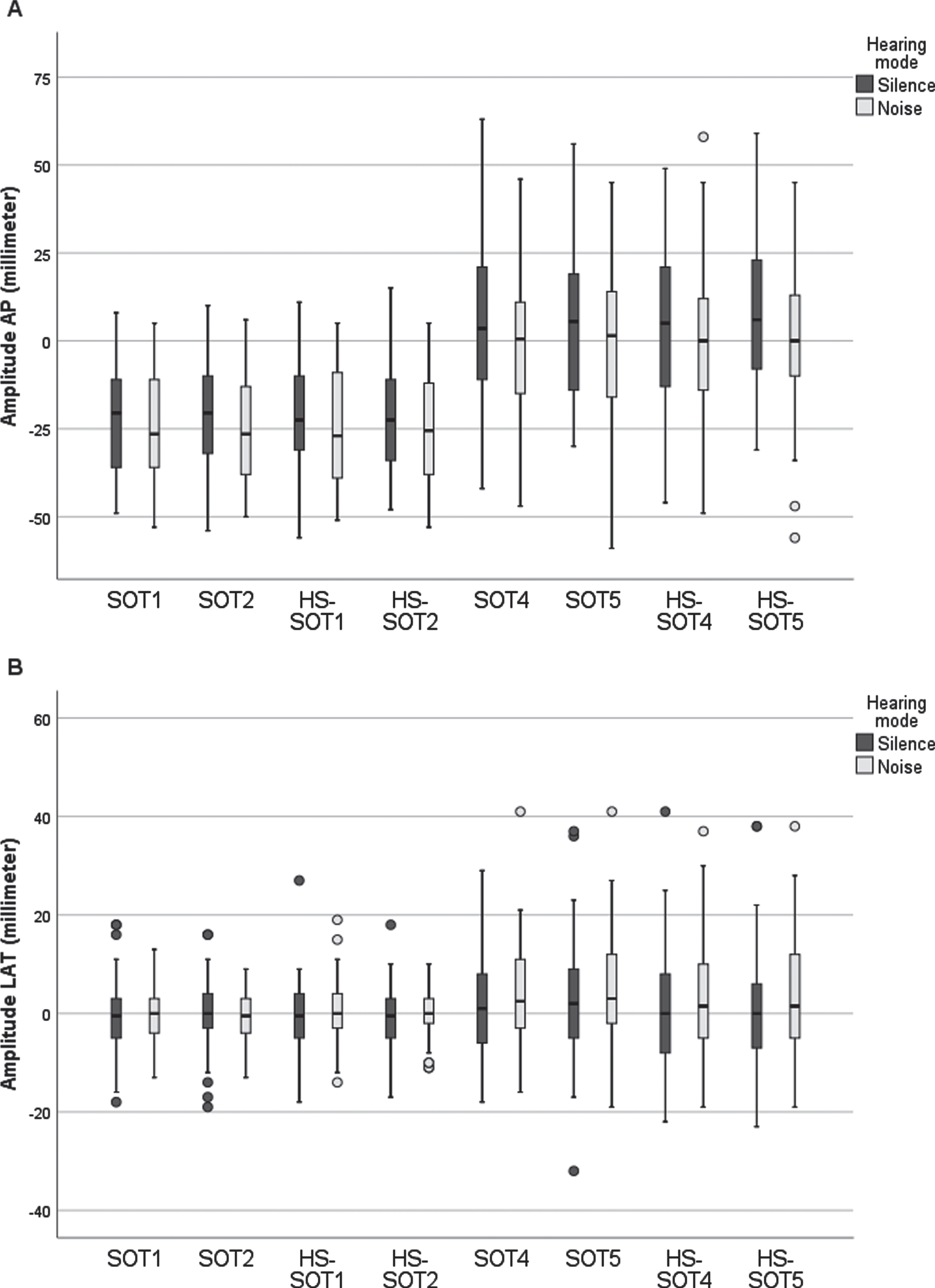
Box plot of AP amplitudes (A) and LAT amplitudes (B) in eight SOT and HS-SOT postural conditions across two hearing modes of silence and noise.
It is assumed that low frequencies account for visuo-vestibular regulation (0–0.5 Hz), medium frequencies for cerebellar participation (0.5–2 Hz), and high frequencies for proprioceptive participation (> 2 Hz) [15]. To investigate the effects of SOT/HS-SOT and hearing modes on this spectral view of postural system, we analyzed FFT in AP and LAT planes (please see part 3.1.2; Tables 5–8; and Fig. 4).
Comparison of AP FFT (in low and medium frequency areas) between noise and silence hearing conditions
Comparison of AP FFT (in high frequency area) between noise and silence hearing conditions
Comparison of LAT FFT (in low and medium frequency areas) between noise and silence hearing conditions
Comparison of LAT FFT (in high frequency area) between noise and silence hearing conditions

Box plot of AP FFT (0–0.5 Hz) (A) and LAT FFT (0–0.5 Hz) (B) in eight SOT and HS-SOT postural conditions across two hearing modes of silence and noise.
The association between HS and postural sway was assessed by comparing the SA values of HS-SOT postural conditions with their equivalent SOT conditions both in the silence and noise modes, separately (for the silence mode: HS-SOT1 to SOT1, HS-SOT2 to SOT2, HS-SOT3 to SOT3, and HS-SOT4 to SOT4; the same for the noise mode) (Table 9). Given that in HS-SOT compared to SOT, all conditions are the same, and only the movement of the head is added, so the result of the comparison can be an estimate of the effect of head movement. Furthermore, as was mentioned above, HS was performed at a frequency of 2 Hz.
Comparison of SA values (median ± IQR) between HS-SOT and SOT in silence and in noise using Wilcoxon test
The association between white noise and the HS-related changes in postural sway was determined using a division method. Therefore, our division method is nearly equivalent to the ratio method used in original computerized dynamic posturography (CDP) for calculating sensory analysis scores (SOM, VIS, VEST, PREF) [31]. In this method, the SA values of SOT and HS-SOT conditions were divided (Table 10); and then the resulting quotients were compared between the two hearing modes (Table 11 and Table 12).
Division method. Sway area (SA) values (median ± IQR) used for calculating the divisions (the first division up to the sixth division) in both hearing modes of silence and noise
SOT: Sensory organization test; HS-SOT: Head-shake SOT; SA: Sway area.
Comparing the results of “Division method” for corresponding divisions of SOT and HS-SOT in both hearing modes of silence and noise using Wilcoxon test
SOT: Sensory organization test; HS-SOT: Head-shake SOT; SA: Sway area.
Comparing the results of “Division method” for corresponding divisions of SOT or HS-SOT between hearing modes of silence and noise using Wilcoxon test
SOT: Sensory organization test; HS-SOT: Head-shake SOT; SA: Sway area.
The data were statistically analyzed using SPSS 23.0 software (IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp). Kolmo-gorov-Smirnov test was used for controlling the normality of data, and it showed the abnormal distribution of the data. Therefore, Wilcoxon test was performed for following comparisons:
The difference of responses (SA values and AP, and LAT amplitudes) between the noise and silence modes for investigating the association between white noise and postural control (please see part 3.1.2; Tables 1–4; and Fig. 2-Fig. 3). The difference of responses between the noise and silence modes from the spectral point of view by analyzing FFTs in AP and LAT planes (please see part 3.1.2; Tables 5–8; and Fig. 4). The difference between the SA values of HS-SOT postural conditions with their equivalent SOT conditions both in the silence and noise modes, separately, for evaluating the association between HS and postural sway (please see part 3.2.1; Table 9). The difference between the quotients (resulted from the division method) of the noise and silence modes for assessing the association between white noise and the HS-related changes in postural sway (please see part 3.2.2; Ta-ble 10–Table 12).
It should be noted that all values reported in the figures and tables were expressed as median ± IQRs. Moreover, a p-value (P) of less than 0.05 was considered as statistically significant for all comparisons.
Results
The results of this study are presented in two categories:
The effect of changes in sensory inputs on postural sway and the association between white noise and postural control
The effect of changes in sensory inputs on postural sway
As shown in Table 1, the elimination or distortion of sensory inputs increased the SA value and hence postural sway in all postural conditions in both silence and noise modes (SOT2, SOT4 and SOT5 compared to SOT1; HS-SOT1, HS-SOT2, HS-SOT4, and HS-SOT5 compared to SOT1).
The association the association between white noise and postural control
As shown in Table 2, the comparison of the SA values between the noise and silence modes showed a statistically significant reduction in postural sway in the presence of white noise in the following postural conditions: SOT1 (P = 0.001), SOT4 (P = 0.023), SOT5 (P = 0.016), and HS-SOT5 (P = 0.000). This has also been depicted in Fig. 2.
The AP amplitudes of the noise mode significantly decreased in the following postural conditions compared to the silence mode: SOT2 (P = 0.007), SOT4 (P = 0.014), SOT5 (P = 0.029), HS-SOT1 (P = 0.009), HS-SOT2 (P = 0.011), and HS-SOT5 (P = 0.006) (Table 3). According to Table 4, there were no statistically significant differences in the LAT amplitudes between the two hearing modes. These have also been shown in Fig. 3A and Fig. 3B.
As has been displayed in Table 5, the AP FFT (0–0.5 Hz) of the noise mode significantly decreased in the SOT1 (P = 0.000) compared to the silence mode. AP FFT (0.5–2 Hz) values significantly decreased in the noise mode in the following conditions: SOT5 (P = 0.003), HS-SOT1 (P = 0.015), and HS-SOT5 (P = 0.000) compared to the silence mode. Moreover, AP FFT (2–20 Hz) values showed a significant reduction in the HS-SOT1 and HS-SOT5 conditions (Table 6). This has also been demonstrated in Fig. 4A.
As shown in Table 7, the analysis of LAT FFT in the noise mode showed a significant reduction in the SOT1 (P = 0.017) and HS-SOT5 (P = 0.001) conditions for low frequencies (0–0.5 Hz) and in the SOT4 (P = 0.002) and SOT5 (P = 0.008) for medium frequencies (0.5–2 Hz) compared to the silence mode. In addition, LAT FFT (2–20 Hz) significantly reduced in the SOT5 and HS-SOT5 conditions (Table 8). This is also shown in Fig. 4B.
The effect of HS on postural sway and the association of white noise with HS-related changes in postural sway
The effect of HS on postural sway
As shown in the Table 9, HS was associated with a statistically significant increase in postural sway in all HS-SOT conditions compared to their SOT equivalents in both the silence and noise modes (i.e., HS-SOT1 compared to SOT1 in the silence noise modes, HS-SOT2 to SOT2, etc.) (P < 0.05).
The association of white noise with HS-related changes in postural sway
Table 10 shows the division method. SA values (median ± IQR) used for calculating the divisions (the Division 1 up to Division 6) in both hearing modes of silence and noise. Table 11 using the results of the division method, compares HS-SOT data with SOT data for each hearing modes. Based on Table 11, only two comparisons were not statistically significant: comparison of Division 4 with Division 1 in silence (head-shaking plus visual disturbance in silence; or, availability of somatosensory input in silence), and comparison of Division 6 with Division 3 in noise (head-shaking plus somatosensory disturbance plus visual disturbance in noise; or availability of auditory input for postural control). Table 12 using the results of the division method, compares SOT data in silence with the same data in noise, and HS-SOT data in silence with the same data in noise. Based on Table 12, presence of noise has its statistically significant effect in only Division 6 (or availability of auditory input for postural control; P = 0.004).
Discussion
The contribution of somatosensory, vestibular, and visual inputs to postural control is well documented [23]. According to studies, auditory cues play role in postural control [3, 32]. In the present study, fifty healthy individuals underwent 4 SOT and 4 HS-SOT conditions in two hearing modes, including silence and noise. Our results showed that white noise is associated with a reduction in postural sway while standing upright. Furthermore, white noise is associated with a decrease in the HS-related increase in postural sway.
The effect of changes in sensory inputs on postural sway and the association between white noise and postural control
In the current study, postural sway increased when sensory input was limited in all postural conditions, corroborating the commonly held hypothesis that the control of postural sway depends on the amount of available sensory feedback by somatosensory, vestibular, and visual systems [11, 23]. Postural sway is sensitive to subtle changes in sensory feedback, and increased availability of information from sensory systems has been shown to improve the control of upright stance [25]. Similarly, the current results showed that white noise from a stationary sound source is associated with a reduction in postural sway, and this influence (i.e., the noise-related reduction in postural sway) was greater during challenging conditions when postural tasks’ difficulty increases (i.e., less sensory information from other sensory systems is available). In agreement with the present results, previous studies have also shown that the presence of white/pink noise from a fixed-sound source is associated with a decrease in postural sway in healthy adults.
Zhong and Yost [33] showed a substantial reduction in head sway with white noise from a front speaker during Tandem Romberg and Fukuda Stepping tests with closed eyes in participants with normal hearing and vestibular functions. Ross et al. [25, 26] showed an improvement in postural stability with white noise in healthy young adults and adults over 65 years using headphones while standing on a force platform, regardless of the visual condition (eyes open or closed). In the study by Stevens et al. [30], white noise was also associated with reduced postural sway while standing on a balance platform when eyes were closed. In the present study, similar to the previous studies, auditory cues were provided by presenting a white noise at a comfortable and audible level (75 dBA) from a fixed external sound source in healthy adults. These similarities in terms of the participant group, the acoustic input, and experimental setup could underlie the consistency of our results with these studies.
The proposed mechanisms for linking the auditory cues with postural control improvement
Although the exact mechanism is not yet clear, several explanations have been proposed regarding the link between auditory cues and their role in improving postural control. One explanation is called “auditory anchorage theory.” According to this theory, auditory cues from stationary sound sources provide spatial information to help the brain to structure a spatial image of the environment. The nervous system then uses that information to position the body in space and maintain the posture [16, 33]. As Lubetzky et al. [16] demonstrated, “the use of an auditory anchor is supported by studies demonstrating that stationary sound sources and addition of sound sources helped reduce sway, whereas sound attenuation increased sway.” However, this theory does not explain the reduction in sway in all settings, for example, with rotating and moving sounds. In the study of Gandemer et al. [8, 9], rotating white noise, presented via an array of speakers (16 speakers) around the participant rather than a fixed source or headphone, significantly decreased postural sway. Also, Vitkovic et al. [32] reported reduced postural sway with white noise moved in the frontal plane across a semicircular array of 8 speakers. Karim et al [13] reported that a stationary white noise source had to be earth-referenced rather than head-referenced (speakers rather than headphones) to improve performance on a dynamic task. However, Ross and Balasubramaniam [25, 26] observed a substantial reduction of sway with white noise in young adults [26] and in young and older adults [25] via headphones.
Another explanation is increased attentional arousal when noise is presented, in which the presence of noise can lead to reliance on more automatic control processes, which results in reduced postural sway and improved stability [25]. Stevens et al. [30], for example, related the improvement in postural control seen with sound to increased attention or an alerting effect of the sound. Nonetheless, passively listening to noise does not improve cognitive load and hence attention; thus, it is unlikely that passive attention in the noise could reduce sway [16, 25].
The last hypothesis is stochastic resonance (SR), ” which describes the amplification of signals when adding noise to a system with threshold, such as the nervous system [25]. According to this theory, stochastic noise in one modality enhances the detection and processing of a weak signal in another modality. Maheu et al. [17] demonstrated that the presence of pink noise might have led to an enhanced detection of residual somatosensory inputs (i.e., weak somatosensory signals) resulting in a decrease in postural sway.
In the present study, somatosensory inputs were not entirely absent. In addition, the reduction that occurred in the presence of the white noise was mostly significant in postural conditions were somatosensory inputs were decreased, with or without visual cues. Thus, it is possible that the presence of white noise could have enhanced the detection and processing of the residual somatosensory cues, leading to a decrement in postural sway. However, this idea needs to be investigated in future studies.
The effect of HS on postural sway and the association of white noise with HS-related changes in postural sway
In the present study, HS was associated with an increase in postural sway in all HS-SOT conditions compared to their SOT equivalents in both the silence and noise modes (Table 9). Head movement alters the acoustic signals at the two ears and changes interaural time difference, interaural level difference, and spectral distribution. As a result, the brain notices that the movement toward a certain direction is larger and orders the body to adjust in the opposite direction, which, in turn, reduces head and body movements [33]. In agreement with this view, in the current study, white noise decreased the destabilizing effect of HS (Table 10). This probably indicates that the impact of the noise on the postural sway’ reduction depends on the extent of the available somatosensory, vestibular and/or visual inputs. In other words, the noise-related reduction in postural sway is more remarkable when postural tasks’ difficulty increases (i.e., less sensory information from other sensory systems is available), which is in agreement with Dozza et al. [5], Vitkovic et al. [32], and Stevens et al. [30].
When less sensory information is available, auditory cues play a more significant role in decreasing postural sway (Table 12). To put it another way, for example, in the absence of visual and somatosensory inputs (SOT5), the CNS relies more on the auditory cues, suggesting that the CNS might consider the auditory cues as other sensory inputs that classically contribute to postural control. Likewise, Vitkovic et al. [32] and Stevens et al. [30] demonstrated that hearing-impaired subjects with concomitant vestibular dysfunction rely on auditory cues to a greater degree than the hearing-loss subjects without vestibular deficits to facilitate their balance, which may reflect an increase in auditory sensory weighting when the sensory redundancy is decreased.
By eliminating the visual input alone, the effect of head movement on postural sway is not significant (Table 11, by comparing Division 4 with Division 1 in silence). Head movement nearly doubles the SA (Table 10), whether by disturbing the somatosensory information or disturbing both the somatosensory and visual inputs, which verifies that eliminating visual information does not exert any synergistic influence on the postural sway, resulted from head movement (Table 11, by comparing Division 5 and 6 with Division 2 and 3 in silence, respectively). However, justifying these findings based on the above theories or another theory needs to be investigated in the future studies.
The association between stationary white noise and sensory reweighting
Sensory reweighting is a critical component of postural control [10]. Several studies have reported that CNS re-weighs its relative sensory dependence on somatosensory, vestibular, and visual senses when the sensory context and availability of information from these senses changes [5, 32]. In the present study, white noise was associated with a decrease in the difference in SA between HS and HS-free conditions when somatosensory and/or visual inputs were absent, which, in turn, reflects an increase in auditory sensory weighting to enhance the use of auditory cues when the sensory redundancy decreases.
Limitations and recommendations
The results of our study imply that auditory cues are associated with a decrease in postural sway and hence improved postural control; however, there are limitations to the current study. First, though we used the SPS, we did not exactly follow the SPS’s protocol in terms of the number of postural conditions of its SOT assessment, which includes six postural test conditions, the number of repetition of each standing condition, and the duration of each trial, which is 20 second. We only conducted four postural conditions of the SOT, each standing condition was repeated two times, and each trial lasted 10 seconds. Second, the silence and white noise conditions were not randomized. Thus, there is a chance that the benefit of white noise (i.e., reduction in postural sway) was partly due to a learning effect.
Therefore, future studies are needed to investigate the relationship between white noise (or auditory cues in general) and postural control in clinical populations, such as patients with vestibular dysfunction, using the full SOT protocol of posturography and more detailed analysis in low-frequency FFT. The same studies with pitch and roll head movements are also advisable. Finally, galvanic vestibular stimulation could be an option (instead of head-shake) to disturb the normal flow of vestibular inputs to the postural control system.
Conclusion
Considering the results, white noise from a stationary external sound source is associated with improved postural control. It is associated with a decrease in the HS-related increase in postural sway. These results suggest that the auditory cues are important to consider for planning the rehabilitative programs in patients with postural control disorders.