
Abstract
BACKGROUND:
Parkinson’s disease (PD) is a common multi-system neurodegenerative disorder with possible vestibular system dysfunction, but prior vestibular function test findings are equivocal.
OBJECTIVE:
To report and compare vestibulo-ocular reflex (VOR) gain as measured by the video head impulse test (vHIT) in participants with PD, including tremor dominant and postural instability/gait dysfunction phenotypes, with healthy controls (HC).
METHODS:
Forty participants with PD and 40 age- and gender-matched HC had their vestibular function assessed. Lateral and vertical semicircular canal VOR gains were measured with vHIT. VOR canal gains between PD participants and HC were compared with independent samples t-tests. Two distinct PD phenotypes were compared to HC using Tukey’s ANOVA. The relationship of VOR gain with PD duration, phenotype, severity and age were investigated using logistic regression.
RESULTS:
There were no significant differences between groups in vHIT VOR gain for lateral or vertical canals. There was no evidence of an effect of PD severity, phenotype or age on VOR gains in the PD group.
CONCLUSION:
The impulsive angular VOR pathways are not significantly affected by the pathophysiological changes associated with mild to moderate PD.
ABBREVIATIONS
Healthy controls Indeterminate phenotype Left anterior right posterior canal plane Lateral canal Parkinson’s disease Postural instability/gait dysfunction phenotype People with Parkinson’s disease Right anterior left posterior canal plane Semicircular canal Tremor dominant phenotype Vertical canals Video Head Impulse Test Vestibulo-ocular reflex Vestibular nuclear complex Vestibulo-spinal reflex
Introduction
For over 50 years [1], researchers have hypothesised that dysfunction of the vestibular pathways may contribute to the balance deficits and elevated falls prevalence [2] noted in the common neurodegenerative disorder, Parkinson’s disease (PD).
Recent brainstem morphological studies have supported this hypothesis by reporting the significant presence of PD-related Lewy bodies, Lewy nitrites and oligodendroglial bodies in all four of the major vestibular sub-nuclei in the vestibular nuclear complex (VNC) as well as in the root of the vestibular nerve in people with PD (PwPD) [3]. Another study demonstrated reduced expression of an important cytostructural protein and increased neurodegeneration related somatic lipofuscin selectively affecting the Deiters’ nucleus in the lateral vestibular nucleus in PD compared to control samples [4]. Other brainstem nuclei associated with the vestibular system and known to be affected by physical and metabolic changes associated with PD are the dorsal raphe nucleus and locus coeruleus. These nuclei are involved in vestibular-related interoceptive circuits and vestibular sensorimotor pathways [5] and have descending inputs into the VNC [3]. The pedunculopontine nucleus, with roles in modulating posture and locomotion, arousal, attention and learning [6], also has descending input into the VNC and has been shown to have physical and metabolic changes associated with PD [3]. Ascending vestibular pathways include projections to the thalamus and cortex as well to the striatum and basal ganglia (BG) [7], brain regions primarily affected by PD. Lastly, dopamine is known to be a neurotransmitter in the vestibular nuclei, albeit one of the less prevalent, and is also one of the many known chemical mediators in the ascending central vestibular pathways [5]. To our knowledge, no studies have specifically reported on any potential differences in morphological changes in the vestibular periphery with PD compared to age-matched samples.
Despite this fairly compelling evidence of PD-re-lated pathological changes in central vestibular pathways, a recent review [7] highlights the conflicting findings of vestibular function testing in the PD population. Vestibulo-ocular reflexes (VOR) in PwPD have been widely tested via the non-physiological very low-frequency stimulus of bi-thermal caloric stimulation measured with electronystagmography. However, findings varied widely between studies, with some reporting significantly reduced or absent responses [8, 9] while others report abnormally increased responses in PD compared to HC [1, 10].
Surprisingly, the video Head Impulse Test (vHIT), one of the most commonly utilised measures of impulsive angular VOR and vestibular semicircular canal (SCC) function in clinical practice for both peripheral and central vestibular disorders [11, 12], has scarcely been evaluated in the PD population [13, 14], and findings to date conflict. Lv et al. [13] compared horizontal/lateral canal (LC) vHIT VOR gains in 63 people with PD and 56 age-matched HC, and unexpectedly found higher VOR gains in the PD group (mean≥1.20) compared to HC (mean 0.98), particularly for the tremor dominant (TD) phenotype (gains up to 1.80). In contrast, a recent study by Scarpa et al. [14] involving 15 PD subjects and 20 age-matched HC reported that only two PD subjects (13%) had abnormal vHIT, both with reduced VOR gain and corrective saccades. vHIT findings have not previously been reported for vertical canal (VC) VOR gains in PD.
Knowledge of the presence of specific impulsive VOR dysfunction in PD would help guide targeted vestibular rehabilitation therapy protocols and potentially reduce postural imbalance and falls by improving gaze stability during head motion. Currently, vestibular specific rehabilitation is not commonly a focus in PD exercise programmes despite the often-reported symptoms of vestibular, visual, and oculomotor dysfunction in PD [15].
Therefore, the aim of this study was to identify whether people with PD have higher incidence of SCC mediated VOR dysfunction compared to age-matched HC as determined by vHIT-obtained VOR canal gains for all six semicircular canals. A secondary aim was to examine whether PD severity, phenotype, age and disease duration influenced canal VOR gains.
Patients and methods
Data were collected between February 2018 and August 2019 on 40 participants with PD and 40 age-matched healthy controls. Eligible participants were community-dwelling volunteers with no known history of vestibular disorders and aged between 50–80 years old; PD participants had neurologist-diagnosed idiopathic PD. Exclusion criteria were known dementia, prior known vestibular dysfunction, severe visual impairment, known neurological conditions (apart from PD), MMSE≤24, < 20° of neck rotation range of motion or pain during head turn, and diagnosis of atypical PD. Ethical approval for this study was granted by the University of Sydney Human Ethics review board (Protocol number: 2017/925). Participants gave written informed consent prior to study enrolment.
PD participants were tested during the ON phase of their usual antiparkinsonian medication schedule. Demographic information obtained from all participants included age; regular medication use; previous 12 months falls history; fear of falling as quantified by the Falls Efficacy Scale –International Questionnaire [16]; and cognitive status as quantified by the Mini-Mental State Examination (MMSE). Time since PD diagnosis; and freezing of gait (FOG) status as determined by Part 1 of the New Freezing of Gait Questionnaire (N-FOGQ) [17]; were also obtained from PD participants. A trained physiotherapist evaluated PD participants’ motor severity, including neck rigidity, with the MDS-UPDRS Part 3 (i.e. motor sub-section) [18] and with the Hoehn and Yahr Scale; and calculated levodopa equivalent daily dose (LEDD) [19]. Participants in the PD group were grouped into tremor dominant (TD) or postural instability/gait disorder (PIGD) phenotypes based on Part 3 of the MDS-UPDRS. Participants were classified as indeterminate (IND) if phenotyping was ambiguous [20].
Lightweight ICS Impulse video goggles and software (GN Otometrics, Taastrup, Denmark) which recorded motion of the right eye with a camera speed of 250 frames/s were used to complete vHIT for all six semicircular canals (SCCs, i.e., the left and right LC and VC plane pairs consisting of left anterior and right posterior (LARP), and right anterior and left posterior canals (RALP)). Subjects were tested sitting upright with feet on the floor at 1 m distance away from a fixed standardised visual target at eye level in a well-lit room (to ensure a small pupil). vHIT goggles were tightened and a specific goggle insert was used, if required, for participants with non-prominent nose bridges to ensure minimal goggle slip. Eye position signal was calibrated by the subject fixating on two successive projected laser spots. Once successfully calibrated, oculomotor screening was completed to check for spontaneous nystagmus, gaze-evoked nystagmus, skew deviation, saccades, VOR suppression and visual VOR; these findings are not reported in this study. Comfortable neck range of motion was tested with slow (about 0.3Hz) sinusoidal rotational motion of the head in the plane of the canals being tested. Impulsive head displacements ranged between 5°–20°. The range of motion of the impulse was reduced if there were complaints of any discomfort. LC impulsive tests were performed with both hands on the top of the head, VC tests were performed with one hand under the chin and the other on top of the head, well away from the goggle strap and skin of the forehead, to avoid goggle movement artefact [12]. For LARP and RALP testing, the participant was rotated en bloc 40° in the chair to the right or left, respectively, with gaze remaining on the central target. Participants were asked to fixate on the target while the researcher applied small brief unpredictable (in direction and magnitude) head rotations in the canal plane being tested at velocities between 100°–300° per second with minimal ‘bounce back’ at the end of the impulse.
Traces of the eye and head velocity were displayed simultaneously on the computer monitor during testing, and a video recording of the procedure was taken. Twenty impulses were completed in each rotational direction. After testing, each individual head and eye velocity trace was checked for artefacts and unacceptable impulses were discarded. De-identified data sets were analysed by authors IC and KH, who were blinded to the grouping code. Data sets with unacceptable trace noise, out-of-plane eye movement artefact affecting the VCs, blinks or eyelid intrusions were excluded, on consensus, from the analysis. De-identified vHIT mean gain values, defined as the area under the desaccaded eye velocity curve from the start to the end of the head impulse, divided by the area under the head velocity curve over the same time interval, were recorded from acceptable data sets for all six SCCs. A vHIT was considered abnormal if VOR gains were outside the ICS Impulse software-defined age and velocity normal range and either overt or covert corrective saccades were present. Saccades were classified as covert if they occurred during the head movement or overt if occurring after cessation of head motion. One PD participant was excluded from the vHIT assessment due to congenital nystagmus impacting on vHIT system calibration. Thumbnails of raw vHIT data traces are included as
Statistical analyses
This study’s data was collected as part of a larger study investigating balance and vestibular function in PwPD. Based on the vHIT findings from Lv et al. [13], a post-hoc power calculation revealed that with α= 0.05 and β= 0.2; with LC VOR gain hypothesised means of 1.0 (SD 0.2) in HC and 1.2 (SD 0.2) in PwPD, a minimum sample size of 16 participants per group would be adequate to detect any significant between-group differences in LC VOR gains.
All data were analysed using SPSS Version 24 (IBM Corp, Armonk NY). Independent samples t-tests were used to compare demographics and VOR gain means between PD and HC. Fisher’s Exact test was used to compare the proportion of ‘normal’ vs ‘abnormal’ vHIT responses and to test for the relationship with falls between groups. Tukey’s ANOVA was used to compare PD phenotypes with HC. Logistic regression was used to assess relationships between VOR gains and PD duration, age, LEDD and PD severity as measured by MDS-UPDRS-Part 3 and past falls.
Results
PD and HC groups were well matched on demographics, with no statistically significant between-group differences for age, gender or cognitive status (p > 0.05, Table 1). PD participants had mostly mild to moderate disease (78%were in a Hoehn and Yahr stage of 1 or 2). They reported significantly higher fear of falling (p < 0.001) and had a greater incidence of previous falls than HC, including the presence of recurrent falls (i.e.≥2 falls). Twenty-one PD participants (53%) were phenotyped as TD, 17 (43%) as PIGD and two (5%) were classified as indeterminate (IND).
Participant Demographics. Data are reported as mean (SD) or number (%)
Participant Demographics. Data are reported as mean (SD) or number (%)
1Mini Mental State examination. 2Falls Efficacy Scale-International. 3Levodopa Equivalent Daily Dose (mg). 4lower score indicates less severe disease. 5TD = Tremor Dominant; PIGD = Postural Instability/Gait Dysfunction; IND = Indeterminate.
Results of vHIT showed no significant differences in LC and VC VOR gains between the entire PD group, or PD phenotypes, compared to HC, including when data sets of ‘abnormal’ VOR gains with corrective saccades were excluded (p > 0.05, Table 2). No PD participants recorded VOR gains > 1.2 in either LC or VC. Typical vHIT examples are given in Figs. 1A, B and C. Right LC gains were systematically higher compared to left LC gains in both groups, an expected finding [23], due to the right sided camera. More than half of the left anterior and right posterior canal data sets had unacceptable measurement artefacts resulting in exclusion from analysis (Table 2, Figs. 1E and F).
vHIT canal mean gains for the SCC for both PD and HC groups (ANOVA)
HC- healthy control, TD- tremor dominant PD sub-type; PIGD - postural instability/gait dysfunction PD sub-type; IND- indeterminate PD sub-type. Tindependent samples t-test HC vs PD all. Some data sets excluded due to artefact. ∧ANOVA PD phenotype compared to HC.
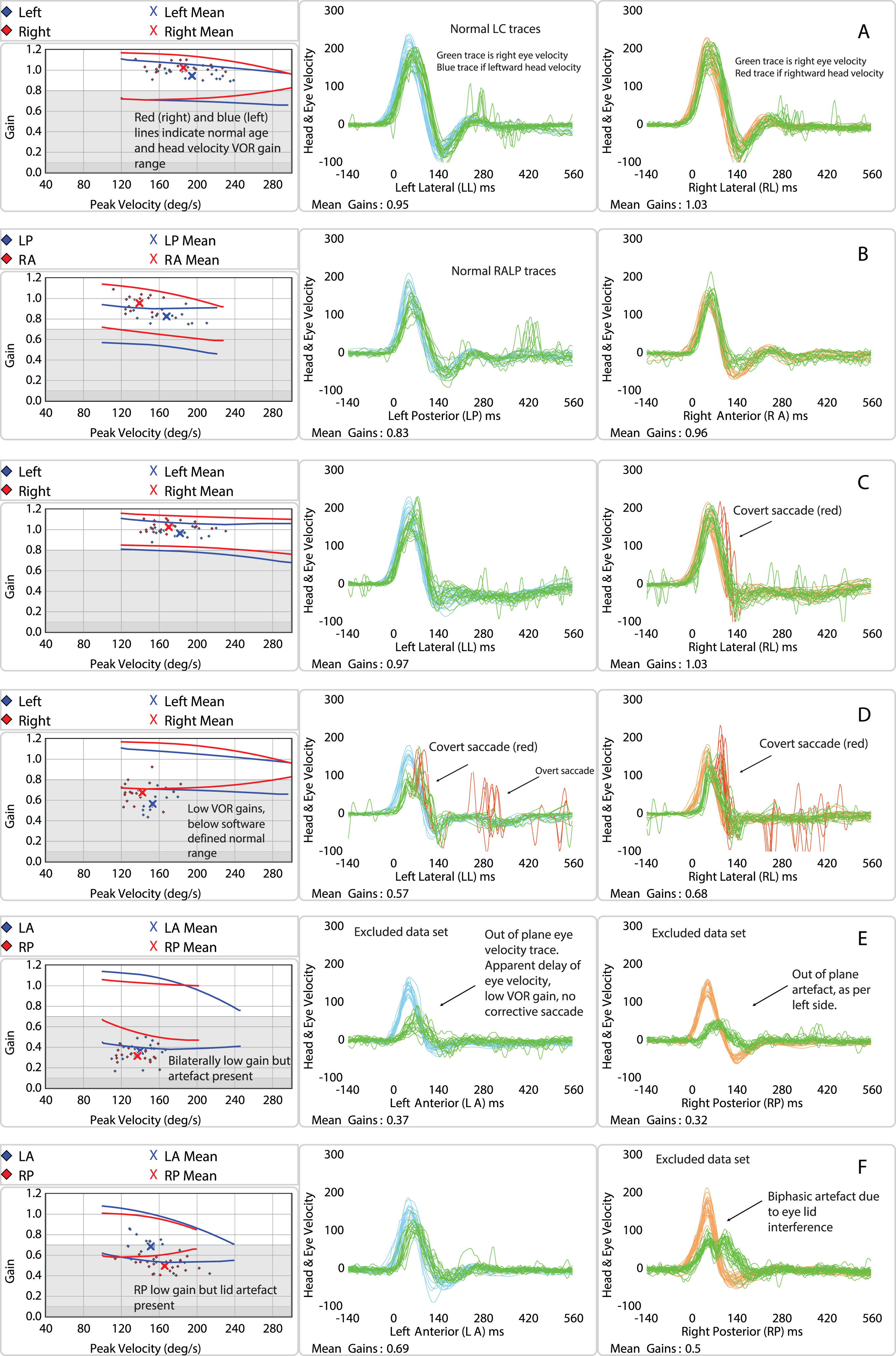
vHIT data trace examples. vHIT responses for a (A) control with normal lateral canal VOR gain; (B) control with normal right anterior left posterior canal responses; (C) PD with small covert saccade on right sided LC testing; (D) PD with bilateral hypofunction; (E) excluded left anterior right posterior data set due to out of plane eye movement; (F) excluded right posterior data set due to lower lid artefact. Age and velocity dependent normal ranges indicated by line markers on gain plots (grey and white plot on left).
Age, disease duration, LEDD and MDS-UPDRS Part 3 were not significantly associated with VOR gains in PD participants for any of the six SCCs. There were no significant differences between the PD group or PD phenotypes and HC in terms of ‘abnormal’ vs ‘normal’ VOR gains for any of the six SCCs (p = 0.35). There was also no significant relationship between abnormal vHIT and the reported number of falls in either group (p = 0.34). In the PD group, 7 participants (18%) recorded abnormally low LC vHIT gains with corrective saccades present (these participants recorded LC VOR gains between 0.50 –0.75). Secondary analysis of these data sets’oculomotor screening (spontaneous or gaze-evoked nystagmus) did not indicate uncompensated vestibular asymmetry.Two participants had bilaterally low LC VOR gains with corrective saccades, and both were phenotyped as TD with high disease severity (Hoehn and Yahr stage 3, MDS-UPDRS Part 3 scores > 52) (Fig. 1D). In the HC group, 4 (10%) participants recorded below normal VOR LC gains with corrective saccades (these participants recorded LC VOR gains between 0.63 –0.78). One had mild bilateral vestibular hypofunction. None of the participants in either group with abnormal vHIT findings reported any prior memorable acute vestibular event or specific vertigo episodes.
This study has shown that impulsive angular VOR, mediated by the lateral and vertical SCCs and measured by vHIT VOR gain values, is not significantly different between people with mild to moderate PD, or between PD phenotypes, and age-matched HC. Our findings are consistent with those of Scarpa et al. [14] and contrast those of Lv et al. [13].
The differences between our findings and the study of Lv et al. [13] may be due to many factors. A review article on the practical aspects and pitfalls of vHIT [12] reports that high VOR gains can commonly be the result of goggle slippage or the vHIT target being too close (< 1m) to the subject, though these factors were reportedly addressed by Lv et al. [13]. Mantokoudis et al. [24] described common vHIT artefacts in their study and noted that high VOR gains were most often due to incorrect vHIT system calibration. They reported consistently reproducing high gains (>1.2) in normal subjects under laboratory conditions by performing repeated vHIT after inaccurate system calibration. They also suggested calibration errors may occur if a subject is inattentive, drowsy or does not accurately focus on the target during the pupil recognition calibration process. It is possible that uncontrolled neck/head tremor in TD PD may aggravate a calibration error such as this. Another possible explanation for the high LC VOR gains reported by Lv et al. [13] is the inadequacy of head stimulus velocities and the possibility of participants predicting head rotation direction [25], thus artificially increasing VOR gains [12].
Neck rigidity and forward head posture are common in people with PD [26] and can add a practical difficulty to vHIT testing. To minimise the effect of PD related rigidity on our testing protocol, we tested PD participants during their ON medication phase. Neck rigidity was assessed in the yaw plane (i.e. item 3.3 of the MDS-UPDRS) before commencing vHIT testing. No PD participants recorded severe neck rigidity, and only 2/40 recorded moderate rigidity: both achieved acceptable head impulse velocities and recorded LC VOR gains within the software-defined age and head velocity normal range. Thus, mild-moderate neck rigidity, at least when testing the LC VOR gains at low amplitudes of head motion, appears not to impact vHIT test findings, despite the practical difficulty for the tester. In the VC planes, low velocity and amplitude sinusoidal passive motion were performed before vHIT to check for patient comfort and calibration of the vHIT system; however, rigidity in these planes was not explicitly assessed; future studies should address this.
The geometrical implications of the forward head position commonly reported in PD and occasionally occurring with thoracic kyphosis with increased age in HC may confound the measurement of VOR gains with vHIT, particularly with VC testing. The VOR gain is measured as the area under the desaccaded eye velocity curve divided by the area under the head velocity curve. A pure VC impulsive stimulus is challenging to deliver passively. For example, if the head impulse stimulus had a small additional translational or torsional component due to the participant’s abnormal body posture or mechanical resistance, the resultant head velocity detected by the plane-specific goggle sensors would be reduced, and the resultant VOR gain would be artificially increased, though this effect is likely to be small [12]. A limitation of our study was that, although forward head posture was noted, an objective measurement, such as the distance from the tragus to the line of the chair’s upright [27] was not explicitly measured.Future studies in PD should aim to address this issue. Alternatively, search coils are the gold standard assessment tool for impulsive VOR and can measure torsional eye velocities [28], however, these are time-consuming, non-portable and semi-invasive.
As in other studies, vHIT trace artefacts were common in both the PD and HC groups (see [12] and [24] for a description of artefacts), particularly in the LARP planes, and resulted in the exclusion of multiple vHIT data sets from the analysis. During VC testing, the most common trace artefact was ‘out of plane’ eye position, seen on the vHIT trace as low VOR gain with an apparent delay of eye motion without covert or overt corrective saccades (Fig. 1E). These trace artefacts result from the vHIT system only being able to track horizontal and vertical eye velocities but not torsion. If the gaze is out of plane, the resulting torsional component of the eye movement in response to the head impulse is lost to measurement, thus producing the typical artefact described above. During LARP testing, some subjects in both groups reported difficulty maintaining gaze angle or seeing the target clearly during testing; this was exacerbated in subjects with ‘droopy’ eyelids.
The suspected reason for increased difficulty with the maintenance of gaze fixation specific to the LARP plane relates to the subject rotating their body en bloc 30–40° to the right to the software-defined ‘correct’ head position. This effectively moves the right (i.e., recording) eye further from and lateral to the central gaze fixation target; the recording eye is in eccentric medial gaze, with the pupil next to the ocular canthus. The eccentric medial eye position is further exaggerated if the participant has a forward head position, as their head moves around in an arc as they rotate right en bloc (see supplementary diagram). For RALP testing, the subject’s recording eye is in a less eccentric lateral position and gaze fixation is therefore easier, hence less out of plane artefact.To avoid this in future, after rotating en bloc to the software-defined position, the clinician should ask the subject to shift their body laterally on the chair to realign their gaze with the central target, to avoid extremes of eccentric gaze, especially in the LARP plane. Additionally, PwPD are known to have impaired contrast sensitivity [29], and the use of a LED lightbox as the background for the fixation target may help keep the gaze in the correct position for VC testing.
The second most common artefact was upper or lower eyelid interference, producing an apparent biphasic or uniphasic eye response or ‘table-top’ eye velocity curve (see Fig. 1F), again preferentially affecting the LARP plane. This was likely due to the close proximity of the pupil to the canthus and closer proximity of the top and bottom eyelids. Some subjects did not tolerate ‘tucking’ of eyelids as a method of avoiding this. Persistent blinking also produced unacceptable data traces.
PD severity may also impact vHIT findings in this group. Neuropathological studies have shown PD associated neurodegenerative changes affecting the vestibular nuclei predominantly responsible for LC and VC VOR reflex responses, the medial and superior vestibular nuclei, respectively [3]. An explanation for the disparity between this and our findings of a lack of significant vHIT gain difference is that the participants in this study had mild to moderate PD while neuropathological studies are made post-mortem, suggesting possibly more significant neurodegeneration and disease burden in the latter. vHIT VOR changes may occur later in the disease process, as suggested by the two more severely affected PD participants with bilateral vestibular hypofunction in our study. Future studies in PD should aim to compare vHIT VOR gains across a range of disease severities.
The small number of studies investigating the effects of vestibular rehabilitation on PD have reported significant improvements in gait and functional performance as well as subjective complaints of dizziness [30, 31]. Based on our findings,vestibular rehabilitation programmes for PwPD should focus on sensori-integration, balance and gait training including head motion, though no specific emphasis need be placed on gaze stability training per se, at least in the early to mid-disease stages of PD.The essentially normal impulsive vHIT-recorded VOR function in early to mid-stage PD indicates that the increased falls prevalence seen in this group, compared to controls, does not arise from dysfunction of SCC-mediated reflexes.
Conclusion
In this study, there were no statistically significant differences in VOR gain as measured by vHIT in any of the six SCCs between subjects with mild to moderate PD or PD phenotypes and age and gender-matched HC. This implies that the impulsive angular VOR pathways remain largely unaffected by the neurodegenerative changes associated with early to moderate stage PD.
Declarations of interest
Nil.
CRediT author statement
KH: conceptualisation, original draft and writing review, investigation, data curation, methodology, formal analysis.
EC: conceptualisation, investigation, writing re-view and editing, supervision.
SP: conceptualisation, formal analysis, writing re-view and editing, supervision.
AB: software, writing review and editing.
HGM: resources, writing, editing.
IC: conceptualisation, writing review and editing, supervision.