
Abstract
AIM:
To comprehensively evaluate the dynamic change of vestibular function during long-term follow-up of vestibular neuritis, as well as the co-relationship with the outcomes of vestibular neuritis (VN), which provides the recommendations for vestibular function tests during the course of VN.
METHODS:
A prospective cohort study was conducted on 16 patients with acute VN. Caloric test, vHIT, rotatory chair tests, VEMP, dizziness handicap inventory (DHI) score, and dynamic dizzy scales (VAS-DD) was first performed within 7 days of neuritis onset, which were further re-evaluated during the 6–12 months of follow-up. The dynamic changes on multiple objective vestibular examinations were analyzed during the acute and recovery stage of VN. We further evaluated the co-relationship between the vestibular dysfunction scales and the prognosis of VN.
RESULTS:
In more than 6 months of follow-up, 44% of the ultralow frequency, 94% of the low-to-mid frequency, and 44% of the high-frequency function of the horizontal semicircular canal returned to normal (p < 0.05). The change degree in symmetry of the rotatory chair test was correlated with the gain of the horizontal semicircular canal on the vHIT and the unilateral weakness (UW) value on the caloric test (p < 0.05). The change in DHI score was correlated with the phase; change in VAS-DD level correlated with the symmetry and TC of the rotatory chair test at VN recovery stage (p < 0.05). There was no significant correlation between the change in DHI score or change in VAS-DD and the degree of vestibular function recovery (p > 0.05).
CONCLUSION:
In general, vestibular function improved during the course of VN. The rotatory chair test can be used to evaluate the overall function of the vestibular system and the compensatory state in patients with VN.
Introduction
Vestibular neuritis (VN), also called Acute Unilateral Vestibulopathy (AUVP), is a common type of acute peripheral vestibular syndrome in clinical practice, with obvious sustained rotatory vertigo, instability, nausea, vomiting, and horizontal spontaneous nystagmus [1]. It is not associated with cochlear or central nervous system symptoms. Vestibular neuritis can be divided into superior VN, inferior VN and total VN. In clinical practice, superior VN is more common, total VN takes second place, and isolated inferior VN is rare [2, 3].
The caloric test was used early in evaluating horizontal semicircular canal function and was once considered the gold standard for diagnosing VN [4]. The vestibular function testing of cervical and ocular vestibular evoked myogenic potential (VEMP), and video head impulse test (vHIT) can be used to evaluate selective impairment of the vestibular nerves for making a diagnosis of VN [5]. The vHIT can even help to provide a more accurate diagnosis of the rare subtype of inferior VN [6]. VEMP abnormalities improve more significantly than canal-related test abnormalities after 12 months follow-up in VN [7]. However, VEMPs failed to predict the development of chronic vestibular dysfunction [8]. The vestibular semicircular canal system has frequency characteristics, which are associated with the viscosity of the endolymphatic fluid in the semicircular canal, the frictional resistance of the membranous semicircular canal wall, and the elasticity of the gelatinous roof [9]. The consistency among multiple functional tests of the vestibular system has not been evaluated during the course of VN.
The caloric test is mainly used to evaluate the function of the horizontal semicircular canal. Unilateral weakness (UW) and directional preponderance values (DP) are common parameters to evaluate vestibular function, at frequencies less than 0.003 Hz. The vHIT can be used to assess the function of six semicircular canals. Gain-reductions and pathological saccades are considered abnormal, which represents vestibular function at frequencies of 2–5 Hz. VEMPs are designed to evaluate otolith organ function as well as the related neural circuits. According to the distribution of the vestibular nerve, cVEMP is used to evaluate the function of the sacculus and inferior vestibular nerve. oVEMP is used to evaluate the function of the utriculus, and superior vestibular nerve. The rotatory chair test can be used to evaluate central compensatory function at various frequencies. Gain, symmetry, phase shift, and time constant (TC) are commonly used parameters to evaluate vestibular function at low-to-mid frequency [10–12].
The clinical outcome of VN has been mostly evaluated by the subjective symptomatic recovery and vertigo assessment scales. Impaired vision, dizziness, and postural imbalance during walking and rapid head movement are common chronic clinical symptoms. Several studies have reported that 20% to 53% of patients have incomplete recovery with continuous or episodic vertigo or unsteadiness. Some patients with VN improved spontaneously and returned to normal activity [13–15]. Regarding vestibular function, 42% of patients with VN had normalization of horizontal semicircular canal paresis, while more than 50% of the patients with VN still had canal paresis in long-term follow-ups for more than 5 years [14, 16]. The prognosis of VN was relatively large different and the key factors affecting the prognosis were not clear.
It is unknown whether the prognosis of VN is related to abnormalities at specific frequencies of the horizontal semicircular canal function or damage sites in peripheral vestibular organs. It is unknown which examination of vestibular function is more likely to reflect the recovery state of VN. In the current study, we addressed those questions by evaluating the improvement of peripheral vestibular function in patients with VN as well as the co-relationship with subjective symptom scales during long-term follow-ups.
According to previous studies, the clinical recovery of VN partly depends on the central process of vestibular compensation and partly on the improvement of peripheral vestibular function [17, 18]. Thus, understanding the characteristics of patients with VN is essential to guide rehabilitation strategies to achieve faster and more efficient recovery.
Materials and methods
This prospective study was conducted from December 2020 to June 2022. We recruited 16 patients with VN referred to the Vertigo and Vestibular Dysfunction Clinical Center in the Otorhinolaryngology Department at the Eye and ENT Hospital of Fudan University, China. 20 healthy volunteers (male/female = 11/9, age: 32.6±7.6 years) were a control group who matched gender and age distribution of the enrolled patients. The institutional Ethics Committee review board approved this study, and all the enrolled participants provided written informed consent.
The simplified Dizziness Handicap Inventory (DHIs) was used to measure the vestibular symptom severity of VN, including 10-item questionnaires to evaluate the physical, emotional, and functional impairment associated with dizziness. The answers to each question were always (4 scores), sometimes (2 scores) and none (0 scores). VAS-Balance (VAS-BA) and VAS-dynamic dizziness (VAS-DD) were used to measure degree of instability and emotional sensation, respectively. The scores range from 1 to 10, and 10 is the highest, meaning the most severe symptoms. DHIs scores <6 and VAS scores <3 were defined as subjective symptom recovery without vertigo and instability.
The enrolled participants were in line with the diagnostic criteria of Acute unilateral vestibulopathy/vestibular neuritis, which was defined by the Committee for the Classification of Vestibular Disorders of the Bárány Society [1], and the inclusion and exclusion criteria as follows: A) age of participants ranged from 20 years to 50 years; B)Acute or subacute onset of spontaneous vertigo lasting more than 24 hours with nausea/vomiting or unbalance; C) unidirectional horizontal-torsional nystagmus beating away the affected side; D) Unambiguous evidence of reduced unilateral VOR function; E) acute central neurological signs or symptoms were absent, with normal MRI/CT of the brain or without central ocular motor or central vestibular signs; F) no acute audiological or otological signs or symptoms, including no unilateral audiometry abnormality; G) no history of recurrent vertigo episodes, such as sudden deafness with vertigo, Meniere’s disease, acute bilateral vestibular function loss, vestibular diseases with fluctuating symptoms and vestibular migraine. H) Patients with a history of cardiovascular and cerebrovascular diseases, obesity, diabetes, and hypertension were excluded. Baseline information of all enrolled patients was collected within 7 days of neuritis onset, including gender, age, onset time, onset side, DHIs, VAS-BA, VAS-DD, nystagmus intensity, pure tone audiometry, vestibular function tests (caloric testing, vHIT, the rotatory chair test, and VEMPs) and past medical history. The vestibular function test and DHIs, VAS-BA, and VAS-DD were re-evaluated during 6–12 months follow-up.
The patients received vestibular rehabilitation as early as possible, and tried to start customized vestibular rehabilitation within 1 week. Patients had no blood pressure abnormalities, disturbance of level of consciousness, chest tightness, palpitation, dysarthria, extreme weakness or deviation of walking before receiving vestibular rehabilitation. Oral corticosteroids (prednisone) were administrated as 50 mg daily for 3 days for the patients with body weight above 60 kg, and decreased by 10 mg every two days; For the patients with body weight below 60 kg, prednisone was administrated as 40 mg daily for 3 days and decreased by 10 mg every two days. Oral valaciclovir was administrated as 300 mg twice daily for 7 days.
A GN Otometrics Type air irrigator (Otometrics, Taastrup, Denmark) was used to blow the constant hot/cold air to the left or right ears for 60 seconds, with a temperature of 49°C or 23°C. Cold air was delivered prior to the hot air to each ear, and the interval between the two operations was 5 minutes. GN Otometrics Type 1068 system (Otometrics, Taastrup, Denmark) was used to record the maximum slow-phase velocities of nystagmus by air irrigation and compute the canal paresis (UW) value based on the formula of Jongkees [19]. A canal paresis value more than 22% was considered an abnormal caloric test in our vestibular laboratory. A nystagmus response less than 12°/s bilaterally was considered bilateral canal paresis. A Directional preponderance value also was computed using the formula developed by Jongkees. A value of less than 27% was recorded as normal.
The Bio-Logic Navigator PRO (Natus) was used to conduct the VEMP examination in a soundproof chamber. The air conduction sound (ACS) consisted of 500 Hz short pure tone bursts with a rise/fall time was 2 ms and peak duration of 2 ms with a Bandpass filter 10∼1500 Hz, stacking 120 times. The ACS was transmitted to the subject’s ear via a calibrated earphone, starting with 125 dB SPL and then decreasing with 5 dB SPL step by step, with interelectrode resistance <5 Kω. In the oVEMP test, the reference electrode was located about 1 cm below the midpoint of the lower edge of orbits, the recording electrode was placed below 1 cm the reference electrode, and the ground electrode was placed in the midpoint of the lower edge of orbits on other side. When the subjects heard the sound coming from the headset, they were asked to look upward and hold up gaze at 30 degrees. In the cVEMP test, the reference electrode was located in the middle of the sternocleidomastoid muscle; the recording electrode was placed on the surface of the lower suprasternal fossa, and the ground electrode was placed in the middle of the sternocleidomastoid muscle on other side. When the subjects heard the sound from the earphones, they were asked to raise their heads so that the sternocleidomastoid muscles were contracted and in a constant state of tension, keeping their heads at the midline of their body.
A vHIT system (ZT-VNG-1 system, Shanghai ZEHNIT Medical Technology Co., Ltd., Shanghai, China) was used to measure VOR function with high angular accelerations (above 2000 degrees/s2). All vHITs tests were performed by the same clinician. The patient was seated and wore a test eye mask. Eyes were fixed on a visual target 1.5 m away. The direction of head rotations were random. The rapid, random, and mini-amplitude head pulse movements were performed at a speed of 150–200 degrees/s in the horizontal direction and 100–150 degrees/s in the vertical direction, with a head-movement amplitude of 30–45 degrees in each plane. Each plane was tested 15–20 times, and the computer automatically calculated the average gain and the presence of saccades (including covert saccades and overt saccades). Gains equaled the ratio of eye velocity to head velocity for responses to impulses. The normal reference values of vHIT gain in our laboratory are 0.8–1.2 for horizontal semicircular canals and more than 0.7 for vertical semicircular canals.
The rotatory chair test was performed on VertiChair (ZT-CHAIR-I, Shanghai ZEHNIT Medical Technology Co., Ltd., Shanghai, China) with VertiPACS. VertiGoggles (ZT-VNG-II, Shanghai ZEHNIT Medical Technology Co., Ltd., Shanghai, China) were used to record the maximum slow angular velocity of nystagmus. The sinusoidal harmonic acceleration test was measured at 0.01 Hz to 0.64 Hz with a full rotation speed of 50 degrees/s and a maximum acceleration of 3.1–201 degrees/s2. The chair rotated about an earth-vertical axis. A rotational step test was performed to record vestibular function at frequencies of 0.5 Hz, and the test was performed with a maximum rotation speed of 90 degrees/s and a maximum rotation acceleration of 3 degrees/s2. Parameters for the rotatory chair test include gain, phase shift, symmetry, and time constant. The gain represents the ratio of eye speed to head speed. The phase represents the coordination between eye and head movement, equivalent to reflex latency. Symmetry corresponds to the difference between left and right eye movements. The gain, phase shift, and symmetry of the rotatory chair test were abnormal if the average of three consecutive frequencies was higher or lower than the corresponding frequencies in the control group. The result of TC in the VN group was higher or lower than the normal reference value (mean±SD) of control group was regarded as abnormal.
SPSS 22.0 was used for the statistical analysis of the data. The description of continuous variables was expressed by mean±standard deviation/error, and the categorical variables were described by rate. The difference analysis of continuous variables was performed by t-test, paired t-test for UW and DP of caloric test, gain of vHIT, and scores of DHI, VAS-DD, VAS-BA. The gain, phase, symmetry and TC of rotatory chair test difference were analyzed by ANOVA; The categorical data analysis was performed by Chi-square test and Fishers exact test for abnormal rate of vestibular function test. Pearson correlation analysis was used for assessing the correlation of two continuous variables for scores reduction of DHI, VAS-DD, VAS-BA and vestibular function parameters changed level, and multiple linear regression was used for multivariate continuous variables about symmetry, UW, DP, TC changed degree and other vestibular function parameters at recovery stage. The difference and correlation were considered statistically significant if the level p < 0.05.
Results
In the cohort study, 21 patients meeting the diagnostic criteria were included. In the final, 16 patients with VN completing regular follow-up and receiving vestibular function re-evaluation were enrolled. The enrolled patients with VN were aged from 22 to 45 years. The percentage of VN that affect superior nerve were 100%. The percentage of VN complete lesions of superior nerve and inferior nerve were 31%. The demographic information of the VN patients is shown in Table 1.
The demographic information of the VN patients at onset stage
The demographic information of the VN patients at onset stage
The incidence of horizontal semicircular canal injury at ultralow frequency levels was 93.8% at the early onset stage, UW of the caloric test at the onset stage was 67.8% ±8.1%, and DP was 84.6% ±7.1%. After 6 months of recovery, the ultralow frequency horizontal semicircular canal function was recovered (p < 0.05), UW of 43.8% of VN patients returned to normal, and the percent of DP was significantly reduced (p < 0.05). (Table 2).
Caloric test UW and DP percent and normal rate at VN onset stage and 6–12 months after VN recovery stage
The abnormal symmetry of the rotatory chair test with low-mid-frequency was 100%, the abnormal phase shift was 62.5%, and the abnormal gain was 83.8% at the onset stage of VN (Table 3). Symmetry was significantly shifted compared to the control group (p < 0.05). The left vestibular neuritis was shifted to the left, and the right vestibular neuritis was shifted to the right. The symmetry of 93.8% of VN patients returned to the normal range after 6–12 months of recovery, and the symmetry was not significantly different between the control group and the VN group (p > 0.05) (Fig. 1.1).

shows symmetry of all enrolled patients at VN onset stage. The symmetry of left VN shifted to left side and the symmetry of right VN shifted to right side.
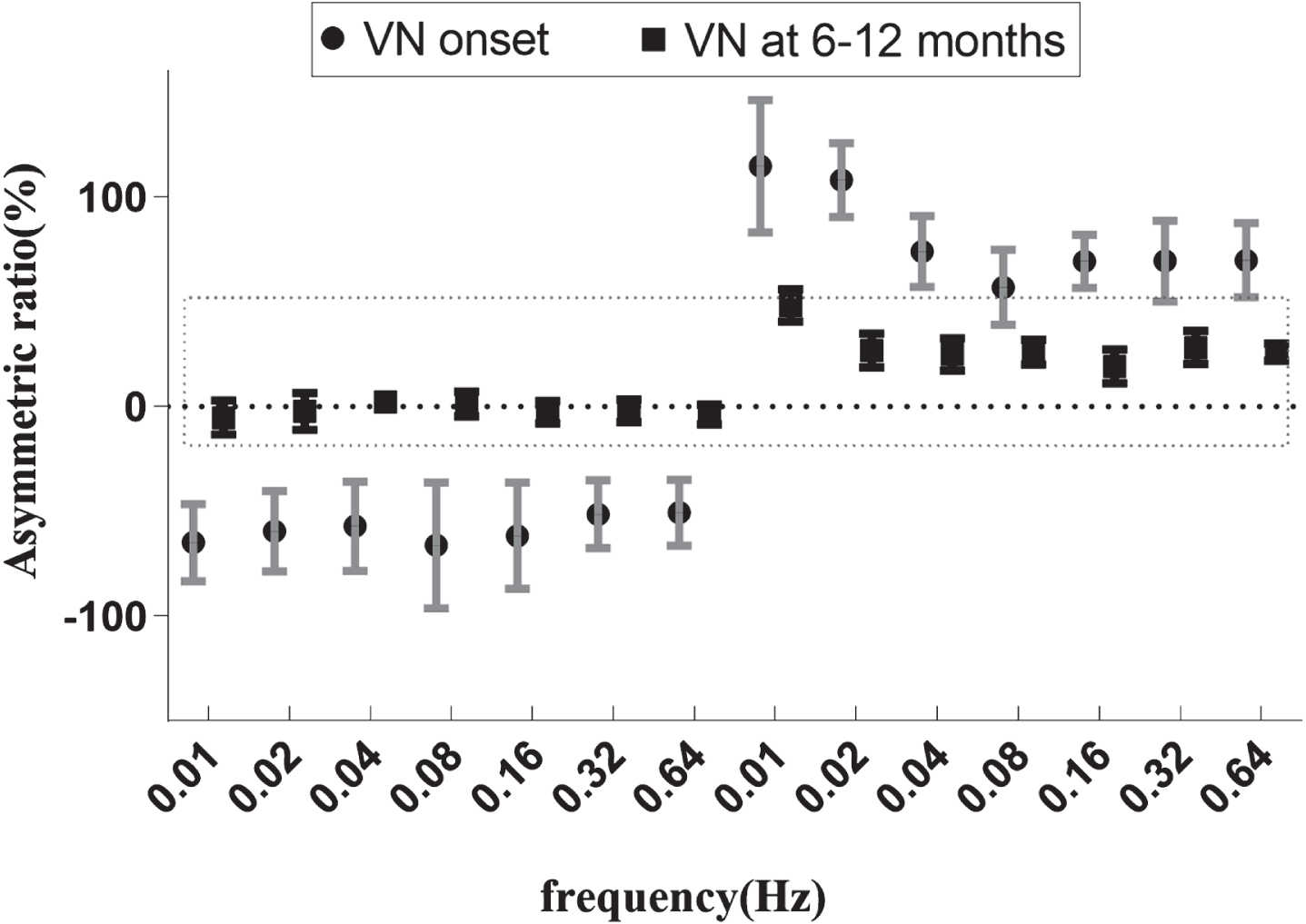
shows the change of symmetry of all enrolled patients at 6–12 months after VN recovery stage. The left VN group was under the horizontal axis at VN onset, which located on the X-axis first from 0.01 to 0.64 Hz, then returned to the normal range after 6–12 months follow-up shown by the dashed boxes. The right VN group was above the horizontal axis at VN onset, which is located on the X-axis second from 0.01 to 0.64 Hz, Symmetry returned to the normal range after 6–12 months follow-up shown by the dashed boxes.
Rotatory chair test normal rate at VN onset stage and 6–12 months after VN recovery stage
The gain level of each frequency of 0.01–0.64 Hz both at the VN onset and 6–12 months after VN recovery stage was less comparing with the control group (p < 0.05). However, the gain of the VN was not significant different between onset and 6–12 months after VN recovery stage (p > 0.05). The phase shift level of 0.04 Hz, 0.08 Hz and 0.32 Hz was different among VN onset stage, 6–12 months after VN recovery stage and the control group (p < 0.05), and the phase of the VN was not significantly different between VN onset and 6–12 months after VN recovery stage (p > 0.05), and there was no difference on the phase shifts of 0.32 Hz between control group and 6–12 months after VN recovery stage (p > 0.05) (Table 4).
The gain and phase of rotatory chair test in VN and control group at VN onset stage and 6–12 months after VN recovery stage
The TC of the affected side of VN was 3.4±1.5 s at VN onset stage, 9.9±1.6 s at 6–12 months after VN recovery stage, 9.6±1.7 s in the control group, and the TC of the unaffected side was 9.0±1.8 s at VN onset stage, 8.5±1.4 s at 6–12 months after VN recovery stage. The TC of the unaffected side showed no significant difference at VN onset stage, 6–12 months after VN recovery stage, and the control group (p > 0.05). The TC of the affected side was significantly shorter at VN onset stage than 6–12 months after VN recovery stage and control group (p < 0.05) (Fig. 2).
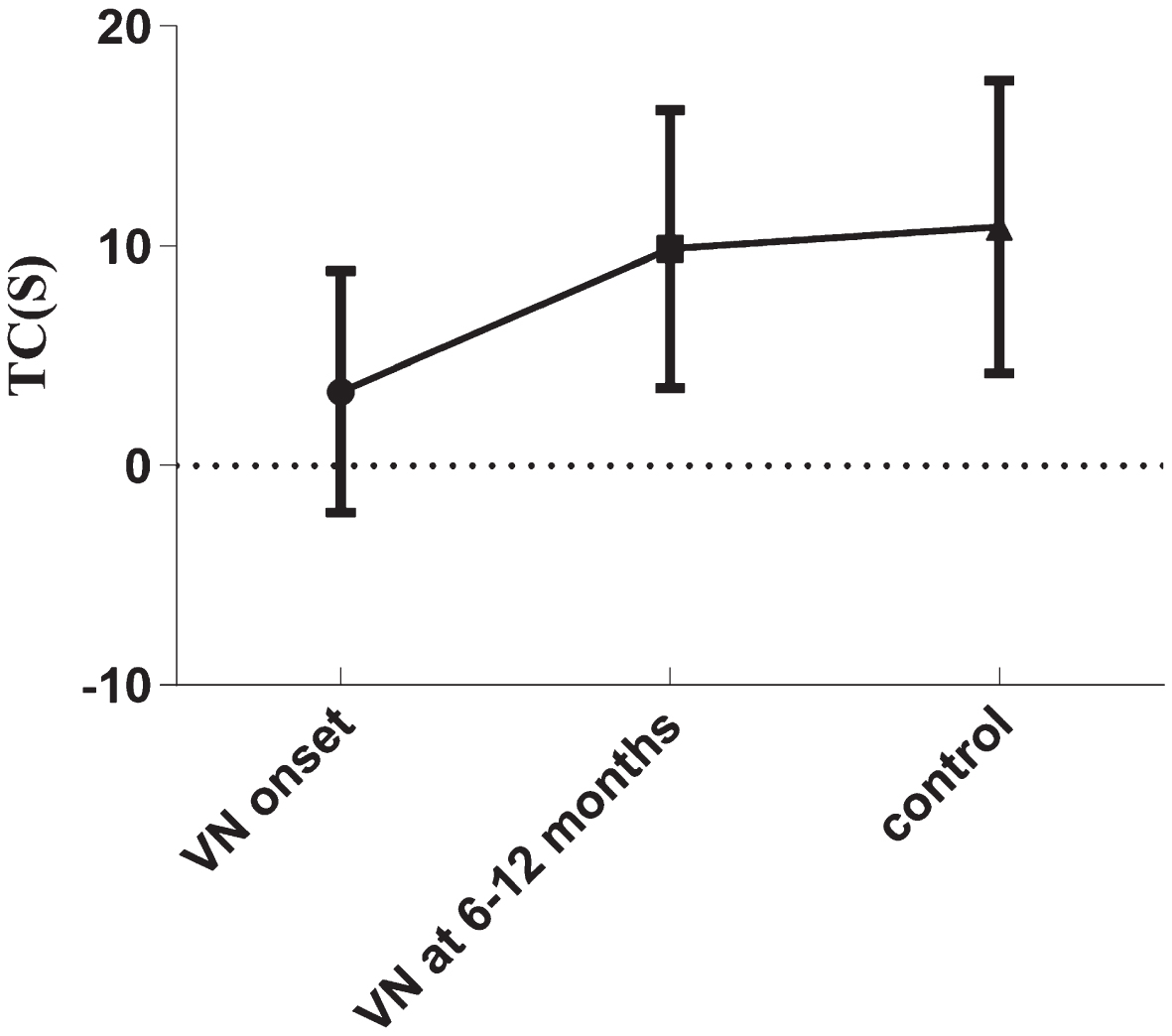
The VN onset data show the TC for the affected side of all enrolled patients (mean±SD) at the onset stage, VN at 6–12 months shows the affected side of all enrolled patients’ Tc results (mean ± SD) at recovery stage; control shows the left side Tc results (mean±SD), the Tc of onset group was significantly shorter than the 6–12 months recovery stage and control group (p < 0.05).
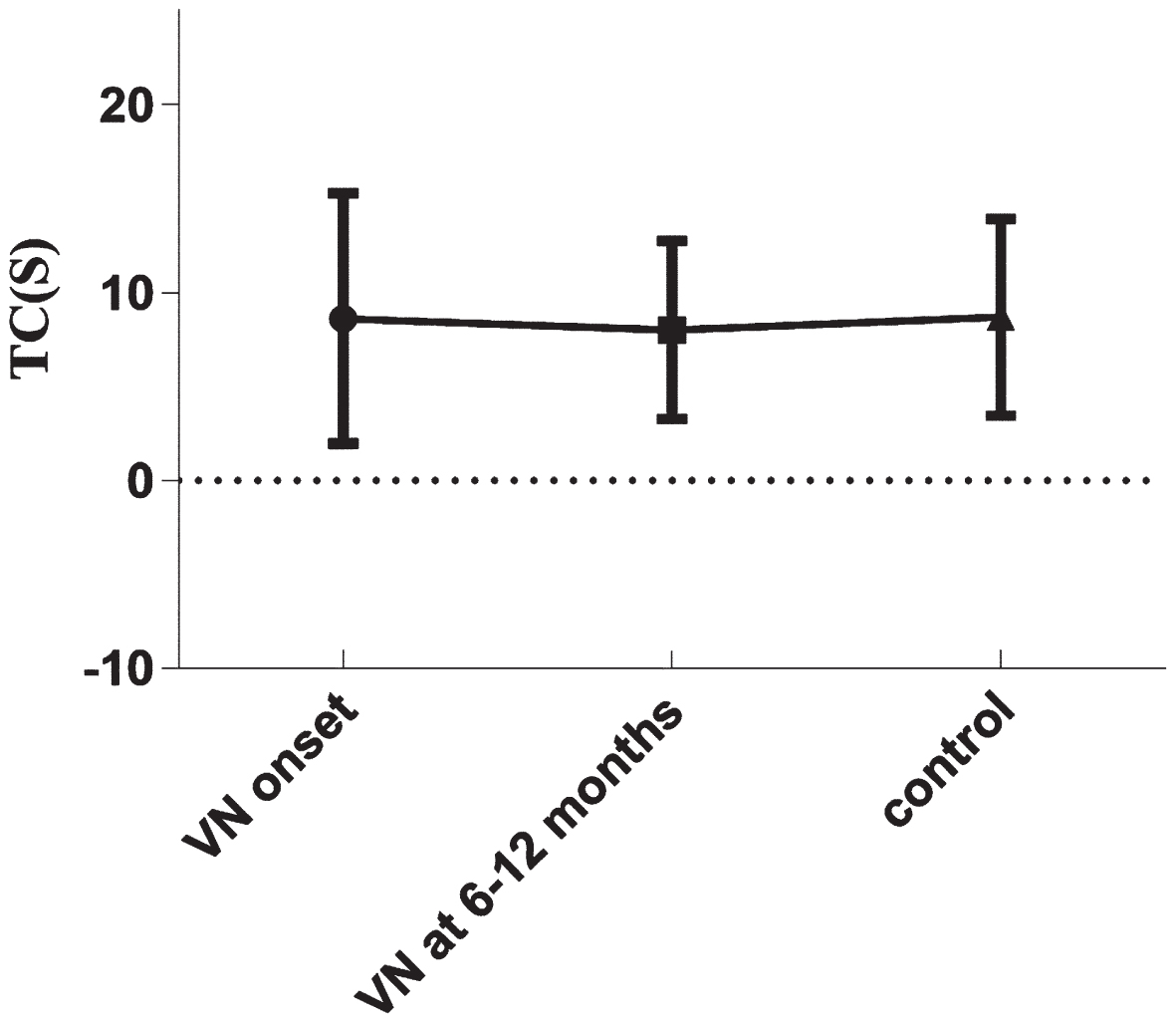
The VN onset data show Tc results (mean±SD) the unaffected side of all enrolled patients’ at the onset stage. VN at 6–12 months shows the unaffected side of all enrolled patients’ Tc results (mean ± SD) at recovery stage, control shows the right side Tc results (mean±SD); there were no significant differences among them (p > 0.05).
The incidence of horizontal semicircular canal function impairment at a high-frequency level of VN was 93.8%, and the abnormal incidence of anterior semicircular canal dysfunction and posterior semicircular canal dysfunction was 43.8% and 25%, respectively. After 6–12 months of follow-up, the abnormal incidence of horizontal and anterior semicircular canals was reduced compared with that at the VN onset (p < 0.05), and posterior semicircular canals returned to a normal level. Still, there was no statistical difference compared to initial evaluations (p > 0.05). The gain of the vertical semicircular canals reached the normal level, and the gain of the horizontal semicircular canals was still slightly lower than the normal level (p < 0.05). (Table 5) Still, the pathological saccade wave decreased or disappeared significantly. At 6–12 months of follow-up, saccades were completely absent in 37.5% (5/16) of the VN patients, 25% (4/16) of the VN patients had significant decreased amplitude of overt saccades, and 37.5% (5/16) of the VN patients just presented with covert saccades.
vHIT result at VN onset and 6–12 months after VN recovery stage in the affected side
At the onset of VN, the absent rate of oVEMP on the affected side was 31.3%, and the abnormal incidence was 93.8%. After 6–12 months of follow-up, the abnormal incidence and asymmetric ratio were not significantly improved (p > 0.05), and the present rate was higher than that at the onset of VN, but there was no statistical difference at onset and recovery stage of VN (p > 0.05). At VN onset stage, the absent rate of cVEMP was 18.8%, and the abnormal incidence was 37.5%. After 6–12 months follow-up, the abnormal incidence and asymmetry ratio had no significant improvement (p > 0.05) (Table 6).
VEMP results at VN onset and 6–12 months after VN recovery stage in the affected side
Note: AR means asymmetry ratio of amplitude.
After 6–12 months follow-up, one patient still had obvious positional vertigo, one patient still had a sense of right deviation when walking, and the other patients had no apparent complaints of vertigo and instability. DHI, VAS-BA, and VAS-DD were significantly reduced compared with the onset of VN (p < 0.05) (Fig. 3). The proportion of subjective symptoms completely recovered was 80%.
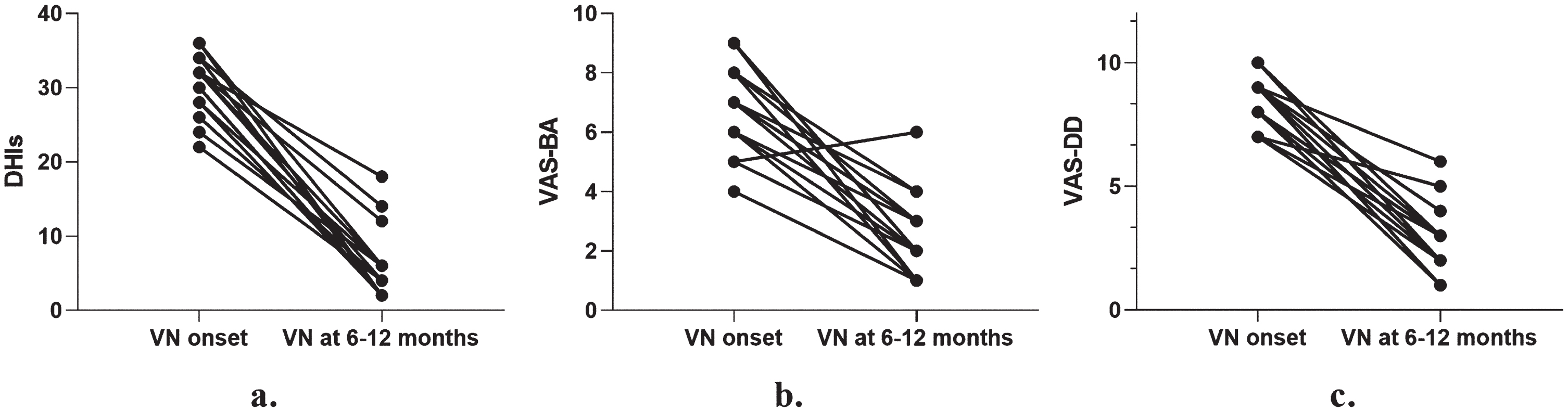
a. The scores of DHI was reduced at 6–12 months after recovery stage than that at VN onset (p < 0.05); b. The scores of VAS-BA was reduced at 6–12 months after recovery stage than that at VN onset (p < 0.05); c. The scores of VAS-DD was reduced at 6–12 months after recovery stage than that at VN onset (p < 0.05).
There was no significant correlation between DHIs, VAS-BA, VAS-DD scores reduction and the changed values of UW, DP, symmetry, TC and vHIT gain of horizontal semicircular canal affected side, as vestibular function recovery parameters at VN onset and after 6–12 months of follow-up by single-factor correlation analysis (p > 0.05). DHI change level was negatively correlated with the phase of the rotatory chair test (R2 = 0.554, p < 0.05), DD-VAS change level correlated with the symmetry and TC of the rotatory chair test at 6–12 months after VN recovery stage (R2 = 0.694, p < 0.05). The degree of symmetry change of the rotatory chair test was negatively correlated with the vHIT gain of the horizontal semicircular canal and UW value of the caloric test, and the degree of symmetry change was positively correlated with the TC on the unaffected side at 6–12 months after VN recovery stage (R2 = 0.773, p < 0.05). The change degree of DP was positively correlated with phase and TC on the affected side at 6–12-month VN recovery stage (R2 = 0.703, p < 0.05) (seen in supplementary material). However, the change degree of UW only was correlated with UW at 6–12 month VN recovery stage, and the change degree of horizontal semicircular canal vHIT gain only was correlated with vHIT gain at 6–12 month VN recovery stage (p < 0.05).
The pathogenesis of VN was unclear, and the management protocols of VN had not been normatively established. However, VN is generally associated with viral-mediated inflammation of the vestibular nerve, and valaciclovir has been reported to treat VN [20]. Corticosteroids can improve early symptoms and accelerate the recovery of VN [21]. Vestibular rehabilitation can alleviate vestibular symptoms and improve vestibular function in the medium and long-term follow-up [22, 23]. In order to achieve the best recovery effects with the homogenization intervention, the treatment strategies for VN in this study were composed of oral valaciclovir and corticosteroids, as well as vestibular rehabilitation. The age distribution of patients in this group ranged from 22 to 45 years old, excluding age’s influence on the prognosis of VN [24]. In this study, 80% of patients achieved satisfactory treatment results, with only one presenting with positional vertigo and one presenting with a sensation of leaning to the right when walking. The recovery efficacy is better than that reported in previous literature [3, 10], which may be associated with the optimized comprehensive treatment plan and younger aged patients enrolled in this study.
The caloric test was used to assess the ultralow frequency function of the peripheral vestibular system. It was regarded as the gold and early standard for diagnosing VN. At the same time, the caloric stimulus was not physiological due to the artificial current created by the differentiated densities of endolymphatic fluid in the horizontal semicircular canal after local heating or cooling with air or water, thereby causing an imbalance between the right and left vestibular-ocular reflexes. A previous study reported that 45% to 60% of canal paresis in VN could be returned to an average level after treatment [3, 25]. In this study, 93.8% of patients with horizontal semicircular canal dysfunction at the onset stage, and the value of UW and DP were 68% and 85%, respectively. UW returned to normal, meaning the horizontal semicircular canal function recovered. In this study, UW in 43% of patients reached normal during the recovery stage, which is in line with the previous report. DP can be considered an objective evaluation index of dynamic vestibular compensation, especially independently appearing without spontaneous and positional nystagmus [26, 27]. At the onset of VN, the abnormal rate of UW and DP was similar. However, the recovery of DP was significantly better than that of UW after 6 months of follow-up, and 80% of the patients had satisfactory clinical efficacy. The results indicated that the recovery of ultralow-frequency vestibular function also benefited from dynamic vestibular compensation.
The normal high-frequency vestibular function has an essential impact on the maintenance of daily activity, especially walking and rapid head movement. vHIT is a high-frequency measurement tool and a valuable complement to caloric tests. Even in several studies, vHIT was regarded as the current gold standard test of semicircular canal function, with 87.9% sensitivity and 94.8% specificity. Its positive and negative predictive values were 85.3% and 95.8%, respectively [4, 29]. The horizontal semicircular canal vHIT alone can identify superior nerve dysfunction of VN. However, both abnormal cervical vestibular evoked myogenic potentials and posterior semicircular canal vHIT to diagnose inferior vestibular nerve are necessary [2].
Reports differ as to which semicircular canal functions are more quickly restored. A literature report that the vertical canal had a better recovery, and the vertical canal VOR gains recovered more rapidly than the horizontal canal gains. However, little literature reports that the posterior canal’s function was not prone to recovery [28, 29]. In this study, the gain of anterior and posterior semicircular canals was significantly improved and almost returned to normal after 6–12 months of follow-up. The gain improvement degree of the horizontal semicircular canal was less than the vertical semicircular canal.
VEMP examination, as the primary means of evaluating otoliths and vestibular nerves, is of great help in diagnosing VN. In this study, the abnormal rate of the oVEMP test was 93.8%, and the cVEMP test was 37.5%, suggesting that superior vestibular nerve damage was more common. The previous study reported that the VN patients with otolith dysfunction had recovered entirely and VEMPs returned to normal levels after 6–12 months of follow-up [7, 30]. In this study, the vestibular nerve and otolith function did not improve significantly. However, the abnormality rate of cVEMPs were reduced compared to that at onset of disease after 6 months of follow-up, which was not statistically significant. The difference may be related to the impairment degree of vestibular nerve or otolith function, laboratory testing technology, and sample difference. However, we regarded that VEMP is essential to make a diagnosis and recognize the type of VN.
Lee et al. reported that the vestibular symptoms of inferior VN recovered quickly, the hospital duration and the follow-up period were shorter, and the symptom onset period was longer [6]. In this study, one had normal results in the caloric test, one in the oVEMP examination, and one in the horizontal semicircular canal vHIT. However, no patient was found to have only abnormal cVEMP or posterior semicircular canal vHIT. There is insufficient evidence to confirm the diagnosis of inferior VN. The low occurrence of inferior VN may be related to the anatomical structure. The inferior vestibular nerve runs shorter than the superior vestibular nerve, and the inferior vestibular nerve enters the bone canal with two branches. Therefore, the inferior vestibular nerve is not susceptible to virus infection [31]. We considered that a series of cross-validation of vestibular function tests is of great value for the localization and typing of VN. Inferior VN may not exist, and assessing vestibular dysfunction inadequately may cause a diagnosis of isolated inferior VN.
The overall outcome of VN is associated with various factors, including improvement in peripheral vestibular function, central vestibular compensatory, and adverse psychological and emotional states [32, 33], which combined effect determines the final overall prognosis of VN. At the same time, this may explain why there was no significant correlation between the overall subjective effect (DHI reduction) and vestibular function test in the prognosis of VN in this study. However, this study found that the improved symptoms of dynamic dizziness after recovery were inverse to the changed degree of symmetry in the rotatory chair test. The more symmetry changed after follow-up, the residual dizziness was less. The symmetry changed degree in the rotatory chair test may be reference indexes for indirect assessment of overall vestibular function in VN.
The function of the semicircular canal in multiple frequencies and otolith decreased by varying degrees in this study. The previous study reported that the damage to high-frequency horizontal semicircular canal function is permanent, and the low-frequency part of the peripheral vestibular system was easy to recover or become symmetrical [34]. In our study, we did not find the damage to high-frequency horizontal canal function more severe than low frequency, and 43.8% of the ultralow frequency and high-frequency horizontal semicircular canal function returned to a normal level and decreased by the same degree.
It has been reported that caloric tests and vHIT were used to diagnose VN. The rotatory chair test can be complementary to the caloric test when used to evaluate dizzy patients. Rotatory chair tests tend to be normal without adding diagnostic benefit when the caloric test is normal [35–37]. In our study, we found that the changed degree of symmetry of the rotatory chair test at disease onset and after 6 months of follow-up was negatively correlated with the vHIT gain of the horizontal canal and the UW of the caloric test after follow-up. This indicated that the rotatory chair test was consistent with the caloric test in the assessment of vestibular function recovery. However, the changed degree of symmetry was inverted correlated with the function recovery of high-frequency test in VN, which indicated that the vHIT evaluating vestibular function improvement was not a replacement during VN recovery, and the recovery step and degree of various frequencies of vestibular function may not keep the same trajectory in the VN prognosis. Jonathan et al. reported the main gain of vHIT recovery for the horizontal canal was present at the first months and decreased recovery efficiency from 3 months to 1 year [38].
According to Ewald’s second law, the semicircular canals on the conjugate plane remain synergistic. The rotatory chair test detecting bilateral vestibular dysfunction was superior to providing accurate side-specificity in unilateral vestibular dysfunction. However, the rotatory chair test was a physiologic stimulus and had varied precise frequency and amplitude. In this study, the gain of the rotatory chair test was not significantly different between the VN onset and recovery stage, which were both less than the control group. The gain was not a good indicator to predict the recovery effect, but it was helpful to make a diagnosis of VN. At the onset stage of VN, the symmetry of the rotatory chair test is of positive value to determine the affected side, which is the symmetry deviation consistent with the laterality of the VN. In practice, the sensitivity of rotatory chair test is higher in low-frequency stimulation, especially for the phase [39]. In this study, the phase of the rotatory chair test was earlier than the control group, especially in the range of the frequency 0.04 and 0.08 Hz. In this study, the overall subjective effect (DHI change level) of VN was negatively correlated with the phase of the rotatory chair test; dynamic dizzy improvement (VAS-DD) was correlated with the symmetry of rotatory chair test at 6–12 months after VN recovery stage; these results support the idea that the rotatory chair test can be used to assess the prognosis of VN on subject effect and symptoms recovery.
The time constant (TC) measures the time of nystagmus intensity reducing to 37% of its initial level. A previous study reported that TC would better diagnose peripheral and central vestibular. The TC of the affected side was shortest in patients with peripheral vestibular dysfunction, but both sides demonstrated lower than average duration [40, 41]. In this study, the TC of the affected side was significantly shorter than the unaffected side and control group, indicating that TC provides help in diagnosing VN. In the acute episode of vestibular neuritis, the velocity storage mechanism of the brainstem will be severely affected. With the recovery of vestibular function and vestibular compensation, the degree of velocity storage function recovery is related to dynamic dizziness, which indicated that the value of TC was a helpful factor to evaluate the prognosis of VN. In addition, the change degree of symmetry in the rotary chair test and DP in the caloric test were both positively correlated with the TC of the unaffected side at the follow-up stage, which shows the change of contralateral TC may also be a reference indicator of dynamic compensation.
Dynamic vestibular compensation processes also include adaptation, restoration, and habituation, which was a collaborative process between the vestibular balance system and other multi-sensory systems. DP of the caloric test, the gain of vHIT and the covert and overt saccades were used to evaluate the central vestibular compensation. The improvement in VOR gain of vHIT measures will evaluate central vestibular compensation to the temporary unilateral vestibular dysfunction occurrence [26, 42]. In this study, we found that the rotatory chair test can also be used to assess vestibular compensation and suggested that changes degree of symmetry and time constants of the affected and unaffected sides in the rotatory chair test at the VN recovery stage are recommended indicators.
A limitation of this study is the lack of dynamic subjective visual vertical testing and the sensory organization test to further evaluate utricular function and multi-sensory integration, for the case presenting with a sensation of leaning to the right when walking. Knowing the otolith function in the pitch plane and multi-sensory integration function is essential to making an appropriate treatment and vestibular rehabilitation plan. In a further study, more attention will be paid to the assessment of otolith function, dynamic subjective visual vertical and sensory organization testing, especially for patients with chronic unsteadiness.
Conclusion
Objective assessment of vestibular function cannot replace subjective symptom scale assessment in the prognosis of VN. Dynamic changes in vestibular function were present during VN. The changed degree of vestibulo-ocular symmetry can be used to evaluate indirectly the multiple frequencies of vestibular function and dizziness in VN. A rotatory chair test may be recommended for vestibular function assessment in VN prognosis.
Footnotes
Acknowledgments
This study was supported by the Shanghai Shen-kang Hospital Development Center (SHDC2022CRD006), and the Project of Shang-hai Municipal Science and Technology Commision (19441917100, 20S31907000).
Conflict of interest
No potential conflict of interest relevant to this article was reported.