
Abstract
BACKGROUND:
The management of dizziness and vertigo can be challenging in the emergency department (ED). It is important to rapidly diagnose vertebrobasilar stroke (VBS), as therapeutic options such as thrombolysis and anticoagulation require prompt decisions.
OBJECTIVE:
This study aims to assess the rate of misdiagnosis in patients with dizziness caused by VBS in the ED.
METHODS AND RESULTS:
The cohort was comprised of 66 patients with a mean age 56 years; 48% were women and 52% men. Among dizzy patients, 14% had VBS. We used Cohen’s kappa test to quantify the agreement between two raters –namely, emergency physicians and neurologists –regarding the causes of dizziness in the ED. The Kappa value was 0.27 regarding the final diagnosis of central vertigo disorders and VBS, thus showing the low agreement. We used the χi2 test to show the association between the presence of two or more cardiovascular risk factors and admission to the stroke unit (p = 0.015).
CONCLUSION:
There is a substantial rate of misdiagnosis in patients with dizziness caused by VBS in the ED. To reduce the number of missing diagnoses of VBS in the future, there is a need to train emergency physicians in neurovestibular examinations, including the HINTS examination for acute vestibular syndrome (AVS) and the Dix-Hallpike (DH) maneuver for episodic vestibular syndrome. Using video head impulse test could help reduce the rate of misdiagnosis of VBS in the ED.
Introduction
Dizziness and vertigo account for 3 to 4% of all emergency department (ED) visits [3–13]. Dizziness is defined by international experts as the sensation of disturbed spatial orientation without a false or distorted sense of motion and vertigo is defined as the sensation of self-motion when no self-motion is occurring or the sensation of distorted self-motion during an otherwise normal head movement [13].
Managing dizziness and vertigo in the ED can be challenging. It is estimated that up to 20% of VBS can manifest as isolated dizziness without any other neurological symptoms, which could partly explain the misdiagnosis of VBS in the ED [6]. At least half of patients change the description of their dizziness when asked to describe it again after 6 minutes [8]. This suggests that the diagnosis cannot be based on patient history alone. Indeed, Navi et al. reported that 22% of patients with dizziness or vertigo had no clear diagnosis after a complete vestibular assessment [7].
General medical etiologies (e.g., metabolic, toxic, cardiovascular) are the most common diagnoses, being given to 50% of patients presenting with dizziness at the ED [3]. Peripheral vestibular disorders such as vestibular neuritis (VN) and benign paroxysmal positional vertigo (BPPV) represent 33% of all vertigo visits. Neurological disorders are observed in 6 to 11% of cases, with vertebrobasilar stroke (VBS) being the most serious condition requiring acute treatment [3].
Edlow et al. recently described a new diagnostic approach based on the timing and triggering factors of dizziness [2]. Acute vestibular syndrome (AVS) is characterized by the sudden onset of vertigo or dizziness accompanied by nausea or vomiting, unsteady gait, head motion intolerance and spontaneous nystagmus lasting for days to weeks [13]. In this case, VBS and VN are the main diagnoses to consider. The HINTS examination (Head Impulse test, Nystagmus, Test of Skew) differentiates between these two clinical entities with better accuracy than brain magnetic resonance imaging (MRI) performed in the first 2 days after symptom onset. In the case of episodic vestibular syndrome, the presence or absence of a triggering element helps determine the etiology. The diagnostic algorithm is shown in Fig. 1. This approach is based on current knowledge about vestibular and neurological physiology and pathophysiology and is consistent with strong evidence in the literature. However, it has not yet been validated in the ED [2]. The aim of this study was to evaluate the rate of misdiagnosis in patients with dizziness and vertigo in the ED by comparing the diagnosis of emergency physicians with the conclusive diagnosis of the neurologist, especially regarding VBS. For this purpose, we used the diagnosis algorithm of Edlow et al. [2] and, where necessary, the help of a neurologist expert in vestibular disorders and/or brain MRI.
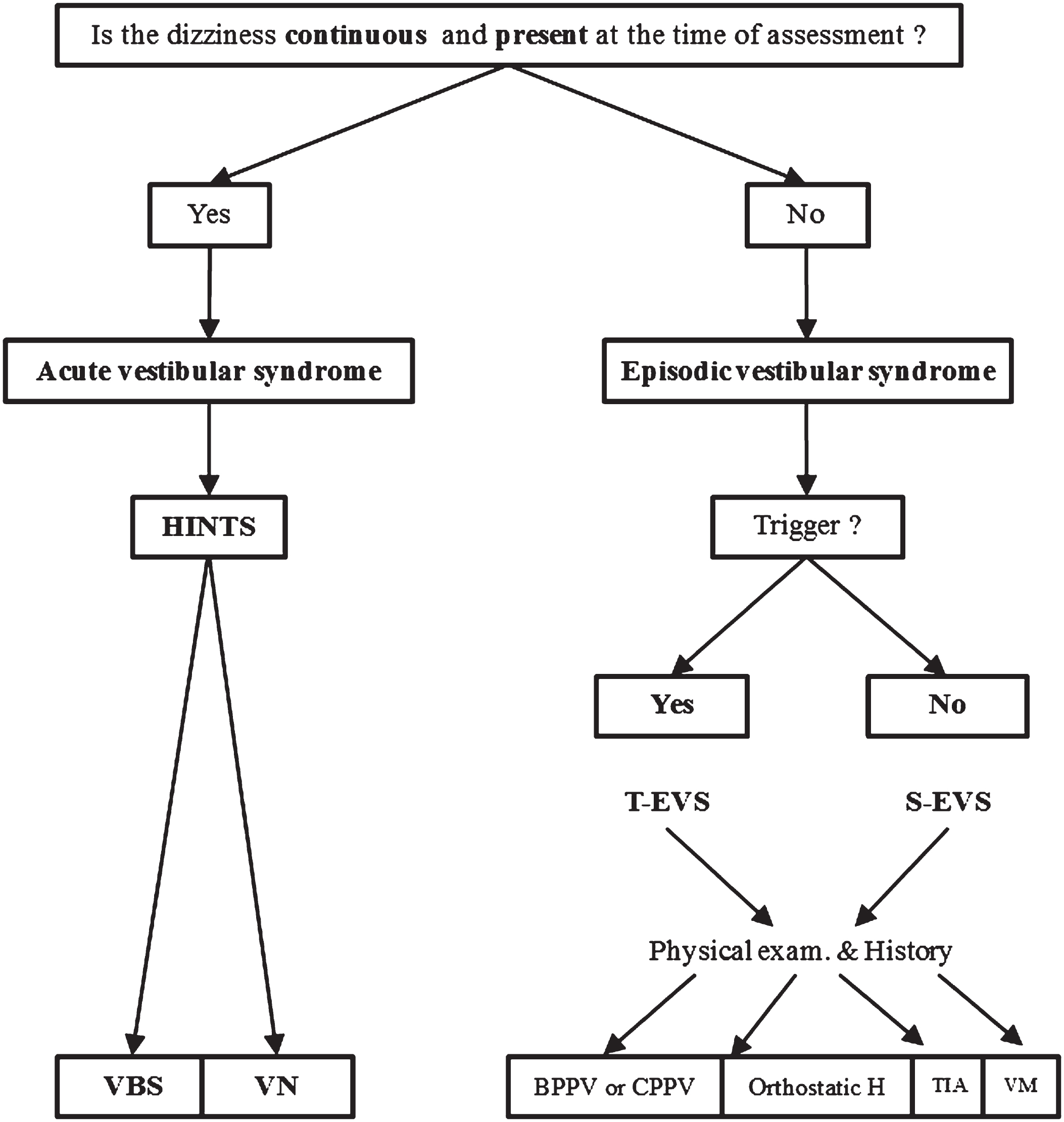
Decision algorithm to differentiate etiologies of vertigo or dizziness (adapted from Edlow et al. [2]). VBS: vertebrobasilar stroke; VN: vestibular neuritis; HINTS: Head Impulse test; Nystagmus; Test of Skew; T- EVS: triggered episodic vestibular syndrome; S-EVS: spontaneous episodic vestibular syndrome; BPPV: benign paroxysmal positional vertigo; CPPV: central paroxysmal positional vertigo; Orthostatic H.: orthostatic hypotension; TIA: transient ischemic attack; VM: vestibular migraine. Causes of misdiagnosis in patients presenting with dizziness or vertigo in the ED.
This 1-year prospective single-center study was conducted at the ED of Brugmann University hospital, an academic care hospital in Brussels, Belgium. It receives approximately 71.900 ED visits annually.
We included patients over 18 years old who visited the ED of the Brugmann University Hospital for isolated vertigo or dizziness from February 2020 to February 2021.
We only enrolled the dizzy patients for whom the ED asked for a neurological evaluation, which explains the relative low number of patients included in the study.
Since the diagnostic approach is solely based on timing and triggering factors of dizziness, the potential risk of bias associated to other terms patients may endorse, like lightheadedness and imbalance, is neglectable.
The COVID-19 pandemic reduced the enrollment, because of the lockdown. Patients who presented with isolated vertigo or dizziness for more than a month at the time of presentation were excluded from the cohort.
No radiologic study was ordered before neurological assessment.
A neurology resident was available for consultation 24 h per day.
The neurology residents were trained by the expert in HINTS and Dix Hallpike (DH) tests.
All patients were first examined by the emergency physician who made the preliminary diagnosis and decided to call a neurology consultant.
The neurological evaluation was available within minutes and in unclear situations the resident took videos which were submitted to his attendee.
The video goggles offered the ability to perform an exam with fixation block, however in acute patients having overt signs and when questions occured, a video-recording with a cell phone was performed. In our study, videonystagmography and video-head impulse test were performed by the expert in vestibular disorders during hospitalization.
The initial diagnosis of the referring emergency physician was shared with the neurology consultant, who made the conclusive diagnosis.
Emergency physicians had not received training in neurovestibular examination before the start of the study. Teaching courses were organized by the neurologist at the end of the study.
The diagnostic algorithm summarized in Fig. 1 was used by the resident neurologist. The HINTS examination was used for AVS. For triggered episodic vestibular syndrome, the DH maneuver was performed, and blood pressure was measured. If the final diagnosis confirmed by the specialist was BPPV, orthostatic hypotension or vestibular neuritis, brain MRI was not performed. If the diagnosis remained unclear after using this algorithm, the patient was assessed by the attending neurologist expert in vestibular disorders for final diagnosis. All patients with the following 3 final diagnoses were subsequently managed by the neurologist: VBS, transient ischemic attack (TIA) and vestibular migraine.
An oto-rhino-laryngologist assessment was required for VN and BPPV.
Non-parametric Cohen’s Kappa test was used to quantify the degree of agreement between two raters in the case of qualitative conclusions (i.e., diagnosis). Cohen’s Kappa test value tends towards 1 when there is greater agreement. This allowed us to compare the diagnosis of central vertigo disorders and VBS proposed by the emergency physician with the final diagnosis retained by the neurologist after the workup.
The χ2 test of independence (χi2) was used to determine statistically significant associations between two or more cardiovascular risk factors and admission to the stroke unit.
The study was approved by the ethical committee of the Brugmann University Hospital (B077202043285/I/U).
Results
Participants
The demographic data of the cohort are presented in Table 1. The study included 66 patients with a mean age of 56 years, with 48% (32/66) women and 52% (34/66) men.
Baseline characteristics of the study population
Baseline characteristics of the study population
Hypertension was the most common cardiovascular risk factor, accounting for 24% (16/66) in our cohort. Data on other cardiovascular risk factors are presented in Table 1. Only 4% (3/66) of patients had a prior history of stroke and 7% (5/66) had a prior history of BPPV.
A total of 14% (9/66) of the patients in this cohort had VBS (Table 2).
Most frequent causes of dizziness in the ED according to etiology retained by emergency physician and neurologist
VBS: vertebrobasilar stroke; TIA: transient ischemic attack; BPPV: benign paroxysmal positional vertigo. (1) Initial benign diagnoses made by the emergency physician, these were: 1 syncope and 1 hypertension. (2) Initial serious diagnoses, mainly vertebrobasilar stroke, made by the emergency physician.
The level of agreement between the emergency physician and the neurologist was low, with a Kappa value of 0.27 for the final diagnosis of central vertigo disorder. A total of 30 patients had central vertigo disorder as final diagnosis and disagreement in diagnosis between neurologists and emergency physicians was found in 6 patients. These 6 erroneous initial diagnoses made by emergency physicians were: 2 unknown origin diagnoses, 1 syncope, 1 hypertension, 2 BPPV. After removing the possible bias of brain MRI and/or hospitalization, the Kappa value was 0,3. Nine diagnoses made by the neurology resident in the ED were modified after imaging and/or hospitalization. Of these diagnoses, 33% were vestibular migraines, 22% were meningiomas of the internal auditory canal, 11% intracranial hypotension.
Regarding the final diagnosis of dizziness due to VBS, the Kappa value was 0,27.
Among a total of 9 VBS as a conclusive diagnosis, 22% (2/9) of the VBS would have been missed if they had only been examined by the emergency physicians (Table 2). For these 2 missed cases of VBS, the initial erroneous diagnoses made by the emergency physicians were syncope and hypertension.
A total of 65% (13/20) of serious initial diagnoses (mainly VBS) presented by emergency physicians were actually benign conditions after neurology consultation (Table 2). The following final diagnoses for these 13 initial serious causes were retained: 4 BPPV, 3 VN, 1 COVID-19, 1 cardiac arrythmia, 1 hypertension, 2 vestibular migraine and 1 functional neurologic disorder (Table 2). Of the 4 patients with BPPV, 3 of them had no DH maneuver done by the emergency physician. Of the 3 patients with VN no HIT was done. The remaining patients had a normal clinical examination.
Of all patients, 39% (26/66) had MRI brain imaging (Diffusion Weighted Imaging, T2 weighted Fluid-Attenuated Inversion Recovery, T2* weighted imaging, Time Of Flight). Computed tomography (CT) angiography of the brain and neck vessels was performed in 74% of patients (49/66) and 86% (57/66) of the final neurologist diagnoses made in the ED before hospitalization and/or brain MRI.
Sensitivity, specificity, positive predictive value and negative predictive value of clinical examination of emergency physician
After excluding final diagnoses that required brain MRI, the sensitivity of ED clinal examination for VBS was 77% (7/9×100), with the specificity being 84% (41/49×100). The positive predictive value (PPV) of the ED clinical examination for VBS was 47% (7/15×100). The negative predictive value (NPV) of the ED clinical examination for VBS was high at 96% (41/43×100).
For 51 benign conditions (final diagnoses) where in-hospital treatment was not required (for example: BPPV, VN, vestibular migraine), the sensitivity of ED clinal examination for benign conditions was low at 56% (28/50×100), with the specificity being 88% (14/16×100). The PPV of the ED clinical examination for benign conditions was 93% (28/30×100). The NPV value was low at 39% (14/36×100).
Rate of misdiagnosis of dizziness in the ED
For all diagnoses combined, 62% (41/66) of the diagnoses of dizziness and vertigo made in the ED were later corrected by the neurologist. The neurology resident was reachable all the time and had to ask his supervisor validation for only 4 cases.
Causes of misdiagnosis in patients presenting with dizziness or vertigo in the ED
Table 2 reports the different identified etiologies of dizziness or vertigo initially made by the emergency physician and after evaluation by the neurologist. The four causes of misdiagnosis in patients presenting with dizziness or vertigo in the ED are illustrated in Fig. 2.

Causes of misdiagnosis of patients presenting with dizziness and vertigo in the emergency department.
Neurological examination errors also seemed to be a cause of misdiagnosis. Other two causes of misdiagnosis were patient history relating to the description of vertigo (e.g., frequency, position, duration) and the DH maneuver not being performed or being misinterpreted.
Finally, we used the χi2test to check if the presence of two or more cardiovascular risk factors was more frequently associated with admitting a patient to the stroke unit (Table 1). Among 20 patients hospitalized in the neurovascular unit, 60% (12/20) had two or more cardiovascular risk factors (Table 1). This was statistically significant (p = 0.015).
Discussion
The agreement between emergency physicians and neurologists regarding the conclusive diagnosis for patients with dizziness is low.
To the best of our knowledge, the only study that compared the agreement between two physicians regarding the diagnosis of dizziness is the study of Royl et al. [12], but with a different study design compared to ours: it consisted of retrospective collection of data and the preliminary diagnosis was made by the ED neurologist (trainee) and compared to diagnoses in the medical discharge reports of patients hospitalized following ED presentation or to diagnoses in ED reports of patients who revisited the ED within 4 weeks of their initial presentation. So, these final diagnoses were made by the attending neurologist or were based on the discharge diagnosis after hospital admission. The authors showed that 44% of dizziness diagnoses made by the trainee neurologist were subsequently corrected by the attending neurologist [12]. In our study, 62% (41/66) of the diagnoses of dizziness and vertigo made in the ED by the emergency physician were later corrected by the neurologist. Furthermore, in the study of Royl et al. [12], 6% of benign diagnoses were corrected to “dangerous,” mainly VBS. We found a lower rate of 3% (2/66) (Table 2). On the other hand, we found that 65% of initial serious diagnoses in the ED were corrected to benign, which is a high rate compared to 23% found in the study of Royl et al. [12]. This could be explained by the low sensitivity of 56 % of ED clinal examination for benign conditions, a PPV of 47% for the ED clinical examination of VBS and the fact that the initial diagnoses in Royl et al. were made by the trainee neurologist.
To sum up, their findings contrast with our study, but we cannot say that we have the same conclusion because of several causes: the study design is different, their neurology trainees were trained in the vestibular exams and used Frenzel lenses. However, their neurology trainees still came out with a high “misdiagnosis” rate.
The most frequent causes of misdiagnosis in patients presenting with dizziness or vertigo in the ED in our study were related to differences in history between the emergency physician and neurologist, and with the patient changing his/her story over time. In some cases, the description of the patient’s clinical history was unreliable or insufficiently detailed. Some details about dizziness were missing, e.g., frequency, positional nature and duration (Fig. 2). Misdiagnosis also occurred when the clinical examination such as neurological examination or DH maneuver was not performed or was misinterpreted in the ED. To avoid misdiagnosis of VBS in the ED, clinical examination is the most relevant item to consider in the ED. Of the 5 patients with VN diagnosed by the neurologist and confirmed by the oto-laryngo-logist (Table 2), 4 presented a positive HIT, which was not tested by the emergency physician initially. In 6 patients a misinterpretation of nystagmus lead to a wrong diagnosis; for example, physiological nystagmus was interpreted as pathological and gaze-evoked nystagmus was not seen as a central cause of vertigo.
The head impulse test (HIT) is the most sensitive test to perform in patients with AVS, as it can assess the vestibulo-ocular reflex. It is therefore regarded as the most important test of the HINTS examination to differentiate VN from VBS. Positive HIT is suggestive of peripheral vestibular deficit. HIT is estimated to be negative in 80–100% of VBS but positive in 83–100% of VN [5]. In this study, 80% (4/5) of bedside HIT were positive, thus indicating VN. Nevertheless, it is widely known that HIT is examiner dependent. Machner et al. showed that the specificity (VBS with normal HIT) of bedside HIT performed by a non-expert (i.e., emergency physician) is 64% compared to nearly 100% when performed by an expert (i.e., neurologist), whereas the specificity of the video HIT is 100% when performed by non- experts [5].
Recording oculovestibular reflexes and catch-up saccades using a mobile device allows for the quantitative analysis of the deficit and a posteriori reassessment of the results by other physicians [5]. Explaining the principles of HINTS to emergency physicians and providing training in the use and interpretation of bedside and video HIT would save valuable time in the care of VBS.
The DH maneuver is underutilized in the ED, as our findings showed that 25% of misdiagnoses are related to the underutilization and/or difficulty in interpreting the DH maneuver (Fig. 2). When a patient presents a positional dizziness or vertigo with a positive DH maneuver, its sensitivity is 100% for BPPV [6]. In this study, the DH maneuver was performed by emergency physicians in only 28% (4 /14) of the patients with BPPV as final diagnosis confirmed by the otolaryngologist. Rau et al. found similar results with the DH maneuver being performed in 24% of 41 patients with BPPV [11]. Nevertheless, the failure to carry out the DH maneuver gives rise to expensive, unhelpful, and potentially irradiating examinations such as brain CT scans [11, 13].
Triggered episodic vestibular syndrome can also be a stroke. Indeed, VBS is not always expressed as AVS. We report that 67% (6/9) of VBS were AVS, while 33% (3/9) were triggered episodic vestibular syndrome. This central paroxysmal positional vertigo (CPPV) may be accompanied by downbeating nystagmus triggered by a change in position (e.g., DH maneuver) [4–10].
In order to have a systematic approach each time a dizzy patient is admitted to the ED, ‘TI.TR.A.T.E.’ is an acronym proposed by Newman-Toker et al. [11], for
Cardiovascular risk factors are not the most sensitive factors for admission to the stroke unit (Table 1). There was a statistically significant association (p = 0.015) between the presence of two or more cardiovascular risk factors and admission to the stroke unit. Mandge et al. recently demonstrated that cardiovascular risk factors have poor sensitivity (12.5%) for VBS [6]. Gaze-evoked nystagmus and ataxia grade 2-3 (severe imbalance with standing or falling in the upright posture) combined had a sensitivity of 100% (92% for ataxia alone) [6]. The HINTS examination had a sensitivity of 100% and specificity of 96% for VBS, which exceeds brain MRI in the first 48 hours [5, 6]. Gaze-evoked nystagmus, ataxia grade 2-3 and HINTS are the most sensitive factors for admission to the stroke unit [6, 5].
Diffusion-weighted MRI can be completed by a study of brain perfusion when VBS is suspected. We admitted nine patients with VBS to the stroke unit, including four patients with negative diffusion-weighted MRI findings. Among these 4 patients, the first patient had gaze- evoked nystagmus and ataxia grade 2. The second had ataxia grade 3 that resolved after thrombolysis within 90 minutes and cerebellar hypoperfusion on brain perfusion CT. The third patient had left ptosis, left arm dysmetria, and ataxia grade 2 with complete thrombosis of the left vertebral artery on CT angiogram. The last patient had ataxia grade 3 and skew deviation.
The negative diffusion-weighted MRI of the four patients diagnosed with VBS could be explained by several factors. In two patients, the brain MRI was performed within 24 hours of symptom onset and in one patient within 48 hours. Machner et al. reported that 50% of diffusion-weighted MRI of the brain can be false negatives within the first 48 hours for small VBS [8]. Finally, one patient had cerebellar hypoperfusion on cerebral perfusion CT, while diffusion-weighted MRI of the brain was negative. Because there was no installed necrosis the patient was treated with IV thrombolytic therapy within 90 minutes. Choi et al. recently conducted a study on patients with spontaneous episodic vestibular syndrome, showing that 43% of patients with confirmed VBS had a negative diffusion-weighted MRI of the brain (performed within 24 hours of symptom onset in 91% of patients). Overall, 12% of these patients showed cerebellar hypoperfusion on perfusion-weighted MRI of the brain [1]. Therefore, diffusion-weighted MRI of the brain should ideally be performed 48 hours after symptom onset and preferably with perfusion brain CT or MRI in order to reduce the rate of VBS with false-negative diffusion-weighted MRI.
Limitations
Our study has several limitations because only a relatively small number of patients were included given the COVID-19 pandemic because of the lockdown period, which limited recruitment.
The patients included in the study are only those for whom a neurological consultation was requested by the emergency physicians, therefore we have a selection bias in our study. This bias would likely lower the rate of misdiagnosis.
Besides, the term ’misdiagnosis’ is a misuse of language because the purpose of the ED is not always to make the right diagnosis, but rather to gather enough information to make a safe disposition for the patient.
This often leads to a change in the final diagnosis made by the inpatient team and does not necessarily represent a misdiagnosis at the ED, a term we often used in this paper. Of course, time-dependent diagnoses (such as acute stroke within the therapeutic window) do need to be made urgently.
Conclusions and perspectives
This study shows that there is a substantial rate of misdiagnosis in patients with dizziness caused by VBS in the ED. To reduce the number of missing diagnoses of VBS in the future, there is a need to train physicians, especially emergency physicians in neurovestibular examinations, including the HINTS examination for AVS and the DH maneuver for episodic vestibular syndrome. Although time is limited in the management of VBS, a detailed medical history is essential to obtain the correct diagnosis. Using the acronym ‘TI.TR.A.T.E.’ as a mnemonic tool in order to have a systematic approach with every dizzy patient in the ED, could also be helpful. Brain perfusion imaging (CT or MRI) has an additional diagnostic value, because it can help detect VBS with a negative diffusion-weighted MRI. Finally, the utilization of video HIT in the ED could be of interest to avoid overlooking VBS. Further prospective studies are needed to confirm this hypothesis.
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Footnotes
Acknowledgments
We gratefully acknowledge the advice on the statistical analysis of the data by Lonnet Germain. We gratefully thank Oprea Elena for her precious advices.