
Abstract
BACKGROUND:
Our sense of direction (SOD) ability relies on the sensory integration of both visual information and self-motion cues from the proprioceptive and vestibular systems. Here, we assess how dysfunction of the vestibular system impacts perceived SOD in varying vestibular disorders, and secondly, we explore the effects of dizziness, migraine and psychological symptoms on SOD ability in patient and control groups.
METHODS:
87 patients with vestibular disorder and 69 control subjects were assessed with validated symptom and SOD questionnaires (Santa Barbara Sense of Direction scale and the Object Perspective test).
RESULTS:
While patients with vestibular disorders performed significantly worse than controls at the group level, only central and functional disorders (vestibular migraine and persistent postural perceptual dizziness), not peripheral disorders (benign-paroxysmal positional vertigo, bilateral vestibular failure and Meniere’s disease) showed significant differences compared to controls on the level of individual vestibular groups. Additionally, orientational abilities associated strongly with spatial anxiety and showed clear separation from general dizziness and psychological factors in both patient and control groups.
CONCLUSIONS:
SOD appears to be less affected by peripheral vestibular dysfunction than by functional and/or central diagnoses, indicating that higher level disruptions to central vestibular processing networks may impact SOD more than reductions in sensory peripheral inputs. Additionally, spatial anxiety is highly associated with orientational abilities in both patients and control subjects.
Keywords
Introduction
Sense of direction (SOD) can be defined as our ability to orientate ourselves within our local environment and to know in which direction objects are [48]. SOD is a complex multi-sensory process involving the integration of self-motion cues with optic flow information sensing our external environment, which is integrated at multiple levels of the neuraxis and under cognitive control [43]. The vestibular system in particular, provides sensory information on head accelerations in three-dimensional space and is known to be a key contributor to spatial orientation in the absence of visual cues [21, 41]. However, the relative importance of vestibular input to everyday SOD ability remains unclear. Many individuals are aware of having a good or poor self-perceived sense of direction ability but questionnaire tools, mainly the Santa Barbara Sense of Direction (SBSOD) scale, provide a quantitative assessment of subjective SOD skills which is representative of real-world navigational ability [25]. In addition, psychometric assessments such as the Object Perspective test [32], are useful tools to evaluate cognitive visuospatial components to SOD such as spatial updating and object orientation.
Few studies have investigated the impact of vestibular system dysfunction on SOD and, to our knowledge, no studies have compared SOD ability and the interaction of symptom effects in a large and multiple diagnoses cohort. This is important, as despite the fact that dizziness, disorientation, and vertigo symptoms commonly arise from a mismatch in visuo-vestibular processing in many disorders, mechanisms underlying differing diagnoses are diverse. Whilst structural disorders are often the consequence of physical lesions to the peripheral vestibular system, functional vestibular disorders involve more complex maladaptation of vestibular information processing in higher cortical circuitry and may be exacerbated by underlying psychological components. As such, a key question is to what extent does the form of vestibular pathology affect orientational ability? We hypothesise that dizziness and psychological symptoms, as well as overall SOD ability, likely show high variability between vestibular diagnoses. In order to assess this, we recruited a diverse cohort of patients with varying vestibular disorders, including clear peripheral vestibular diagnoses such as benign paroxysmal positional vertigo (BPPV), bilateral vestibular failure (BVF) and Meniere’s disease (MD), as well as central/functional disorders of vestibular migraine (VM) and persistent postural perceptual dizziness (PPPD) which both lack obvious physical or structural aetiology. In addition, assessing patients with BVF may help answer a more fundamental question, namely, how critical is vestibular input (severely reduced in these patients) to human SOD? Although vestibular input is essential to angular spatial orientation in the dark [34, 18], we usually refer to day-to-day SOD as an activity taking place within the visual world. Indeed, questionnaires such as the SBSOD relate to sense of orientation and direction with respect to external visual objects. Therefore, the prominent role of visual-cognitive cues in humans may mask any effects of vestibular loss on the perceived sense of direction as commonly assessed with questionnaires. Moreover, disrupted cortical processing of multisensory visual and self-motion information associated with functional vestibular disorders may impair SOD abilities even when peripheral vestibular function remains intact.
Additionally, psychological symptoms such as anxiety and depression are often concomitant in patients with vestibular disorder and may act to worsen disorientation symptoms arising from vestibular dysfunction and prolong effective recovery [8, 44]. Moreover, 10% of people who report vestibular symptoms receive a primary diagnosis of an anxiety disorder and thus such disorders represent the most prevalent psychiatric association with vestibular-like symptoms. Accordingly, it has previously been shown that comorbid psychiatric symptoms act to worsen clinical outcomes in vestibular disorders and have consequently been shown to be the strongest predictors of persistent dizziness symptoms in some patients, as opposed to actual vestibular deficits [7, 22]. However, although general anxiety may be heightened in patients, common symptom questionnaires do not separate a spatial component of anxiety, which is likely more relevant to patients suffering from dizziness symptoms. Similarly, susceptibility to migraine also impedes recovery and aggravates vertigo in vestibular disorders [3], yet the effect of migraine symptoms on sense of direction remains unknown. In this study we implemented the Spatial Anxiety Questionnaire [34] to assess anxiety experienced by patients in spatially challenging environments, as well as other validated symptom questionnaires to establish the effect of psychological and migraine symptoms on orientational abilities in varying vestibular diagnoses.
Hence, our primary aim was to assess whether vestibular dysfunction impairs SOD ability by comparing orientation measure scores between a healthy control cohort and patients on the group level. Following aims were to then assess differences in SOD ability between varying vestibular diagnoses, and to explore the interactions of symptomatic dizziness, psychological comorbidity and migraine factors with SOD ability in patient and control groups.
Methods
Participants
A total of 87 patients with varying vestibular disorders (13 benign paroxysmal positional vertigo, 12 bilateral vestibular failure, 12 Meniere’s disease, 20 vestibular migraine and 30 persistent postural perceptual dizziness) were recruited according to B
All participants provided data by completing general health questions: gender (M/F), age (years), height (m), weight (kg) as well as six clinically validated questionnaires (see below). A single question asked if patients felt their SOD had changed as a result of their condition. Upon completion of the questionnaire battery, all participants were prompted to take the Object Perspective test [32], however responses were only received for a total of 43 healthy participants and 51 patients.
Dizziness Handicap Inventory (DHI)
The DHI assesses disability due to dizziness via 25 items categorised into functional, physical and emotional components of disability [28]. Each item is scored as: yes =4, sometimes =2, no =0, with a maximum disability score of 100. A score range of 16–34 is indicative of mild handicap symptoms, 36–52 suggests moderate symptoms, and a score of 54 or higher indicates severe handicap symptoms.
Visual Vertigo Analogue Scale
The Visual Vertigo Analogue Scale consists of 9 items on which participants rate their perceived dizziness on a scale between 0 (no dizziness) and 10 (most dizziness) in different visual vertigo-inducing environments [12]. Total visual vertigo severity is calculated as a percentage: (score for each item/number of items answered) *10. Participants are considered positive for visual vertigo symptoms if they scored 1 or above on two or more items, reflecting a minimum combined threshold of 2.22.
Migraine Screen Questionnaire
The Migraine Screen Questionnaire is a 5-item questionnaire used to screen for migraine symptoms [33]. Each item is scored as: yes =1 or no =0, for a total score of 5 points. A score ≥4 indicates likely migraine symptoms.
Hospital Anxiety and Depression Scale (HADS)
The HADS questionnaire screens for anxiety (HADS A) and depressive (HADS D) states in non-psychiatric populations, consisting of 14 items sub-divided between two respective anxiety and depression subscales [51]. Each item is scored on a (0–3) 4-point Likert scale for a total score of 21 on each scale, with score ranges of 0–7 = normal, 8–10 = borderline abnormal, 11–21 = abnormal.
Santa Barbara Sense of Direction Scale (SBSOD)
The SBSOD consists of 15 items (e.g. ‘I am very good at judging distances’) which are each scored on a 1–7 point Likert scale ranging from ‘Strongly Agree’ to ‘Strongly Disagree’ [25]. Total score is calculated by: (score for each item/15), with a maximum score of 7.0 indicating greatest sense of direction ability.
Spatial Anxiety questionnaire
The Spatial Anxiety questionnaire asks participants to rate their experienced anxiety in 8 different spatially challenging environments (e.g., ‘Finding my way to an appointment in an unfamiliar area of a city or town’) on a 5-point Likert scale between: ‘Not at all’ = 0, to ‘Very much’ = 4 [34]. Total score is equal to the sum of scores for each item with a maximum score of 32 indicating highest severity of spatial anxiety symptoms.
Object Perspective test
The Object Perspective test is a 12-item assessment of cognitive SOD ability involving the drawing of imagined headings between objects in a circular array and has shown consistency with similar tests of spatial cognition [32]. The test was adapted for online use (Supplementary Fig. 1). Total score was calculated as the number of responses falling within 90° of the correct heading direction. A test of validation between the two test methods in 18 subjects showed acceptable correlation (r = 0.74, p < 0.01) and no significant difference between mean scores (paired-sample t-test: t(17) = 0.861, p = 0.40).
Statistical analysis
Parametric comparison of group means was achieved using one-way ANOVA with post-hoc Tukey’s correction. Non-parametric Mann Whitney U and Kruskal-Wallis H tests with post-hoc Dunn-Bonferroni correction for multiple comparisons were conducted following a significant result for Levene’s test for equality of variances (p < 0.05). A two-tailed p-value < 0.05 was used to detect statistical significance. Univariate linear regression was used to investigate associations between SBSOD and symptomatic questionnaire scores. Additionally, we conducted exploratory factor analysis through principal component reduction to identify latent variables influencing main orientation and symptom variables. Specifically, we aimed to assess whether orientational abilities, as quantified by SBSOD and Object Perspective test scales, are associated with psychological factors such as (generalised or spatial) anxiety or depression, in the control or patient populations. Principal components were selected on the basis of an eigenvalue > 1 and pattern matrices were subjected to oblimin rotation due to correlation between orientational and symptomatic variables. Values lying > 3 standard deviations from the group mean were considered outliers and excluded from analyses. IBM SPSS Statistics v28.0 was used for statistical analysis and plots were generated using the Seaborn package in Python (3.9.13).
Results
Demographic characteristics
Demographics and other characteristics are shown in Table 1. Age ranged from 17 to 82 years with no significant differences observed in mean age across groups (F(5,150) = 1.81, p = 0.11). All but Meniere’s disease and control groups showed a majority female gender distribution (Table 1), which was significant (Chi-square: 15.3, df: 5, p < 0.01). All vestibular disorder groups had a majority dizziness duration of > 24 months, with small but significant differences (Chi-square: 16.1, df: 8, p < 0.05) mainly due to slightly shorter durations in the BPPV group.
Demographic characteristics in control and patient groups (Mean+SD or %)
Demographic characteristics in control and patient groups (Mean+SD or %)
Note. BPPV Benign Paroxysmal Positional Vertigo; BVF Bilateral Vestibular Failure; MD Meniere’s Disease; VM Vestibular Migraine; PPPD Persistent Postural-Perceptual Dizziness.
Distributions of age, dizziness disability (DHI, Visual Vertigo Analogue Scale), migraine symptom scores (Migraine Screen Questionnaire), anxiety and depression (HADS A & D), Spatial Anxiety Questionnaire, Santa Barbara Sense of Direction (SBSOD), and Object Perspective test scores in control subjects and patients are shown as kernel density estimations in Supplementary Fig. 2. Means and standard deviations together with controls versus combined patient groups comparisons are given in Supplementary Table S1. (Spatial Anxiety Questionnaire, SBSOD, Object Perspective test are considered in detail in the next section of results). Mean scores for controls were below the minimum established thresholds (see methods) indicative of mild symptoms on the DHI (2.6±4.1), migraine screen questionnaire (1.2±1.6) and HADS (A: 4.5±3.3, D: 2.8±2.7) scales. Control subjects showed minimal evidence of visual vertigo symptoms with a mean score of 2.5±3.6 close to the minimum threshold on this scale. Mean score in all patient groups was significantly higher than control subjects on the DHI (H(5,156) = 115.2, p < 0.001) and for all patient groups except those with BPPV on the Visual Vertigo (H(5,156) = 91.1, p < 0.001) scale. No difference was seen between vestibular groups. Both PPPD and VM groups showed significantly higher migraine scores compared to control subjects (H(5,156) = 30.63, PPPD: p < 0.001, VM: p < 0.001) and scored significantly higher on the HADS A (H(5,156) = 39.1, PPPD: p < 0.001, VM: p < 0.001) and HADS D (H(5,156) = 39.6, PPPD: p < 0.001, VM: p < 0.001) scales. A comparison of mean migraine scores in PPPD patients with no confirmed history of VM or other migraine symptoms was also elevated compared to control subjects (U = 824.0, p < 0.01). However, no significant differences were observed for Migraine Screen Questionnaire, HADS A or HADS D scales between any of the vestibular groups (p > 0.05).
Performance on orientational measures is worse in patients compared to controls and is also linked with greater dizziness disability
A comparison of mean SBSOD score between healthy controls (N = 69) and all vestibular groups (N = 87) showed that mean score for patients was significantly lower on this scale (U = 2101.0, p < 0.001) (Fig. 1A). Similarly, patients scored significantly lower on the Object Perspective test (U = 630.0, p < 0.001) (Fig. 1C) and higher on the Spatial Anxiety Questionnaire (U = 1734.0, p < 0.001) compared to control subjects (Fig. 1B). SBSOD was significantly associated with spatial anxiety in vestibular patients (R2 = 0.44, p < 0.001). Moreover, 68.8% of patients said they experienced no change in their SOD following their diagnosis, whilst 31.3% claimed it had worsened. Interestingly, patients who rated their SOD as worse scored significantly higher on the DHI (U = 507.5, p < 0.05) and Spatial Anxiety Questionnaire (U = 324.0, p < 0.001) and significantly lower on the Object Perspective test (U = 147.5, p < 0.05) compared to those who experienced no change in SOD ability (Fig. 2). No effect of age was observed on SBSOD or Object Perspective test score in either control subjects or patients (p > 0.05).
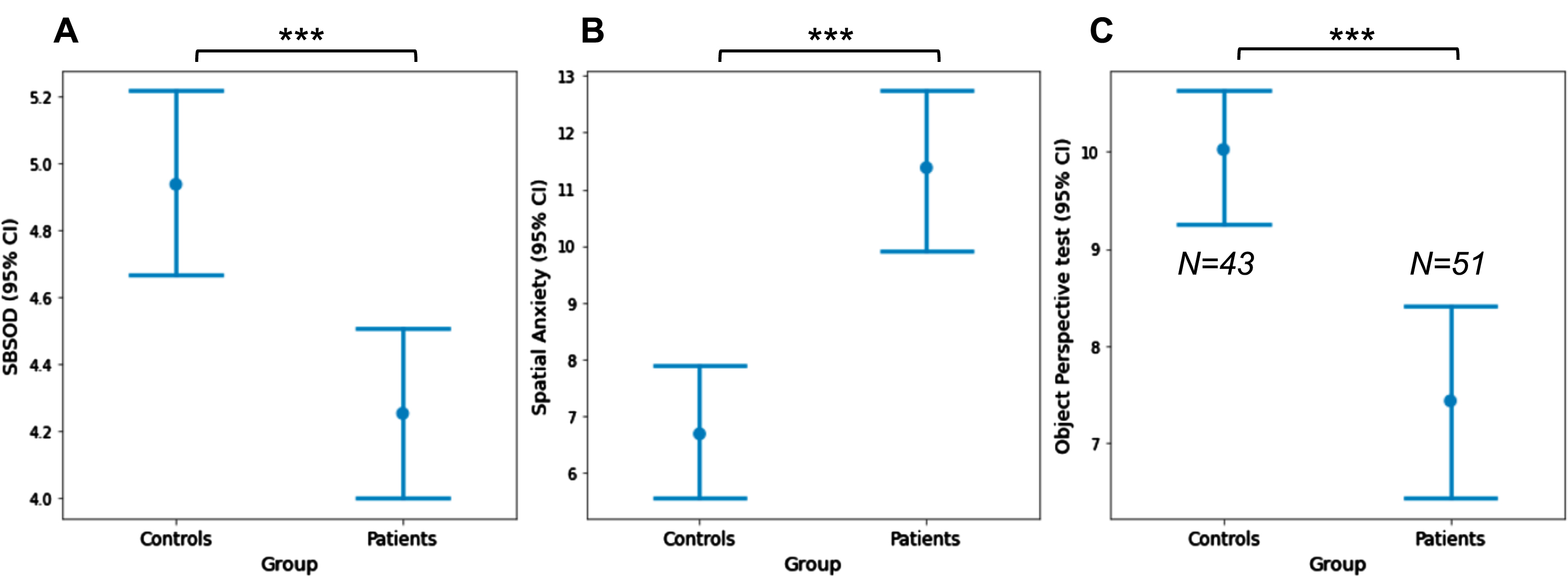
Mean and 95% confidence interval for A) Santa Barbara Sense of Direction, B) Spatial Anxiety Questionnaire and C) Object Perspective test score in control and patient groups. Means compared via Mann-Whitney U test. *p < 0.05, **p < 0.01, ***p < 0.001. N = 87 patients and N = 69 healthy controls except as indicated in C.
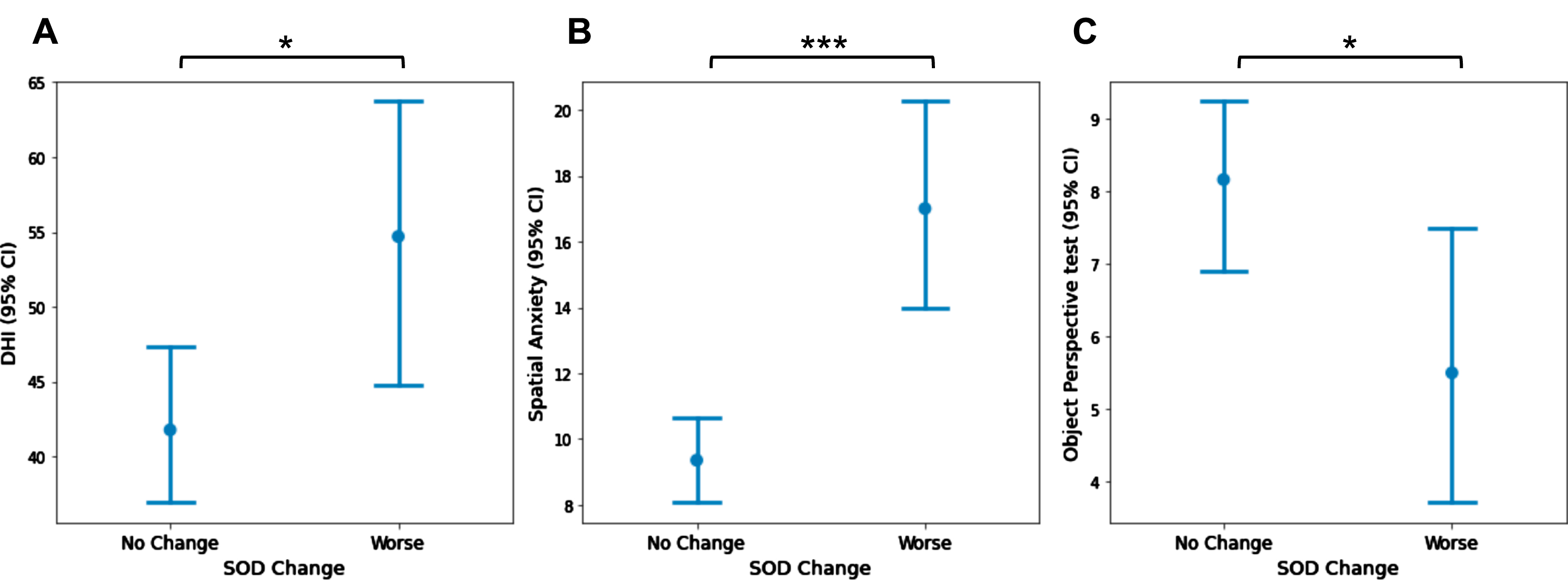
Mean and 95% confidence interval on A) the Dizziness Handicap Inventory, B) Spatial Anxiety Questionnaire and C) Object Perspective test scales for patients who rated their SOD as having either worsened (N = 23) or remained unchanged (N = 63) since their diagnosis. Means compared via Mann-Whitney U test. *p < 0.05, **p < 0.01, ***p < 0.001.
To assess whether SOD ability varied depending on aetiology of vestibular dysfunction, mean scores for main SBSOD, Spatial Anxiety Questionnaire and Object Perspective test variables were compared across patient groups and controls (Fig. 3). Most patient groups displayed a lowered SBSOD score in comparison to control subjects (Fig. 3A), however this effect was only statistically significant in patients with vestibular migraine (p < 0.05). For the Spatial Anxiety Questionnaire (Fig. 3B), PPPD and vestibular migraine groups alone scored significantly higher than controls (PPPD: p < 0.01, VM: p < 0.001). For the Object Perspective test (Fig. 3C), only patients with PPPD scored significantly worse than control subjects (p < 0.05).
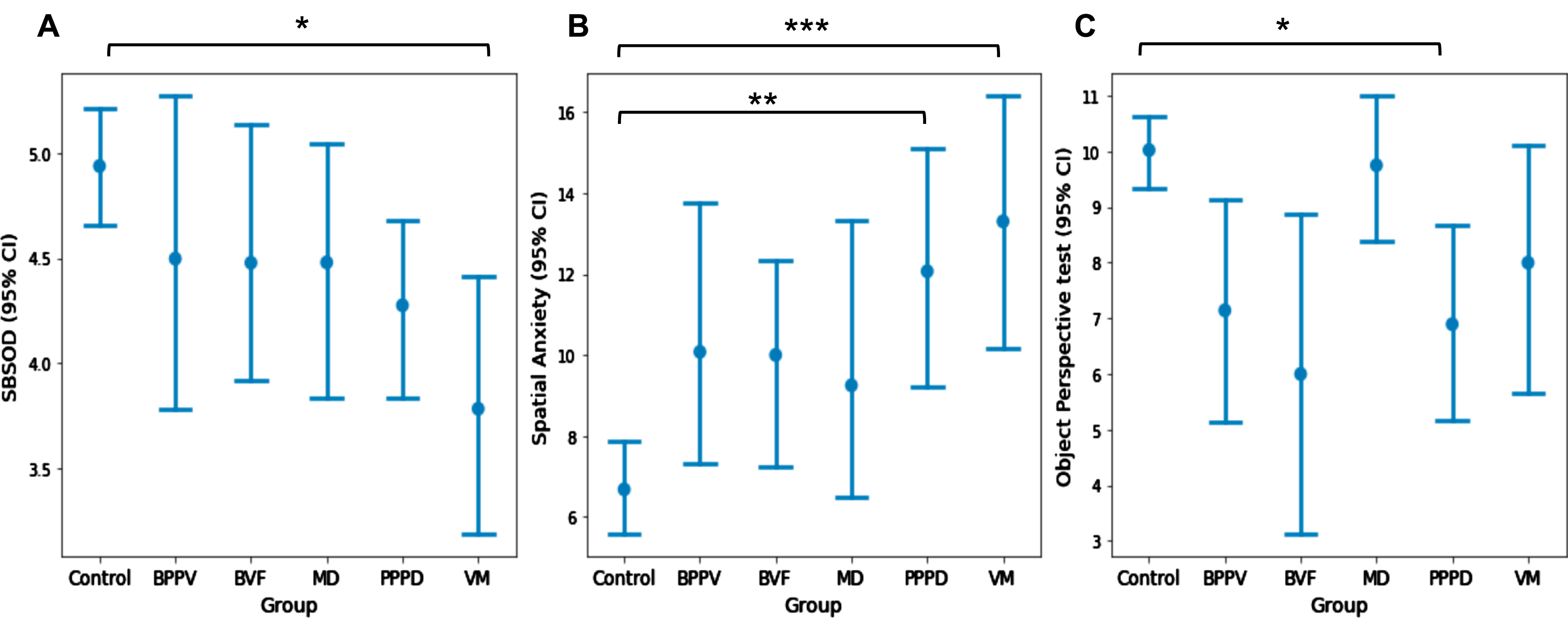
Mean and 95% confidence interval for A) Santa Barbara Sense of Direction scale, B) Spatial Anxiety Questionnaire and C) Object Perspective test score in vestibular groups and control subjects. Means compared via Kruskal Wallis test with post-hoc Dunn-Bonferroni correction. *p < 0.05, **p < 0.01, ***p < 0.001.
Linear regression analysis was used to investigate whether sense of direction, as measured by the SBSOD questionnaire, was associated with other questionnaire variables. In control subjects, the HADS and Spatial Anxiety questionnaires showed significant negative association with SBSOD score (HADS A: R2 = 0.19, p < 0.001, HADS D: R2 = 0.09, p < 0.01, Spatial Anxiety Questionnaire: R2 = 0.42, p < 0.001), whilst the Object Perspective test showed a positive association (R2 = 0.10, p < 0.05).
Exploratory factor analysis across questionnaire variables
Exploratory factor analysis was used to assess possible latent variables across symptomatic (DHI and HADS) and orientational measures (SBSOD, Object Perspective test and Spatial Anxiety Questionnaire). Three factors were identified in control subjects, however the two main components explained 37.6% and 23.2% of the variance in the sample respectively, whereas the third component only loaded a single variable (Visual Vertigo) and explained a small 15.4% of sample variance. The individual components and their loadings are shown in Table 2, where component 1 (37.6% of the variance) heavily loads the ‘orientational’ components, namely SBSOD, Spatial Anxiety Questionnaire and the Object Perspective test. In contrast, component 2 (23.2% of the variance) loads the HADS Anxiety and Depression factors as well as the DHI, presumably quantifying the low levels of dizziness and/or disorientation present in the normal population [39].
Factor analysis component loadings in controls and vestibular patients
Factor analysis component loadings in controls and vestibular patients
Note. Factor loadings for principal component analysis of questionnaire measures in Control subjects (N = 43) and Vestibular patients (N = 51) with Oblimin rotation.
Two main components were identified in patients with component 1 explaining 49.69% of the variance, while the second component explained 14.57% of the total variance. The pattern matrix in Table 2 shows that component 1 loads all symptomatic variables (DHI, Visual Vertigo, HADS Anxiety and Depression), but not the orientational measures. In contrast, component 2 loads orientational abilities strongly but not the subjective psychological or vestibular-related symptoms (with a standard loading cutoff of 0.4, the only symptom near this value would be HADS Anxiety at 0.36). Segregation between the loading of individual components is clear cut, that is, components load heavily on one but not on both factors identified.
The initial aims of this study were to evaluate the effect of vestibular dysfunction on sense of direction ability as quantified by the SBSOD and Object Perspective test measures, as well as secondary effects of dizziness, migraine and psychological symptoms across vestibular groups and control subjects. Overall, these results indicate that sense of direction and the related variables depicted in Fig. 1, are not so much affected by the loss of peripheral vestibular function, but by central or functional disorders (VM and PPPD). Moreover, perceived sense of direction shows association with experience of task-specific spatial anxiety, rather than generalised anxiety symptoms in both patient and control groups.
In terms of understanding the peripheral vestibular system’s contribution to sense of direction ability, we focus on patients with bilateral vestibular failure. Our diagnostic criteria included a 90% or greater reduction in vestibular function, as such this group could help in assessing whether normal vestibular function is essential for human sense of direction and orientation abilities. Perhaps unexpectedly, however, as Fig. 3 indicates, the BVF group do not show statistically significant differences on orientation measures with respect to control subjects, despite this group showing relatively low mean scores for both the SBSOD and Object Perspective test scales. Notably, considerable variation was observed in this group with individual-level inspection highlighting that the worst performing patient was an outlier 70 year old woman with multiple comorbidities, including diabetes, essential tremor with pendular pseudo-nystagmus [9], polypharmacy, antidepressant drugs and recurrent vertigo episodes fulfilling diagnostic criteria for vestibular migraine. Thus in general, our results indicate that bilateral vestibular hypofunction per se, does not appear to significantly impact sense of direction as assessed by the orientation measures used here.
Despite the small numbers of studies which have explored SOD and vestibular dysfunction, this finding is nonetheless reflected by previous work [13], in which patients with chronic bilateral vestibular failure perform similarly to control subjects in implicit and explicit perspective-taking tasks. Also supportive are results of experiments with purely vestibular navigation tests in normal volunteers, where performance levels in simple angular navigation tasks are not associated with SBSOD scores [49]. Conversely, a recent study reported an association between lower SBSOD score and saccular vestibular loss (absent C-VEMPs) [20]. We believe this finding, dictated by 3 subjects (out of 52) with bilaterally absent C-VEMPs, is limited by low subject numbers and the implausibility that short latency saccular reflexes are involved in SOD processing in humans (Nb recall that the sacculus senses linear acceleration along the longitudinal body axis, a kind of motion not relevant to human sense of direction). Since initial submission of our work, another study has reported deficits in Object Perspective test performance in a group of patients combining bilateral and unilateral peripheral vestibular lesions [18]. However, this work selected patients more on the basis of vestibular test results rather than clinical diagnosis, hence a comparison with our data is difficult. For instance, although the authors did not investigate PPPD patients, anxiety levels in peripheral patients were noticeably high, with two thirds classifying as moderately or severely anxious. Thus, this raises the possibility that many of these patients could suffer from PPPD in addition to the underlying vestibular disorder, with the former rather than the latter being associated with a deterioration in Object Perspective test performance.
Nevertheless, the non-significant finding in patients with BVF reported in the present study is further reinforced by the comparable performance of other peripheral vestibular groups, in particular those with Meniere’s disease, who also do not differ significantly from control subjects on main orientation measures. Thus, the lack of difference in SOD among peripheral disorders compared to control subjects likely reflect that these patients rely on visual and/or cognitive components for their sense of direction. Importantly, these components may remain intact or possibly become enhanced following vestibular loss and are likely more relevant to general SOD ability compared to vestibular motion information. This latter point is accentuated by the fact that we report non-significant findings on orientation tasks which are desk-based, which despite their correlation with real-world spatial tasks [25], are nonetheless completed in static environments with minimal vestibular contribution. Results from other studies investigating the effects of broader peripheral vestibular dysfunction on sense of direction specifically are lacking, but studies investigating cognitive spatial orientation abilities as assessed by mental rotation tasks report mixed results [10, 36]. However, although important to overall orientation ability, object manipulation and perspective-taking have been clearly separated as differing cognitive abilities [32]. As such, despite mixed evidence in the available literature, our results align with previous findings indicating that peripheral vestibular information likely contributes minimally to everyday sense of direction.
Consequently, the significant results observed in functional vestibular groups can likely be attributed to the complex neurobiology, prominent psychological factors, and the absence of central vestibular compensation commonly associated with these disorders [1]. The neurobiological mechanisms underlying PPPD remain unclear, however, numerous fMRI studies have consistently revealed functional abnormalities in the parieto-insular vestibular cortex (PIVC), which serves as an integration site for self-motion and visual information related to spatial orientation abilities [27, 42]. In vestibular migraine, cortical depolarisation originating from the occipital pole is thought to trigger trigeminovascular hypersensitivity responsible for headache symptoms, as well as abnormal activity of the central vestibular system [5]. Moreover, research has also revealed a reduction in grey matter volume within the PIVC in patients with VM, which has further been shown to have a negative association with DHI score [50]. Collectively, previous results suggest that functional abnormalities affecting the central vestibular system may disrupt the integration of multisensory inputs, precipitating ongoing symptoms of dizziness and impairing orientation abilities in VM and PPPD. Accordingly, performance on a vestibular-based orientation task has been found to correlate with the amount of long-term vestibular symptoms, including derealisation and depersonalisation, which are often reported by patients with VM and PPPD [30].
Patients with PPPD and VM in the present study showed comparable demographic characteristics to those reported in previous studies, being majority female with a mean age in the late 40s to 50s [16, 37]. Additionally, PPPD and VM groups alone showed elevated psychological symptom severity compared to healthy individuals in our study, also in alignment with prior cross-sectional studies which report highest prevalence of psychiatric comorbidity in patients with VM (49–65%), with much lower prevalence in peripheral disorders of BVF (24%) and BPPV (15%) [14, 17]. Heightened trait anxiety has been associated with disruption of spatial working memory in healthy individuals [35, 47], and has also been associated with increased sensitivity of the vestibular system [19]. Moreover, prior work has suggested that clinical outcome following acute vestibular neuritis is largely influenced by psychological factors in combination with increased visual dependence, not by the extent of peripheral vestibular recovery [11, 38]. While it has been hypothesised that a causal role of psychological factors in functional dizziness may relate to the projection of vestibular afferents to the parabrachial nucleus, a known regulator of emotional processing [4, 29], studies investigating the incidence of premorbid psychiatric disorder in functional dizziness disorders report mixed results [46]. In comparison to aforementioned studies, a critical finding here is that spatial-specific, as opposed to generalised anxiety symptoms, are more associated with SOD ability, which was consistent across the study population.
Correspondingly, correlations between spatial anxiety and both Object Perspective test and SBSOD scales have been shown in previous studies investigating healthy populations [24]. Similarly, yet distinct from sense of direction ability, a recent study demonstrated significant correlation between mental rotation ability and spatial, rather than trait anxiety symptoms and further indicated that the degree of spatial anxiety experienced is not inherently linked to individual trait anxiety [2]. Thus, this appears to support the existence of domain-specific spatial anxiety, which cannot be solely attributed to generalised anxiety symptoms.
In relation to vestibular dysfunction therefore, spatial anxiety may disrupt cognitive spatial abilities such as perspective-taking, as well as hyper-sensitising patients with functional disorders to vestibular inputs. This may lead to poor integration of multimodal sensory information and diminish subjective orientational ability. This effect is further supported by results from factor analysis conducted with the entire patient population as a whole, in which the primary component extracted loaded dizziness and psychological factors heavily, whereas in the secondary component, spatial anxiety showed clear separation from general symptomatic factors but showed strong inverse association with the SBSOD and Object Perspective test. This effect is essentially a mirror image of results in control subjects, as although in both groups the symptomatic and orientation factors remain segregated, the former is dominant in patients and the latter is dominant in control subjects. This is perhaps expected given the much stronger presence of symptoms in patients than in controls. Nevertheless, these results support the notion that experience of a specifically spatial component to anxiety is highly associated with subjective sense of direction in both patients with vestibular disorder and the general population. However, a possible limitation to this finding could relate to a degree of similarity between items on the SBSOD and Spatial Anxiety Questionnaire scales. Whereas the SBSOD relates to one’s perceived sense of direction ability, the Spatial Anxiety Questionnaire focuses on one’s experience of anxiety in various spatially challenging environments. Therefore, the similar constructs of these two measures may raise the possibility of shared variance between the reported scores.
Conclusion
In summary, this study aimed to investigate the impact of varying vestibular disorders as well as symptomatic dizziness and psychological factors on perceived sense of direction ability. Our results indicate that it is central and functional disorders (vestibular migraine and PPPD) rather than diagnoses with peripheral vestibular aetiology that account for impaired orientational abilities in patients when compared to control subjects. Notably, patients with bilateral vestibular failure do not show abnormal perceived sense of direction, indicating that this ability (as measured with the SBSOD scale) does not critically depend on normal levels of vestibular function. Moreover, spatial anxiety and orientational measures exhibit strong negative association with each other and show clear separation from symptomatic factors in both patient and control groups, suggesting that it is specifically spatial anxiety fears rather than generalised trait anxiety that is associated with poorer sense of direction ability. However, the relative contributions of the orientational and symptomatic components to overall sample variance show contrasting influences between groups, with the primary component comprising the dizziness and psychological symptom measures in patients. Although orientational scales used in this study have been shown to be reflective of real-world ability, future work should nevertheless aim to reaffirm these findings adding physical assessments of orientational ability in vestibular patients.
Footnotes
Acknowledgments
The work was made possible by a research grant to AMB (R481/0516) from Dunhill Medical Trust and support from the National Institute for Health Research, Imperial College London Biomedical Research Centre.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request. No experiments were preregistered.