
Abstract
Background
It has long been known that the environment influences the health of working people. Classic examples of occupational diseases, such as silicosis (a miner’s disease), mesothelioma caused by asbestos and deafness due to a noisy working environment, indicate the direct influence of the environment on employees’ health.
However, environmental factors were not included in the two most important disability models of the 1980s: the International Classification of Impairments, Disabilities and Handicaps (ICIDH) [1] (disease ->impairment ->disability ->handicap) and the Nagi model [2] (pathology ->impairment ->functional limitation ->disability). However, the environment was taken into account in the definition of handicap (ICIDH) and disability (Nagi model). Verbrugge and Jette [3] expanded the Nagi model with intervening factors that ‘speed up or slow down’ the pathway between pathology and disability [4]. The International Classification of Functioning, Disability and Health (ICF) [5], the successor of the ICIDH, was strongly influenced by the Handicap Creation Process model that has fostered widespread research on the nature and impact of the environment (Whiteneck and Dijkers [6]).
The ICF
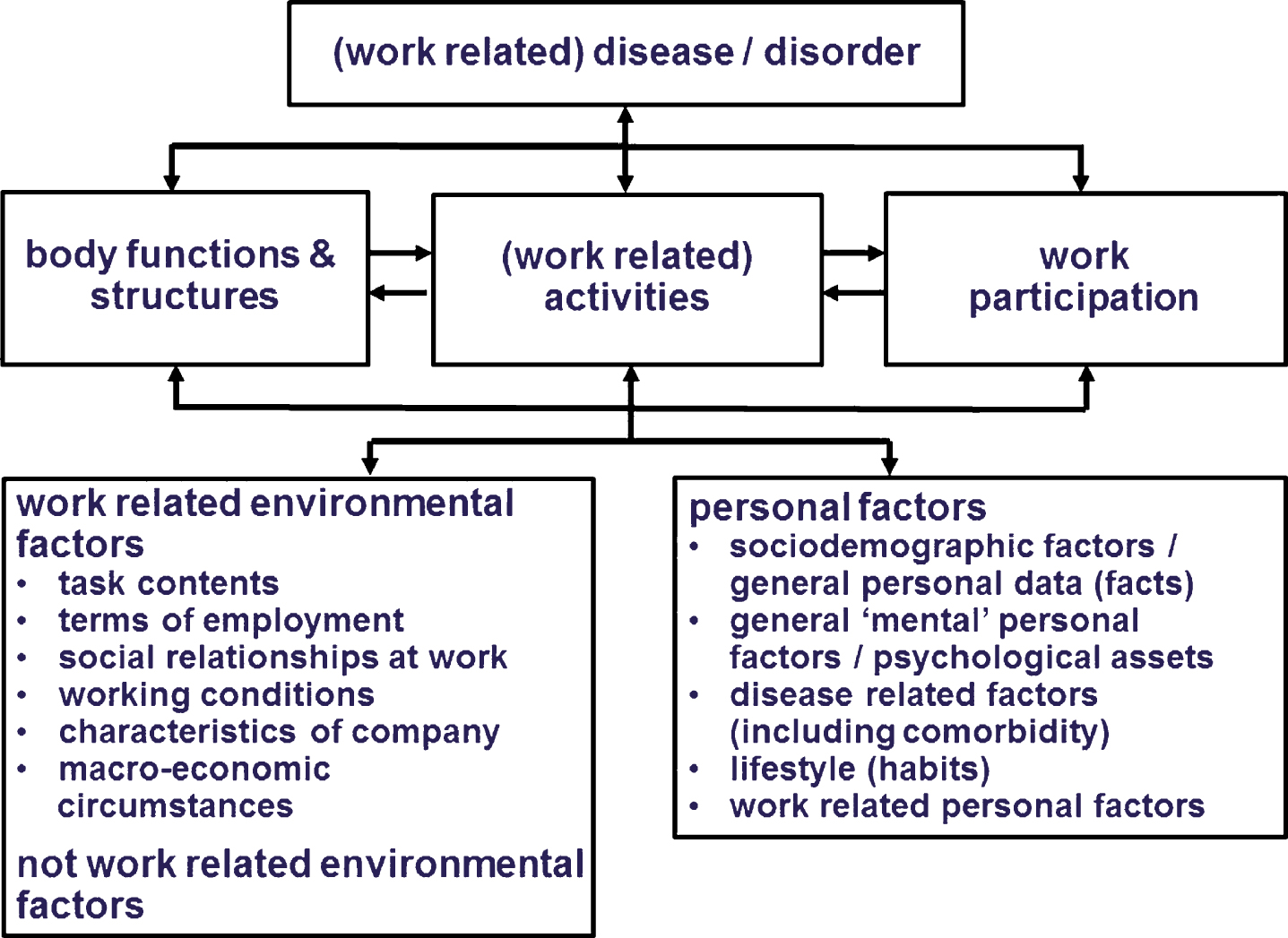
The ICF, published in 2001, was the WHO’s response to criticism of the ICIDH [5]. In addition to other changes (e.g. neutral wording), the ICF conceptual framework, expressed in the ICF diagram (Fig. 1), contains contextual factors that are subdivided into two components: environmental factors and personal factors. By adding these components, the WHO emphasised the important influence of environmental and personal factors on an individual’s functioning. Adding environmental factors ensured that “disability is no longer understood as a feature of the individual, but rather as the outcome of an interaction of the person with a health condition and the environmental factors” [7].

ICF diagram [5].
In addition to the ICF diagram, the ICF contains four classifications: body functions (codes start with a ‘b’), body structures (codes start with an ‘s’), activities and participation (codes start with a ‘d’ for domain), and environmental factors (codes start with an ‘e’). The chapters (first level) of the four classifications contain coded categories with different levels of detail (second, third and fourth levels) [5]. In total, the ICF contains more than 1400 codes; all the levels together form the ‘ICF language’. The health and health-related states of an individual may be recorded by selecting the appropriate category code(s) and then adding qualifiers, numeric codes that specify the extent or the magnitude of the functioning or disability in that category, or the extent to which an environmental factor is a facilitator or a barrier [5].
So far, the current classification of environmental factors in the ICF consists of five chapters (first level): e1) products and technology; e2) natural environment and human-made changes to environment; e3) support and relationships; e4) attitudes; and e5) services, systems and policies. These chapters only contain a limited number of categories related to the workplace. Examples on the second level are ‘e135 products and technology for employment’, ‘e330 support and relationships of people in authority’ (e.g. employers and supervisors), and ‘e590 labour and employment services, systems and policies’.
However, many items relevant to occupational health are missing (e.g. task content and terms of employment). This makes it difficult to apply the classification of environmental factors in research and education on the influence of work-related factors on work participation, return to work, productivity, physical and mental health, and quality of life [8, 9].
ICF core sets – ICF selections for a certain patient group or for a specific area of practice (e.g. vocational rehabilitation) [10, 11] – contain items from the four classifications. The importance of environmental factors is clear from the number of codes from this component that are incorporated in the different ICF core sets. Of all the codes in the comprehensive core set for vocational rehabilitation, for instance, 37% are environmental factors [10, 11]. Of the comprehensive core set for stroke, 25% of the codes are environmental factors [12] and of the comprehensive core set for low back pain, 32% of the codes are environmental factors [13].
The definition of a work-related environmental factor we use in this article is based on the ICF definition of environmental factors (see Table 1). Many classical occupational diseases have almost disappeared in Western societies due to legislation (although about 125 million people in the world are still exposed to asbestos in the workplace) [14]. However, new ones have emerged, such as stress-related occupational diseases (e.g. burnout [15], cardiovascular diseases [16]), mental health complaints (e.g. anxiety and depression [17]), complaints of the neck, arm and/or shoulder due to prolonged working in a certain posture (e.g. computer workers) [18], and the consequences of prolonged sitting [19].
Definition of contextual factors
Definition of contextual factors
Besides the negative effects the work environment can have on health and employability, it can also have positive effects: for example, by giving people opportunities for personal growth and development, by fostering positive social relationships at work, by providing optimal working conditions, and by customising the job for employees with activity limitations.
Paying attention to the positive and negative influences of work-related environmental factors is important to understand the functioning of employees, especially those with chronic conditions. Numerous studies have investigated factors that influence the work participation of employees with a chronic condition (e.g. neuromuscular disorders [20]) or who have suffered a spinal cord injury [21] or a traumatic brain injury [22]. Other studies have also reported on the effects of return to work (RTW) interventions (e.g. for people with work-related stress [23] or who have long-term absenteeism due to chronic low back pain [24]). By adapting working conditions (e.g. shifting work content, limiting the number of hours, adapting tools and equipment, and increasing autonomy), employees with chronic conditions can be given the opportunity to continue working or to successfully return to work [25].
However, work-related environmental factors not only influence the well-being and sustainable employability of vulnerable employees, but of all employees. Especially in light of the discussion about sustainable employment, a proactive approach towards keeping employees fit and motivated for work requires addressing work-related environmental factors before health or participation problems arise [26, 27]. It is therefore understandable that the ICF, including the classification of environmental factors, is increasingly used in occupational health care for monitoring the health of employees, alongside things like guidance in vocational rehabilitation [28, 29], evaluation of work ability [30, 31] and research into the usefulness of the ICF for specific groups of workers, such as musicians [32]. Unfortunately, many of the work-related environmental factors found in the literature, especially those related to creating healthy work environments to preserve employees’ long-term health, are not included in the present ICF classification. In the specific field of vocational rehabilitation, Finger et al. [33] noted the lack of work-specific ICF categories in the classification of environmental factors. Adding these and other missing factors would improve the usefulness of the ICF.
In the process of developing the ICF, the WHO decided not to include a detailed list of personal factors. No international consensus could be reached on the structure and the content of this list due to “the large social and cultural variance associated with them” [34] and the ethical concern that a list of personal factors can be misused as a ‘classification’ of the person [35]. Personal factors are represented in the ICF diagram, but the introduction to the ICF only lists some examples of possible personal factors (e.g. gender, race, age, fitness, lifestyle, habits, upbringing, coping styles, social background, education, profession, past and current experience, overall behaviour pattern, and character style) [5].
There is a lot of discussion in the literature about the position and definition of personal factors. Personal factors are perceived to be controversial as they are ‘too personal’ [36] or carry the potential risk of ‘blaming the victim’ by suggesting that a problem exists with the individual [37]. Grotkamp et al. [36] indicated that personal factors should not be used to stigmatise, label or otherwise blame a person; instead, the objective is to respect the individual’s needs and strengths. To neglect personal factors would mean accepting the ICF as an incomplete instrument [36].
Simeonsson et al. [38] made a critical examination of the construct and description of personal factors. They concluded that the personal factors component of ICF is not defined, there are conceptual and taxonomic problems, there is no explicit purpose stated for its use, and no guidelines are provided for its application [38]. These concerns were discussed during the June 2015 meeting of the Functioning and Disability Reference Group (FDRG) of the WHO. An article by Leonardi et al. [39], which can be seen as the result of the debate during the FDRG meeting and the WHO’s official response to the article by Simeonsson et al., concluded that: “Debate thus is needed also about the purposes of personal factors, their definitions and ethical use. This may result in a list of personal factors useful for a complete understanding of functioning and disability in a full biopsychosocial perspective.”
In spite of these constraints, the concept of a ‘personal factor’ is used (e.g. in research, practice, education, policy and planning) and there have been several attempts to come up with a list of personal factors [36, 40–42]. Recently, Müller and Geyh published an article in which they examined and compared suggestions from the literature towards a classification of personal factors [43]. Their main conclusions were that: “Future classification development activities in relation to personal factors should critically consider the topic domains that have been found common among the existing categorizations, should be based on an explicit conceptualization of PF, should clarify the problem of potential overlap of personal factors with other ICF components, should follow conceptual, formal, application and ethical principles of classification development according to WHO standards, and use empirical data and modern classification development methodology” [43].
Personal factors play an important role in (occupational) health care, research, policy and planning, and education, which emphasises the need for a list of personal factors to make the ICF more useful in all these fields [34]. Like environmental factors, personal factors can have a positive or negative influence on health and employability. It is important that these factors be taken into account in occupational health care and research.
Expansion of the ICF diagram
The lack of many relevant work-related environmental factors and the lack of a classification of personal factors were already mentioned in a 2004 article written by Heerkens and colleagues [9]. In that article, some of the authors of this article recommended that the classification of environmental factors be further expanded to add work-related factors and that a list or classification of personal factors be developed to make the ICF more useful for occupational health [9]. The proposed expansion was based on the Van Dijk model [44]. It was expected that this expanded diagram could bridge the gap between the terminology used by health care professionals and that used by occupational health professionals.
Aims
The aims of this discussion paper are: 1) to give an update of the need to add work-related environmental factors to the classification of environmental factors and the need to add a classification or list of personal factors to the ICF; and 2) to present an elaboration of contextual factors, consisting of a list of work-related environmental factors and a list of personal factors. Both lists are intended to make the ICF better suited for use in education, research, occupational health, and policy and planning.
This article is mainly focussed on the use of these additional factors in research, vocational rehabilitation and the assessment of work (dis)ability. The use of the ICF in (higher) education, including these additional factors, is highlighted in another article in this special issue (De Brouwer et al. [45]).
Methods
The ultimate effort of this publication is to enhance the further development of the ICF, as a classification system. All the methodological steps can therefore be related to the recently published view on classifications by Hollenweger [46]. She stated that “classifications are representations of a knowledge domain but at the same time also guide knowledge creation. They are intermediaries between our conceptual worlds and the phenomenon we encounter in our professional lives” [46].
In 2001, the WHO published the first edition of the ICF [5]. From that point onwards, the ICF diagram and the ICF language triggered further knowledge creation. The development of the expansion of the ICF diagram with the Van Dijk model [9] for the specific field of work and health is an example of an intermediary between a conceptual world and problems encountered in occupational health practice. By using the expanded ICF diagram in research and teaching from 2004 onwards, we developed a concept list of work-related environmental factors and a concept list of personal factors. Over the years, we added factors found in the literature and suggestions from researchers and (PhD) students in the field of occupation and health. Three exemplary cases of this bottom-up approach are the work of Detaille et al. [31], Minis et al. [20] and De Beer et al. [47].
In a systematic review of factors influencing work (dis)ability in employees with a chronic somatic disease, Detaille et al. [31] found common prognostic contextual factors: ‘heavy manual work’ and ‘female gender’ for work disability in all the diseases included in their study and ‘age’ (high versus low), ‘education’ (high versus low) and ‘ethnic origin’ (white versus non-white) for rheumatoid arthritis and ischaemic heart disease.
In a systematic review of factors influencing work participation in employees with a neuromuscular disease (NMD), Minis et al. [20] found 10 factors that were indicative for an association with employment status. These included three general personal factors (age, gender and education) and two work-related personal factors (type of occupation, and expressed interest in employment by patients with NMD).
De Beer et al. [47] used the expanded ICF diagram of Heerkens et al. [9] in publishing a systematic review of factors that influence the work participation of adults with developmental dyslexia. They found 314 factors (in all components of the ICF). Among the codes with the highest manifest frequency size were the work-related environmental factors. These include ‘social relationships at work’, where the attitude and support of the employer and co-workers are important, and ‘working conditions’, with factors like the availability of assistive technology and accommodations on the job. Personal factors, like disclosure and coping strategies, were also prominent [47].
As indicated, the Van Dijk model [44] was used in our development of the concept list of work-related environmental factors. In this model, work context is subdivided into task content, terms of employment, social relationships at work, and working conditions. The characteristics of the employment organisation and macro-economic circumstances are also added (see Table 2). We based the structure of the concept list of personal factors on the subdivision by Badley [34] and the results of the systematic review by Geyh et al. [40]. Personal factors are subdivided into sociodemographic factors (general personal data / facts), general ‘mental’ personal factors (psychological assets), disease-related factors, lifestyle (habits), and work-related personal factors (see Table 3).
A list of work-related environmental factors, including corresponding codes from the list of environmental factors in the ICF and inclusions and exclusions; the factors are alphabetised within each subdivision
A list of work-related environmental factors, including corresponding codes from the list of environmental factors in the ICF and inclusions and exclusions; the factors are alphabetised within each subdivision
*with respect to equipment, tools and furniture, a link can be made to ISO 9999:2016, Assistive products for persons with disability – Classification and terminology; http://www.iso.org/iso/catalogue_detail.htm?csnumber=60547.
A list of personal factors, related terms and examples (second column) and comments, including codes from the ICF (mainly codes from the classification of body functions (indicated with a ‘b’)) and inclusions and exclusions; the factors are alphabetised within each subdivision
To check for missing items in the concept lists, we performed a scoping literature review in fall 2015 to map our concept lists to the existing literature in the field of work participation in terms of the nature and characteristics of environmental and personal factors relevant to work. No systematic search was made for this discussion paper, as many reviews are already available. We focussed on literature that is complementary to the literature we used earlier, like the aforementioned articles by Badley [34], Grotkamp et al. [36], Geyh et al. [40] and Müller and Geyh [43]. According to Pham et al. [48], who investigated the phenomenon of scoping literature reviews, only 22% of scoping reviews include a quality assessment. We chose not to perform a quality assessment since we are interested in detecting the factors, not weighing their importance.
This means that the lists presented in this article are a mix of items from a bottom-up approach (factors found in the literature earlier in the process, experiences from our own research projects, and suggestions from students, other researchers, and (occupational) health professionals) and additional factors found in the current scoping literature review done to check our concept lists for missing factors.
The suggested expanded lists of work-related environmental factors (Table 2) and personal factors (Table 3) contain the items that are relevant in practice, education, policy and planning, and research in the field of occupational health. As both lists are still in development and have not yet obtained any official status, we decided to refrain from coding.
In this section, we will describe the results of the scoping literature review and the structure and content of both lists.
Findings from the scoping literature review
In her thesis, Dekkers-Sánchez composed a list of 53 contextual factors: 30 that promote return to work and 23 that hinder it [49]. Examples of environmental factors that promote RTW are ‘the degree of control over one’s working situation’ and ‘support from colleagues’; examples of personal factors that promote RTW are ‘the motivation of the sick-listed employee to RTW’ and ‘positive self-efficacy expectations’. Hindering environmental factors include ‘task contents’ and ‘problematic working environments’; hindering personal factors include ‘a history of absenteeism’ and ‘difficulty in coping’.
De Jong et al. performed a systematic review to assess issues that contribute to the quality of working life of employees with a chronic physical disease [50]. They found 73 issues, which they divided into 30 sub-themes and organised into five major themes: 1) job characteristics (e.g. job flexibility and worksite access); 2) the social structure and environment (e.g. discrimination, misunderstanding, disclosure); 3) organisational characteristics (e.g. requesting work accommodations); 4) individual work perceptions (e.g. enjoyment and evaluating work or life priorities); and 5) effect of the disease and treatment (e.g. cognitive and physical health and work ability) [50].
Lederer et al. [51] published a nice article about the diversity of conceptualisations of work (dis)ability. They developed a “concept map of work (dis)ability as a relation concept resulting from the interaction of multiple levels and dimensions”. With respect to the environment, they made a distinction between the organisational level and the societal level [51].
Other studies in the field of occupation and health have also emphasised the influence of environmental factors and personal factors. Hoefsmit et al. [52] described how environmental and personal factors support early RTW. Relevant factors were the work-related environmental factors ‘adequate cooperation between stakeholders in RTW’ and ‘the employers’ communicative skills’ and the personal factor ‘positive perception of the working situation’ (e.g. enjoyment of work).
Vooijs et al. [53] performed a systematic review of disease-generic factors associated with either work retention or RTW in people of working age with a chronic disease. Contextual factors associated with work participation were ‘work environment’ in the personal factors ‘age’, ‘gender’, ‘education’, and ‘own prediction of RTW’.
The prospective study of RTW across health conditions conducted by Brouwer et al. [54] found that ‘perceived work attitude’, ‘self-efficacy’ and ‘perceived social support’ are relevant predictors with regard to the time to RTW in all types of health conditions. However, they observed important differences in the type of factor and strengths of the relationships between physical and mental health conditions.
The ICF is increasingly important (or used) in assessment instruments: existing instruments are being linked to the ICF using the linking rules of Cieza et al. [55] and new instruments are being developed based on the ICF. An example of a new instrument is the Workplace Assessment Schedule, described by Bassi et al. [56] and based on the characteristics of the workplace. In the process of developing this new instrument, it became clear that only categories from Chapter 1 of the Environmental Factors could be expanded using a more specific standard terminology. The standard used was the ISO 9999:2011, the international classification of assistive products (e.g. safety helmets, workbenches, gloves, earmuffs). The other chapters of the classification of environmental factors were elaborated upon using the general terminology already present in the assessment tool: general workplace characteristics (workplace accessibility and work spaces) and specific workplace characteristics (task and workstation characteristics, technologies and tools for the workplace, personal protective equipment at the workplace, and persons related to the workplace) [56].
Personal factors are not included in the current ICF core sets, as there is no classification of personal factors in the ICF. However, in the preparatory studies for these core sets, personal factors were reported. In a literature search conducted by Viehoff et al. [57] as a preparatory study for the development of ICF core sets for lymphedema, 4% of the concepts found in lymphedema-specific questionnaires were personal factors (e.g. age and lifestyle). When Van der Mei et al. [58] used the linking rules of Cieza et al. [55] to analyse 10 questionnaires related to the quality of life of people with cancer, they reported similar results: 7 of the 10 scales included personal factors (e.g. coping, control, appreciation of life and feeling stigmatised) and 2– 6% of the meaningful concepts were personal factors.
The importance of personal factors for understanding functioning is emphasised by the fact that 18 of the 32 aspects of the concept of ‘positive’ health as determined by Huber [59] (describing how persons perceive their health [60]) can be linked to personal factors [61]. Of those 18 aspects, 12 were already in the concept list of personal factors and 6 were added (feelings of control, being in balance, meaningfulness, feeling good/flourishing, enjoyment, zest for life).
A very recent article by Finger et al. [33] presented the results of a secondary data analysis of the concepts from the systematic literature review, expert survey and patient focus group study of the ICF Core Set for vocational rehabilitation project. It included the 1,924 concepts that were marked as personal factors [33]. These concepts were linked to 31 second-level categories in a proposed ‘personal factors classification’ [33]. Many of the personal factors in this proposed classification [33] were already included in our concept list of personal factors (e.g. age, gender, educational background, language, life events, personal attitudes) and some are additional (e.g. personal values and needs) and were added to our list (see Table 3).
Elaboration of work-related environmental factors
The structure of the list of work-related environmental factors presented in Table 2 is presented in Fig. 2. Items which are part of task content include physical work demands (duration, intensity), psychological work demands (complexity, responsibilities, work pressure), decision latitude, and work autonomy. Terms of employment include working hours, facilities and type of contract. Social relationships at work are related to the attitude and support of employers and supervisors, colleagues and people in subordinate positions. Working conditions can be subdivided into physical aspects (vibrations, noise, air quality, radiation), biological and chemical agents, ergonomic aspects (furniture, computer screen, computer mouse), dangers, hygiene, and the availability of personal safety equipment [9]. With respect to equipment, tools and furniture, a link can be made to the ISO 9999:2016, Assistive products for persons with disability – Classification and terminology; http://www.iso.org/iso/catalogue_detail.htm?csnumber=60547.
The ICF diagram adapted for work, including a further subdivision of work-related environmental factors and personal factors.
There is much support in the literature for the importance of these work-related environmental factors in retaining a job and returning to work. Social support at work is an especially important factor [20, 62].
Other relevant work-related factors are the general characteristics of the company one is working for (e.g. company size and sector) and the societal level/macro-economic circumstances (e.g. labour and employment services and systems, legislation, financial and technological developments, and the labour market) [51] that influence the company’s position, guidelines, policy, and productivity.
Non-work-related environmental factors (e.g. the situation at home and the attitude and support of family members) can also influence work participation [52], but these factors are not the focus of this article and are not included in Table 2 (many of them are already covered by the present classification of environmental factors of the ICF).
The topics described by researchers including Badley [34], Geyh et al. [40], Müller and Geyh [43], and Grotkamp et al. [36], the results of our recent scoping literature review and our earlier work on the subdivision of personal factors [41] have resulted in the categorisation of personal factors as presented in Table 3 and summarised in Fig. 2.
Sociodemographic factors/general personal data (facts) are included in all the categorisations we investigated. Geyh et al. described these factors as ‘facts about the individual’s position in the physical, social, and temporal context’ [40]. Badley described them as a part of ‘scene-setting personal factors’ (together with body functions and structures) [34]. As in Geyh et al. [40], we made a subdivision of sociodemographic factors, position in immediate social and physical context, and personal history and biography.
The general mental personal factors / psychological assets category corresponds with part II and some of part III from Geyh et al. [42]: respectively experience: content of the individual’s concurrent experience, including contextual and situation-specific internal reactions; characterized by ‘aboutness’, and patterns: abstract concepts describing generalized, context-independent, cross-situational, recurrent, and persistent patterns in the person’s experience and behaviour. The potential overlap with other ICF components, as mentioned by Müller and Geyh [43], is especially relevant here. The overlap is mainly with chapter 1 ‘mental functions’ of the classification of body functions. There are several categories in this chapter, such as b126 ‘temperament and personality functions’ (including classes like b1260 extraversion and b1265 optimism), which could be general ‘mental’ personal factors. Since they are covered in the Classification of Functions, it was decided to leave them out of the list presented in Table 3. Since quality of life is defined as “the perception of individuals of their position in life, in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” [63], quality of life is included in this category.
The disease-related factors (including comorbidity) category includes all those items which are not part of the ‘main’ disease / disorder’, but are relevant to the individual’s functioning. In addition to comorbidity, examples include illness perceptions and beliefs and compliance with therapy.
Lifestyle (habits) can be seen as a risk factor for occupational health, but good habits can have a positive influence on (occupational) health. In the subdivision made by Geyh et al. [40], they are included in part III patterns: abstract concepts describing generalized, context-independent, cross-situational, recurrent, and persistent patterns in the person’s experience and behaviour. Lifestyle includes movement habits, use of alcohol and drugs, and dietary habits.
Work-related personal factors include items such as profession, the importance/meaning of work for the individual and work experience.
Many studies have stressed the importance of personal factors for health and employment [20–22, 64].
ICF ontology
The ICF, like most other classifications, was not developed based on formal principles and methods, but is the product of consensus [65]. The words used in the ICF are close to natural language terms, which are sometimes clear but often ambiguous (e.g. related to cultural background). This ambiguity is a problem when using the ICF, especially when these terms are used in computer programs (including electronic health care records). An ontology for the ICF (a formal representation of its domain) could solve this problem by making it possible to compare concepts between different classifications or between classifications and terminologies (e.g. a comparison between ICF and SNOMED CT) [65].
In the discussion of ontology, the conceptualisation of environmental and personal factors will play a role: according to Wang et al., there are moderating, mediating, independent, and confounding contextual factors [66]. Although the ICF as such is ‘neutral’ – consisting of terms to describe human functioning and factors that influence human functioning – it must include all the terms necessary to describe all the factors belonging to the four types of contextual factors mentioned by Wang [66].
Although the need for an ICF ontology was (again) acknowledged during the annual meeting of the WHO in 2014 [67] and the building blocks of such an ontology are clear, it is unknown when this ontology will be available and how it will influence the next revision of the ICF. In the meantime, the lack of work-related contextual factors is increasingly pointed out in the literature [33, 56] indicating that the implementation of the ICF in the field of work and health might be hindered.
Discussion
In assessing work (dis)ability, it is important to assess the positive and negative influences of environmental and personal factors [30]. However, many relevant work-related environmental factors are missing in the present ICF and personal factors are not classified. This study established an elaboration of the contextual factors of the ICF for Occupational Health Care. It was based on two concept lists: one for work-related environmental factors and one for personal factors. We developed those lists using a bottom-up approach over the past 12 years based on literature, our own research projects, and suggestions from students, other researchers and (occupational) health professionals. We performed a scoping literature review to look for missing factors.
Although the interaction between (work) participation and environment is complex [68], as is the relationship between (work) participation and personal factors, it is expected that these lists will stimulate and facilitate the use of the ICF in the fields of occupational health and occupational health research and education. The development of the lists presented here will be an ongoing process; new items can be added when they are needed or when results of new research become available.
Further steps to expand environmental factors
A major challenge is to include the list of work-related environmental factors in the present classification of environmental factors in the next revision of the ICF. For instance, it should be discussed whether all the included work-related factors – e.g. those related to task content and term of employment – can be placed in one of the five chapters of the present classification. A new chapter may be needed for some or all of the work-related factors, but another option is to revise the classification of environmental factors as a whole, taking into account the recommendations of Müller and Geyh [43]. Although these recommendations were formulated for the development of a list of personal factors, they can be used in a revision of the classification of environmental factors as well. In the meantime – before the start of a revision process – it is possible to use the ICF update platform (user guide: https://extranet.who.int/icfrevision/help/ICF/docs/usersguide.pdf) to formulate proposals for updating the classification of environmental factors.
Although this article is focussed on work-related environmental factors, there remains a need for an in-depth analysis to discover whether non-work-related environmental factors, which can also influence work participation, are included sufficiently in the present ICF’s list of environmental factors. These include living conditions, problems in the family and problems with the availability of assistive products (e.g. for mobility).
Further steps towards developing a list or a classification of personal factors
We agree with Leonardi et al. [39] that more debate is needed about the purposes of personal factors, their definitions and ethical use. However, we expect that ultimately there will not only be a list but a classification of personal factors because – like environmental factors – personal factors are an important component of the ICF. Whether it will ultimately be a list or a classification, there is a need for a subdivision of personal factors to completely understand functioning and disability from a full biopsychosocial perspective, as Leonardi et al. [39] indicated. We hope that the discussion about the position of personal factors within the ICF and the development of a list or classification of personal factors will continue and that this article will contribute to that discussion.
Müller and Geyh’s recommendations can be used to indicate possible further steps in the development of a list or classification of personal factors [43]. Their first recommendation is to use the factors in the existing categorisations. Many of these factors are already included in the list of personal factors presented in Table 3.
The second and third recommendations – to clarify the problem of potential overlap of personal factors with other ICF components and to follow conceptual, formal, application and ethical principles of classification development according to WHO standards – are related to the development of an ICF ontology. As discussed above, this question can be resolved during the development of an ICF ontology, including a thorough analysis of the definitions of the key concepts of the ICF. Only in this way can a decision be taken about matters such as the position of mental functions and personal factors; maybe some of the present ‘mental functions’ can be better included in the list of personal factors, while some of the personal factors (especially the general ‘mental’ personal factors/psychological assets) might be ‘mental functions’.
Finally, we agree with Müller and Geyh’s fourth recommendation [43]: to use empirical data and modern classification development methodology. We already did the first part by including relevant literature and comments from ICF users in the field of occupational health care.
Study limitations and strengths
We did not use any consensus meetings or other forms of consensus-building strategies in this study. However, a lot of evidence is already available and both lists are already being successfully used in research [47] and education [69]. Still, these lists have to be seen as a proposal; the items might be useful within the field of occupation and health, but more use cases are needed.
Use of the lists in the field of occupation and health
The lists of work-related environmental factors and personal factors can be used by researchers, teachers, students, occupational and insurance physicians, (allied) health care professionals, employers, employees, and policy makers. Box 1 gives several examples of the use of both lists in the field of occupation and health.
Recommendations
Based on the above arguments, we propose the following recommendations: We welcome researchers, teachers, occupational physicians, allied health care professionals, employers, employees, policy makers and other people interested in the use of the ICF in occupational health to use the lists of work-related environmental factors and personal factors and to share their experiences and make suggestions for improvement. The development of an ICF ontology with room for work-related environmental factors and personal factors has to be given priority; this will increase its applicability in other domains and make mapping with other terminologies and classifications possible. When that times comes, the adapted lists can be used in the revision of the ICF; in the meantime, the list of work-related environmental factors can be used to formulate proposals for updating the classification of environmental factors by using the ICF update platform.
Conflict of interest
None to report.