
Abstract
BACKGROUND:
Spinal symptoms of pain and stiffness on waking have been linked to sleep posture. Sleep posture is commonly classified as supine, side lying and prone. It is clinically postulated that sleeping postures with sustained end of range rotation and extension may influence pain sensitive spinal tissues. However, the lack of a valid and reliable method of assessing sleep posture, means clinicians are unable to provide corrective advice based upon evidenced based research.
OBJECTIVE:
To determine the validity and reliability of a sleep posture recording protocol in the home environment.
METHOD:
Twenty health professionals viewed a pre-recorded video recording of randomised sleep postures under natural and infrared light situations, with a variety of bed coverings, to represent the habitual environment. Sleep postures were classified into six categories including two intermediate postures (supported side lying and provocative side lying). Viewing was repeated after two days.
RESULTS:
Intra-and inter-rater reliability were excellent; Cohen’s Kappa = .93 (95% CI 0.80 to 1.0) and Fleiss Kappa = 0.83 (95% CI 0.82 to 0.84) respectively. Validity, determined as concordance between the health professionals’ classifications and the known postures, was also excellent Cohen’s Kappa = .91 (95% CI 0.77 to 1.0).
CONCLUSIONS:
Reliable and valid assessment of sleep posture, including intermediate postures, could be achieved using low cost, portable, infrared video recording equipment, under a variety of lighting conditions and a variety of bed cover situations typical of the home environment.
Keywords
Background
Daytime posture is considered a contributor to spinal symptoms [1], while sleep is generally considered a period for rest and recovery for workers [2]. It has been identified, that high quality sleep is critical for workers’ recovery [3]. However, some people wake with spinal symptoms, like pain, stiffness and paraesthesia, not present when going to sleep which impact on their sleep quality [4–6]. Self-reported sleep disturbances are associated with reduced performance and increased healthcare costs [7], increased risk of occupational injury [8], cause-specific work disability and delayed return to work [9].
It has been clinically postulated, that some sleeping postures involving sustained end range spinal rotation and or extension, may provoke pain sensitive spinal tissues [4, 10] and therefore affect quality of sleep. At present, there is no high-level evidence to support these clinical observations, possibly due to a lack of appropriate techniques to measure sleep posture. Current sleep posture measurement techniques can be divided into non-technological and technological.
Non-technological research designs have used self-report or questionnaires to measure sleep posture, however most of these have not been validated against a gold standard of measuring sleep posture [4, 12], while others have queried the reliability of self-report [13, 14]. With a small group of healthy participants [15], researchers validated their self-report questionnaire with a single infrared [IR] camera recording, using sleep posture criteria previously described [16]. They found self-report was accurate for the sleep postures of supine, side lying, and prone; however, no validity or reliability data were presented for their IR video classification system [15]. Self-report has also been studied in patient populations. Researchers explored the relationship between sleep posture (supine, side lying and prone) and primary open angle glaucoma, in which self-report was compared to continuous posture monitoring using an Embletta X10 sleep monitor [17]. In another study, researchers explored the relationship between sleep posture and OSA [13]. In the former, self-report of sleep posture was significantly associated with sleep posture [p = .03], while it was not found to be reliable in the latter, and recommendations were made to not solely rely on self-report. Self-report has not been examined for intermediate postures [18], the importance and clinical relevance of which are discussed later.
Technological assessment of sleep posture includes pressure mattress indentation [19, 20], capacitance sensing [21], thermal imaging [22], camera and videography [23, 24] and actigraphy [25]. Utility of the first three methods is limited by availability and cost. Researchers use IR light videography as part of polysomnography [23, 24], to determine sleep posture [6, 27] or to compare posture with other equipment [28]. Infrared eliminates the need for white light, which is known to interfere with sleeping, but using the IR light band in total darkness creates non-uniformities (overexposure in the centre) [29]. Furthermore, examples of IR image capture in the prior paragraph, did so in only one dimension, limiting accuracy due to variable bed covers, light reflection and shallow depth of field. Concerns in association with videography have previously been reported in regards to privacy, quality of image and data storage [28], but with modern equipment, image quality and data storage, these are no longer significant limitations. Actigraphy is inexpensive and commonly used to measure movement [25], however it does not measure posture. A systematic review identified the need for non-invasive, low cost and user friendly objective measurements of sleep, that can be deployed into non-laboratory environments [30]. While some researchers have utilised self-report and IR imaging in institutional dormitories [6, 31], we are not aware of these methods being used in home environments to measure sleep posture.
Sleep posture has been previously classified in different ways, but is most commonly classified into supine, side lying and prone[14–16]. In this three-level classification, supine is where the chest faces the roof, prone is when the chest faces the floor, and all other postures were considered side lying. As a result, side lying is the most commonly classified sleep posture in adults [15, 32]. However, there are several variations contained within the classification of side lying [33–35], termed intermediate postures. Prior researchers scored sleep posture images, obtained from a single IR video camera of healthy participants in a sleep laboratory and noted that intermediate side lying postures occurred. Their approach was to sub-classify these side lying postures based upon pelvic orientation [26]. However, no reliability or validity data for the manual scoring of video images were provided.
Another method used to sub-classify side lying sleep postures, is based on plausible spinal tissue load. When considering whether a sleep posture could potentially provoke night or waking symptoms, it is important to know whether the side lying posture involves end range rotation or extension, as these are known to increase compression and torsion loads and potentially sensitise spinal tissues [23]. For this reason, prior authors sub-classified side lying into two intermediate postures, supportive side lying (SSL) and provocative side lying (PSL) [36]. The authors used a protocol with dual IR video cameras to capture images in two different viewing planes, when assessing sleep posture in the home environment. They defined SSL as side lying with the top thigh resting on the lower thigh, knee or tibia. In this posture, the centre of gravity is high but spinal rotation and extension are minimal. From the SSL posture, if additional flexion of the top thigh occurred, it would result in the top knee lowering to the mattress, inducing pelvic and lumbar rotation and increased lumbar extension [18]. This sleep posture was called provocative side lying. If the lower shoulder is also retracted, spinal rotation progresses into the cervical spine, placing several spinal segments into end range positions. In this study, the authors found that the intra-rater reliability assessment of sleep posture (supine, supported side lying, provocative side lying and prone) was high (ICC > .91) [36], however inter-rater reliability and validity of the sleep postures were not assessed. Therefore, the aim of this research was to determine the reliability and validity of sleep posture assessment, including intermediate postures, using the recording protocol of Cary et al. [36] in a home environment, under varying light and bed cover conditions.
Methods
Ethics approval of this research was granted by the Curtin University Human Research Ethics Committee, reference PT0169 and all participants provided written informed consent.
Sleep posture and sleep conditions
The sleep postures for this study were defined as follows and illustrated in Fig. 1.

Sleep Posture Classification. Historically sleep postures have been classified into four groups, supine, prone, and side lying. Adults spend the greatest period of time sleeping in side lying, however there is a wide variety of side lying postures that involve varying degrees of spine rotation and extension. It is anecdotally acknowledged that sleep positions involving spinal rotation and extension, increase spinal tissue load and contribute to waking spinal symptoms. Therefore, for clinical utility, it would be of benefit to sub-classify the broader side lying posture into specific intermediate postures, based upon the associated biomechanical load. For this reason, we identified the posture of supported side lying [SSL] in which there is minimal spinal rotation or extension and provocative side lying [PSL] in which there is a combination of spine rotation and extension.
Supine – head rotated left, right or neutral, shoulder blades on the bed and legs either straight, bent or a combination
Supported side lying (SSL) – an intermediate sleep posture in which the head is rotated left, right or neutral, with the top thigh resting on or behind the bottom thigh
Provocative side lying (PSL) – an intermediate sleep posture in which the head is rotated left, right or neutral, with the top thigh forward of the bottom thigh
Prone – head rotated left, right or neutral, chest facing the floor and both legs straight.
To examine the reliability and validity of using this method to assess sleep posture, the six sleep postures were video recorded under six different sleep conditions.
The six sleep postures were: Supine SSL left SSL right PSL left PSL right Prone
The six sleep conditions were: Natural light without bedcovers Natural light with a sheet Natural light with a sheet and duvet IR without bedcovers IR with a sheet IR with a sheet and duvet
Video images of the six sleeping postures were captured simultaneously in two visual planes, using cameras at the foot end of bed and overhead. The same model demonstrated each sleep posture and all video was captured in the model’s bedroom (see Fig. 2).
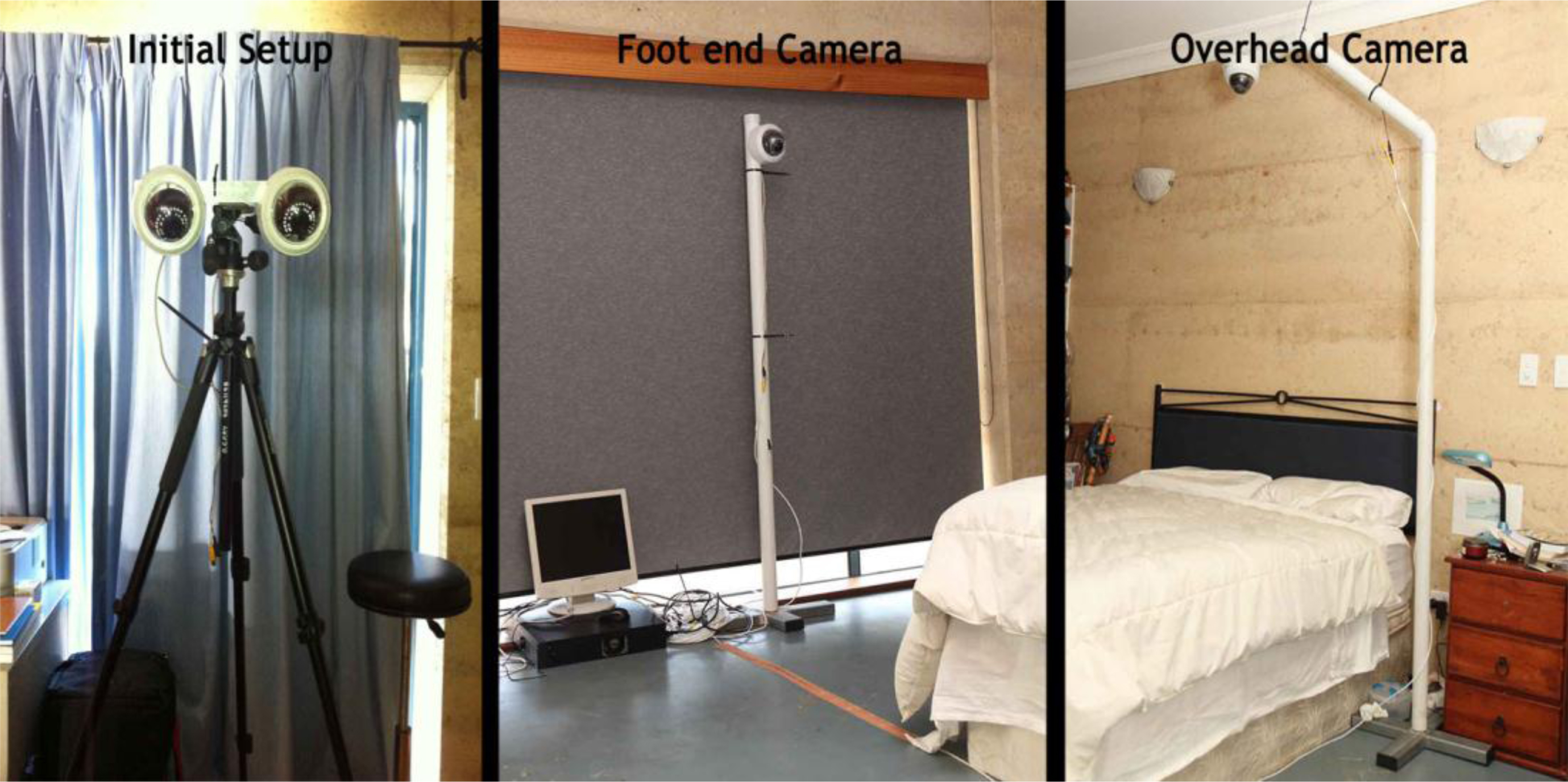
Camera Setup. Sleep imaging initially was provided with hand drawings, then photographs and currently using video captured infrared images. The most common current setting is in a sleep research laboratory associated with polysomnography, in which video footage is obtained from one viewing angle, usually the foot end of the bed. Determining the positioning of a three-dimensional object like the leg, in relation to the other leg or trunk can be difficult when viewed from one angle only. For this reason, we trialled several dual camera setups. We found that having two cameras, with different viewing angles [one overhead and one at the foot end of the bed], provided good depth perception on viewing, relative ease of setup and provided backup data collection, in the advent of one camera failing.
Each of the six sleeping postures were captured for each of the six sleeping conditions (see Fig. 3).

Visual Quality and Viewing Angles. A criticism of infrared captured images has been picture quality and the subsequent inability to determine sleep posture. For this reason, we selected cameras that provided enough resolution to provide high quality images to discern sleep posture. Furthermore, because pictures have no depth perception, we chose camera alignment that assisted in the determination of relative limb and trunk placement. This picture shows the model in the supported side lying posture, covered by a sheet, from the foot end camera and the overhead camera under infrared light.
The order of the six sleep postures was randomised for each of the six sleep conditions. The sleep posture order for each sleep condition was then transcribed onto an audio recording. During videoing, the model demonstrated each sleep posture based upon the audio recording. Each of the six sleep postures was maintained for 10 seconds and on completion of the sleep posture sequence for that sleep condition (60 seconds of recording), the model returned to supine and placed their hands-on their head for 10 seconds to demonstrate the end of the sleep posture sequence for that sleep condition. This procedure was repeated for the five other sleep conditions. Consent for the publication of this study and any additional related information was provided by the model involved in this study.
The recorded video was then imported into video editing software where a short training section was added. This consisted of a picture of each of the sleep postures, with superimposed explanatory text describing the key feature of the sleep posture (supine, SSL, PSL and prone) (see Fig. 4). Total video time was nearly ten minutes, including the training section. The video was uploaded to YouTube and 20 health care professionals were recruited by personal invitation to participate using personalized links. Informed consent was sought and granted by each health care professional. The professionals viewed the video on two separate occasions, with at least a two-day interval between viewings. After each video viewing, the professionals were asked to identify each of the 36 sleep postures as supine, SSL (right and left were combined), PSL (right and left were combined) or prone and email their recording sheet to the researcher.
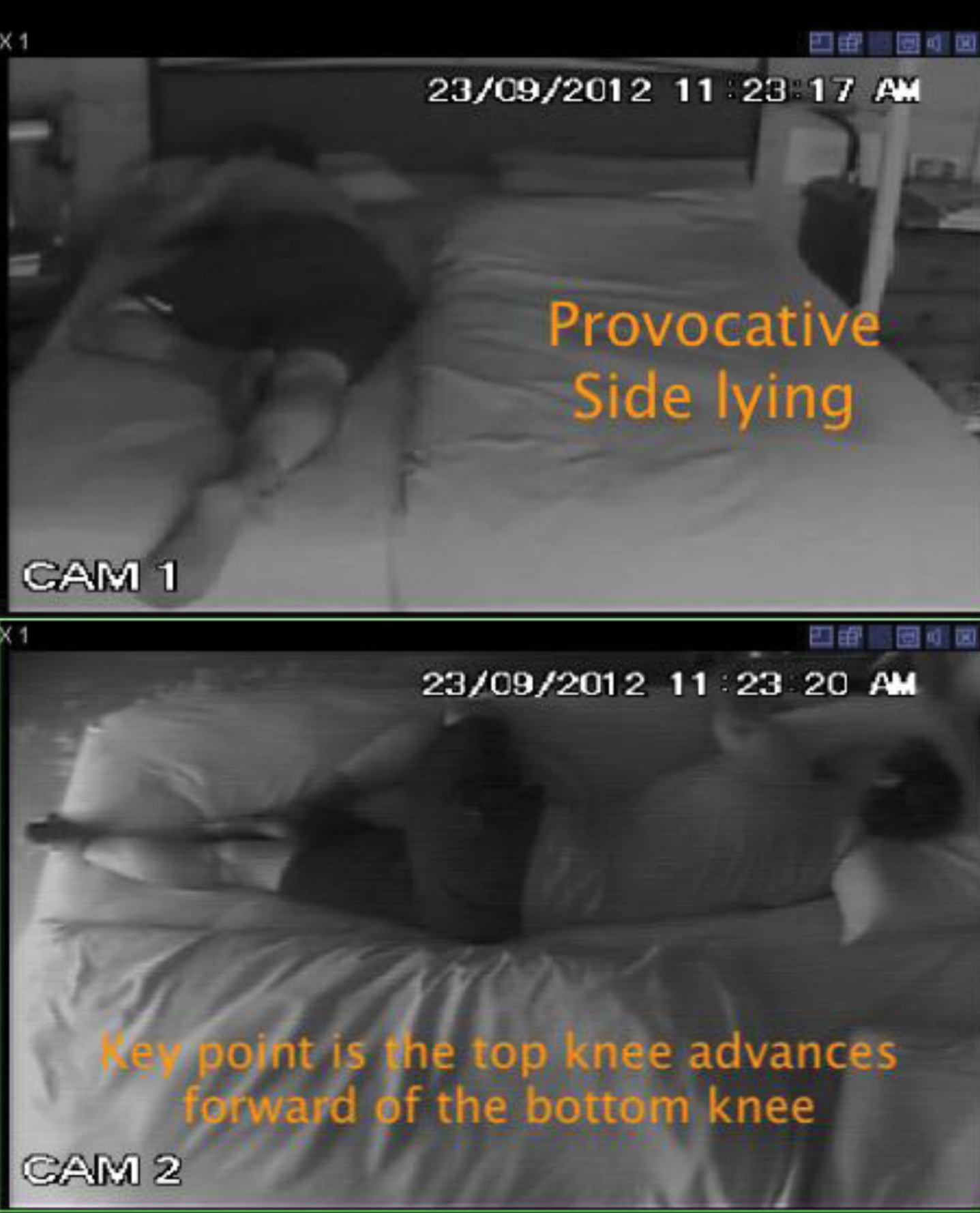
Screen-shot of Video’s Training Section. In the Training section of the video, screen shots of each sleep posture were included, highlighting to raters how to determine each of the different sleep postures. Figure 4. demonstrates the provocative side lying sleep posture, under the condition of natural light and no bed covers.
Inter-rater reliability was determined using Fleiss Kappa comparing the concordance of classifications made by the 20 health professionals during their first viewing of the recorded postures under different lighting and bed conditions. Intra-rater reliability was analysed using Cohen’s Kappa, comparing the classifications made by each professional during their first and second viewings of the recorded postures. Validity was determined using Cohen’s Kappa comparing the classification of each of the 20 professionals during their first viewing of the video against the known posture of the model.
Results
Twenty health professionals (18 physiotherapists, 2 chiropractors; 12 female) with two to 42 years of clinical experience (mean 16.7, SD 12.4), viewed the YouTube recording twice.
Inter- and intra-rater reliability were excellent. Cohen’s Kappa for intra-rater reliability was .93 (95% CI = .80 to 1.0) with a value of 1.0 for 25% of the health professionals and Fleiss Kappa for inter-rater reliability was 0.83 (95% CI = .82 to.84).
Concordance between the health professionals’ classification and the known posture was excellent, Cohen’s Kappa was .91 (95% CI = .77 to 1.0).
Discussion
This study is unique, in that it demonstrates excellent levels of validity and reliability using dual IR cameras to assess sleep posture, including intermediate postures, under a variety of light and bedding situations, as to be normally encountered in a home environment, while enabling recordings over long periods of time [36].
Reliability and validity results compared favourably with others that have measured sleep posture. In a temperature controlled laboratory using photography, prior researchers used a four dimension classification system of sleep posture and reported an inter-tester reliability of over .80 when assessing the basic sleep postures of supine, prone and side lying, but no report on intra-tester reliability or validity [33]. In a sleep laboratory environment, researchers developed an algorithm that classified sleep posture into supine, side lying and prone, based upon mattress surface indentation technology. They reported sensitivity values of 90% for supine and side lying, and 83.6% for prone, using a single IR camera video recording. However, no data were presented for the reliability or validity of using a single camera image as the gold standard [18]. The participating professionals in this study, received only minimal training in sleep posture observation and analysis via videography, and it is likely that accuracy would improve with training, experience and feedback.
Commonly, sleep laboratories use only a foot end camera, and being temperature controlled, keep the environment warm enough that participants only sleep with a light sheet. This makes visual posture assessment significantly easier. Utilisation of dual cameras in this study, was an important element to enable an accurate degree of posture visualization, minimise image over exposure and ensure collection of sufficient data in the home sleep environment. Occasional interference by pets and children and camera failure, highlighted the importance of data collection from separate sources. While more cameras could be beneficial, it would become physically problematic and potentially intimidating in most modern bedrooms.
Accurately measuring a worker’s sleep posture in the home environment, is potentially beneficial because it enables the examination of relationships between sleep posture and spinal symptoms [37]. It also has potential clinical use in managing worker’s comorbidities, such as spinal stenosis [38], obstructive sleep apnoea [39], glaucoma [17], severe peptic oesophagitis [40], acute painful disease and post-surgery or pressure relief positioning e.g. hip or spinal surgery [41]. Finally, neck and back pain are the leading cause of musculoskeletal disability in most countries and most age groups [42]. Improving worker’s self-reported sleep quality (initiation and maintenance of sleep) could reduce susceptibility to episodes and severity of neck and back pain [43, 44], risk of occupational injury [8], and cause-specific work disability and delayed return to work [9].
In summary, this study demonstrates that health professionals with varying levels of clinical experience, can reliably and accurately classify sleep postures, including intermediate postures, under a variety of light and bedding conditions. Participants in this research, received minimal training to observe and analyse sleep posture via videography, and it is possible that accuracy could improve with training, experience and feedback. In light of the overall, excellent level of intra-rater and inter-rater reliability of assessing sleep posture, including intermediate side lying postures, this recording protocol provides a cheap and easily available method to assess sleep posture in home environments.
Study limitations
The model used for the video of this study was sleeping alone. While in sleep centre-based research, this is also the common situation, in many home environments, sleeping with a partner is common and this may influence the accuracy of assessing sleep posture.
Conclusion
The described method, utilising inexpensive IR technology to collect visual data in two planes, provides clinicians with an unobtrusive and portable method of measuring sleep posture, that can be set up with minimal technology skills. This protocol is reliable and valid under a variety of light sources and bed coverings commonly found in a home environment. Further, it has demonstrated that health professionals with varying levels of clinical experience can accurately interpret the results. This protocol now provides the opportunity for sleep posture assessment to be performed in a client’s home environment and not a sleep laboratory, with the potential to identify relationships between sleep postures, spinal symptoms and other medical conditions.
List of abbreviations
IR: Infra-red, SSL: Supported side lying, PSL: Provocative side lying
Conflict of interest
The authors declare that they have no competing interests.
Funding
The author would like to acknowledge the contribution of an Australian Government Research Training Program Scholarship in supporting this research