
Abstract
BACKGROUND:
Laptop computers are used in various places and situations. The number of laptop users experiencing musculoskeletal disorders (MSDs) has increased drastically due to, in part, inappropriate workstations.
OBJECTIVE:
To investigate the neck and shoulder postures, and muscle activity relative to perceived pain when using the laptop at a low-height table, sofa, and bed.
METHODS:
Twenty male participants aged 18–25 years were randomly assigned to perform laptop computer operation at 3 workstations for 10 minutes during which neck and shoulder angles, muscle activity, and pain were recorded by using an Electrogoniometer, Electromyography (EMG), and visual analog scale (VAS), respectively.
RESULTS:
Neck flexions when working at the sofa (18.6°±12.2°) and bed (17.2°±10.5°) were significantly (p < 0.05) greater than that at the low-height table (7.8°±6.5°). However, shoulder flexion when working at the low-height table (28.2°±13.0°) was significantly (p < 0.05) greater than that at the sofa (13.8°±8.6°) and bed (10.91°±7.8°). Working at the low-height table caused the shoulder flexor muscle activity to be significantly (p < 0.05) higher than working at the sofa and bed. Neck pain was reported during laptop computer use at the sofa and bed, and upper back pain when working at the low-height table.
CONCLUSIONS:
High neck flexion and pain were found while working at sofa and bed, whereas high muscle activity at shoulder and upper back pain were found while working at the low-height table.
Introduction
The university student is increasingly using laptops in all aspects of their life. In the USA, around 90.8% of students living on the campus own a laptop computer [1]. In Australia, the mean weekly self-reported use of laptops among school students ranged from 16.9 hours to a maximum of 80 hours [2]. In the UK, it was reported that students in a university spent 5 hours per day on laptop use, of which around 36% involved academic activities [3].
University students reported musculoskeletal discomfort resulting from laptop computer use in various areas of the body including the neck, upper back, shoulder, elbow and wrist [4–10]. Interestingly, undergraduate students reported that the pain caused by computer use disturbed their functional limitation, hindered academic or extracurricular performance and some took medication and visited a physician [6].
The portable convenience of the laptop computer has led to its wide use among university students particularly in non-desk settings at home and/or dormitories which can involve a variety of postures. It was found that some university students used laptop computers in non-desk setting situations at the table, and on the bed and floor [10] and high school students used tablet PCs on the bed and on the floor [11]. Joint angle during laptop use in the prone posture was found to be different when seated at a couch with feet on the floor and on an ottoman. In addition, in the prone posture the neck was extended, the shoulder, elbow and wrist were in the non-neutral position. Discomfort at the neck region was greater than in the seated posture [12]. However, the pain and muscle activity of the head, neck and shoulder during laptop use outside of the office setting has not been yet assessed quantitatively. The objective of the current study was to evaluate neck and shoulder posture, electromyography (EMG) and discomfort among university students aged 18–25 years during laptop use in the non-desk settings of the three different workstations of low-height table, sofa and bed undertaking tasks of transferring information from the internet to Microsoft Word.
Methods
Participants
Twenty males with right hand dominance aged 18–25 years of age were recruited into the current study. The local university community was an area for the recruitment of a convenience sample. They use their laptop at least 2 days per week and/or 2 hours per day. Exclusion criteria consisted of current neck and shoulder pain, history of musculoskeletal disorder, eye problems, and medication and relaxant at least seven days before the study. The study was approved by the Human Research Ethics Committee of Faculty of Physical Therapy of Srinakharinwirot University.
Equipment and data gathering
EMG
Surface electrodes were located on the right side of the cervical erector spinae, anterior deltoid, upper trapezius and middle trapezius. Skin was cleaned before applying the surface electrode (Fig. 1). Isometric MVEs (maximum voluntary exertion) of four muscles for normalization of sEMG were collected [13]. Raw electromyographic signals were gathered at 1000 Hz via a four channel AMT-8 EMG cable telemetry system with analogue differential amplifiers (Frequency response: 10–1000 Hz). The Smoothing process was performed with a band-pass filtered at 20 to 500 Hz and RMS-smoothed with a 30-millisecond time constant. The last 2 minutes of each trial were gathered and the average EMG was extracted for statistical analysis.

Electromyography and Electrogoniometer measurement.
An electrogoniometer (Biometrics, Cwmfelinfach, Gwent, United Kingdom) was used to measure the range of motion of neck flexion, shoulder elevation and flexion. It was applied on the skin with double-sided adhesive tape. For neck flexion, an end plate was firmly attached to the skin at the cervical spine and the other end plate was attached at the upper thoracic spine. For shoulder flexion, an end plate was attached on top of the shoulder with the other end plate placed on the middle part of the deltoid muscle. For shoulder elevation, one end plate was attached on the scapular at the level of the root of spine with the other endplate being attached horizontally on the mid part of the upper trunk. Calibration was performed before gathering data (Fig. 1). The electro-goniometer was attached by the same researcher.
Body discomfort chart and visual analogue scale
Location of discomfort and severity of pain were recorded with a modified body discomfort chart and visual analog scale (VAS) [14]. VAS is frequently evaluated as perception of pain and discomfort in a clinical and research setting. The left end of the line is no pain with the other end being extreme pain with a score from 0 to 10 respectively. Participants marked their level of discomfort on the 10-centimeter horizontal line after completing work on the laptop in each workstation. Pain was reported for a number of pain regions, the average pain intensity of those regions and average overall pain intensity.
Experimental protocol
Workstations
Neck and shoulder postures were collected during laptop computer use at sofa, bed and low-height table conditions (Fig. 2). The order of postures was randomized. Laptop use at sofa involved sitting on the couch with feet on the floor. The participant sat against the pillow with the laptop placed on their lap. Laptop use on the bed involved sitting on a bed with the knees straight. The participant leaned backwards against the wall and pillow with the laptop placed on their lap. Laptop use at a low-height table involved sitting cross-legged on the floor with the back straight and laptop placed on a low-height table. The participant adjusted the location of the laptop and tilted the screen as deemed appropriate by themselves.
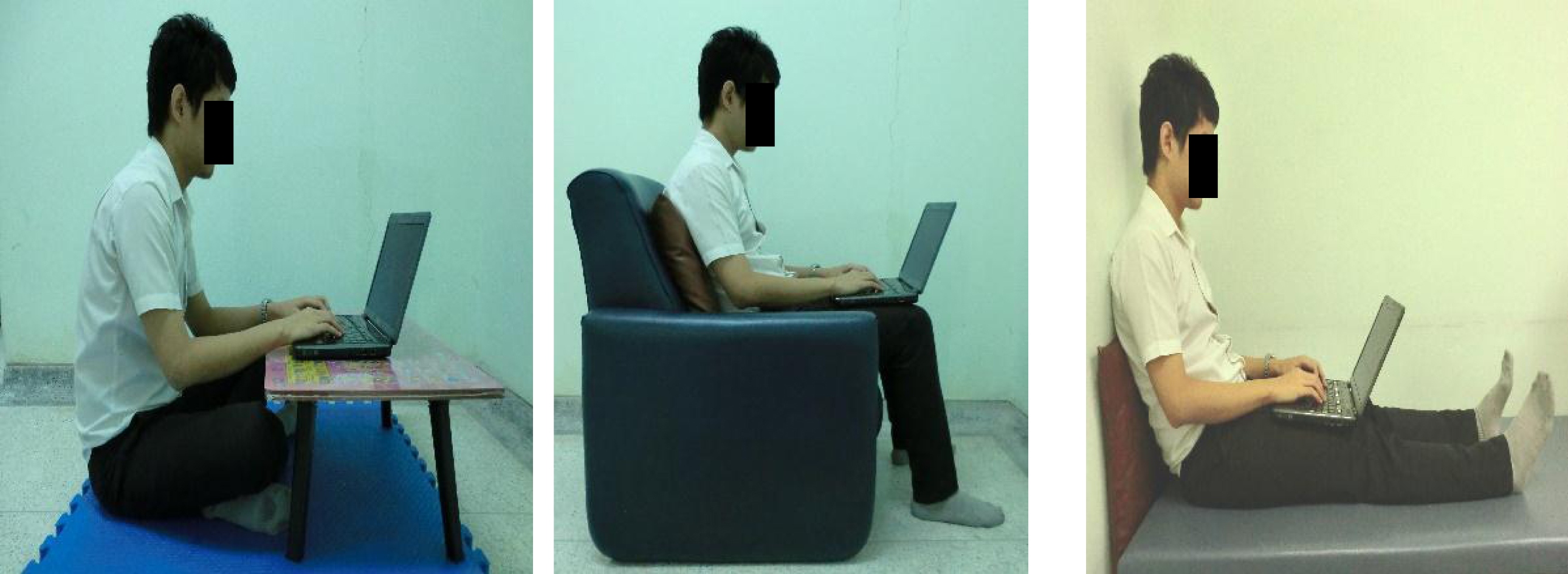
Photographs of a participant working on a laptop on a low-height table, sofa, and bed.
Participants performed two tasks which involved searching for information on the website and typing it on the software program Microsoft Word 2007 (Microsoft Windows XP operating system) to meet a required word count during 10 minutes. In this study, participants worked on a laptop (14 inches’ screen size) and a mouse which was positioned individually. EMG and posture were recorded in the final 2 minutes of each workstation.
Procedures
A consent form was supplied to each participant. Personal information of weight, height, body height was recorded. The order of performing on the three workstations was randomized. The tasks on the laptops for the different positions were explained to the participant. MEVs of four muscles on the right side of cervical erector spinae, anterior deltoid, upper trapezius, and middle trapezius were measured and a break of 20 minutes was taken before data collection was commenced. A break of ten minutes was included before the ten-minute typing task on each workstation. Body Discomfort Chart and visual analog scale were marked immediately after performing on each workstation.
Statistical analysis
Analysis of variance (ANOVA - SPSS for Windows® version 20, SPSS Inc., Chicago, IL, USA) was used to evaluate the difference of the mean of different posture and muscle activity for the different three workstations. A p-value of 0.05 was defined for the statistically significant difference. The number of regions were discomfort was experienced were counted. The average and overall severity of pain were calculated for mean and standard deviation.
Results
Participants
Twenty males were included in this study with the age range of 18–25 years. The body mass index was in the range of 18–25.6 kg/m2 (Mean±SD = 21.6±2.16 kg/m2)
Joint range of motion during laptop use at sofa, bed and low-height table
The angle of neck flexion during computer use at low-height table (Mean±SD = 7.8°±6.5°) was significantly lower than that on the sofa (Mean±SD = 18.6°±12.3°) and bed (Mean±SD =17.3°±10.5°) at a p value of 0.05 (Table 1).
Mean and standard deviation of joint range of motion during laptop use on a low-height table, sofa and bed (n = 20)
Mean and standard deviation of joint range of motion during laptop use on a low-height table, sofa and bed (n = 20)
P-value from ANOVA.
The angle of shoulder flexion in computer use at low-height table (Mean±SD = 28.3°±13.0°) was higher than on the sofa (Mean±SD = 13.8°±8.6°) and bed (Mean±SD = 10.9°±7.8°) at a p-value of 0.05. Shoulder elevation angle during laptop use at low-height table (Mean±SD = 4.2°±3.9°) was significantly higher than that on the bed (Mean±SD = 1°±0.8°) at a p-value of 0.05.
There was no significant difference between right and left neck lateral flexion during the three work stations.
The muscle activity of anterior deltoid at low-height table (1.68%) was significantly higher than that on the sofa (0.90%) and bed (0.60%). However, muscle activity of this muscle did not differ significantly between working on the sofa and bed (Table 2).
Muscle activity during laptop use on a low-height table, sofa and bed (n = 20)
Muscle activity during laptop use on a low-height table, sofa and bed (n = 20)
P-value from ANOVA, *only low-height table versus sofa, low-height table versus bed = p < 0.05.
Even though there was no significant difference in the muscle activity of the cervical erector spine, upper trapezius, and middle trapezius for the three workstations, the EMG of upper trapezius worked at the low-height table tended to be higher than working on the sofa and bed (Table 2).
Participants using laptops reported the highest percentage of discomfort (95%) on the low-height table, while it was 80% and 70% for the bed and sofa respectively (Table 3). During computer use at the low-height table, 55% of participants reported pain at the upper back region and 50% reported pain at the shoulder region. On the sofa, 60% and 40% of participants reported discomfort at the neck and shoulder respectively.
Body discomfort during laptop use on a low-height table, sofa and bed (n = 20)
Body discomfort during laptop use on a low-height table, sofa and bed (n = 20)
p-value from ANOVA.
The results revealed no significant difference in the severity of pain during computer use at the three workstations (Table 3).
The aim of the present study was to evaluate the pain, muscle activity and posture of neck, upper trunk and shoulder during laptop use in the non-desk settings of sofa, bed and low-height table. Overall, the results showed that non-desk usage of a laptop at the different workstations had a variety of effects on discomfort, posture and muscle activity. Seventy to ninety-five percent of participants reported discomfort in many parts of their body after laptop use for 10 minutes.
The findings of the current study were similar to previous studies which found that a computer screen lower than eye level led to a flexed neck posture [15–19]. In the present study, during laptop use, users were these postures with laptop being used on the sofa (18.6°±12.3°) and bed (17.3°±10.5°). This was significantly higher neck flexion than that at the low-height table (7.8°±6.5°). The angle of neck flexion on sofa and bed in the current study was close to the angle of neck during work on the laptop on the lap in the study of Maffet et al (2002) [20] (median value = 23°). The laptop screen during use on the sofa and bed was lower than that as the head mass fell in front of the center of the gravity of the cervical spine, therefore, passive structures including ligaments and joint capsules were stretched leading to discomfort. Unsurprisingly, a higher number of participants reported neck pain after laptop use on the sofa and bed compared with the low-height table.
Interestingly, the angle of neck flexion during laptop use on sofa and bed in the current study were close to the average of the neck flexion relaxation phenomenon (23°±4.5°) in the study of Pialasse et al (2009) [21] which leads to the decreased activity of the neck extensor muscles. The muscle activity of the neck extensor in the current study was 3.77% ±2.82% (sofa) and 4.12% ±2.62% (bed). A higher number of participants reported neck pain for laptop use on the sofa (n = 12) and bed (n = 11) compared with the low-height table (n = 9).
Shoulder flexion angle of laptop use at low-height table was significantly greater (28.2°±13.0°) than on the sofa (13.8°±8.6°) and bed (10.91°±7.8°). Also, the muscle activity of the shoulder flexor was higher than that on the sofa and bed. The laptop on the low-height table was placed in front of the user, leading to a higher number of participants reporting shoulder pain after using a laptop on a low-height table (n = 10) compared with the sofa (n = 8) and bed (n = 7). Shoulder flexion while working on the lap in the current study was 13.8°±8.6° (sofa) and 10.9°±7.8° (bed) which differs from the previous study of Sommerich et al (2002) [16] which found a shoulder flexion of 22° – during use on the lap. This difference may have been caused by the laptop being placed on the lap close to the body during use on the sofa and bed in the current study; however, in the study of Sommerich et al (2002) [16] an external keyboard was placed at elbow height with 90 degrees of elbow flexion and the distance of the keyboard on the support surface was adjusted by the individual.
The usage of a laptop on a low-height table is common among Asian users. Sitting cross-legged during use on a low-height table is fairly similar to sitting on a chair with the feet up with the disadvantage of no back support. Users adopted several non-neutral postures both at vertebra and shoulder. The round posture of the lumbar spine was found to cause a decrease in the lordotic curve and also an increase in the thoracic curve. Therefore, the number of participants reporting low back pain was highest when working at a low-height table, when compared with working on a sofa and bed. Furthermore, 95% of participants reported some pain in many part of their body after using a laptop on a low-height table. We would suggest that the risk of musculoskeletal disorder is higher for laptop use on a low-height table.
This is the first study to evaluate the muscle activity of the neck, upper back, and shoulder in non-desk settings of laptop use frequently experienced after office hours. It has been found that muscle activity, particularly the neck muscle, works differently as relates to the location and height of the computer. Moreover, the results of the present study can also be applied to long-term laptop usage with 10 minutes in a non-desk setting.
One limitation of the study is that the participants were university students; therefore, the results of the current study are not generalizable to other groups of laptop users such as children and adults with different anthropometric characteristics from university students, which will lead to different adaptation of posture, muscular working and discomfort. In the current study, participants worked on the computer for 10 minutes but the data for muscle activity was collected in the last 2 minutes. Some participants would change their posture and thereby cause discomfort during the trial as happens in a real situation. However, in further research, discomfort should be still evaluated over a long period of time but frequent short session evaluations should be conducted to clarify when pain starts for the users in the non-desk settings of laptop use. In addition, discomfort should be evaluated in other age groups. This will be useful for the establishment of guidelines and suggestions for the user about frequent breaks, which is one of the main risks of musculoskeletal disorders.
Conclusion
Computer use at low-height table showed a higher degree of shoulder flexion and elevation compared with use on the sofa and bed. In addition, shoulder flexion was of a higher angle because the laptop was placed at a higher location. Unsurprisingly, the muscle activity of the anterior deltoid muscle at the low-height table was markedly higher when compared with computer use at other places. For these reasons, discomfort was reported as high when using the computer in the other two workstations. However, working on the sofa and bed showed higher neck flexion when compared with working on the low-height table. The computer was placed on the lap lower than the height of the low-height table, therefore, the participants had to bend their neck forward. This led to a high number of participants experiencing neck discomfort.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The funding for this research was provided by Faculty of Physical Therapy, Srinakharinwirot University. Special thanks to Assist Prof. Saitida Lapanantasin for her support.