
Abstract
BACKGROUND:
The Ottawa Paramedic Physical Ability Test (OPPAT™) is a physical employment standard for the paramedic sector. If a candidate is unsuccessful in meeting the OPPAT™ performance standard they should be provided with an appropriate accommodation, such as a strength and conditioning program, to improve performance.
OBJECTIVE:
Develop, implement and evaluate the effectiveness of a 4-week strength and conditioning program on improving OPPAT™ performance and associated fitness measures in paramedic candidates.
METHODS:
A 4-week strength and conditioning program was developed to focus on strength and power improvements. Based on initial OPPAT™ performance, participants were divided into high and low performing groups; only the low performing group received the training intervention. OPPAT™ completion times and relevant fitness measures were compared pre- to post- intervention and between groups.
RESULTS:
Over the 4-weeks, peak lower body power and grip strength did not significantly improve in the intervention group, however OPPAT™ performance improved by 10%. The control group had significantly lower OPPAT™ completion times both pre- and post-intervention (19% and 11% lower respectively), as well as greater grip strength and peak lower body power.
CONCLUSIONS:
Implementation of a targeted strength and conditioning program successfully improved OPPAT™ performance in low performing candidates.
Introduction
Paramedics are integral within the health care system as they provide pre-hospital patient care in emergencies. Physically demanding tasks that are essential to the occupation include lifting/lowering, loading/unloading, pushing/pulling, and carrying patients and equipment [1, 2], exposing paramedics to high loads [3]. The combination of the physical demand and exposure to heavy loads results in paramedics experiencing the highest prevalence of work-related injury by sector [4, 5] with a large portion of these injuries being documented as musculoskeletal disorders (MSD). The emergence of interventions such as powered stretchers [6–8] have helped reduce MSD rates, however, these interventions do not eliminate exposure to other physically demanding tasks. Therefore, it is of great importance that candidates have the requisite physical capabilities to meet these demands, ensuring they are able meet patients’ needs while mitigating the potential for MSDs.
It is common in public safety related professions to develop and implement a physical employment standards (PES) to screen out individuals who do not demonstrate the physical ability required to meet job specific Bona Fide Occupational Requirements (BFOR) [9]. An additional benefit of a PES is that it can also support MSD prevention [10]. For example, within the mining sector, employees who scored poorly on a PES (applied to inform job matching rather than to evaluate against BFOR) were 5.8 times more likely to develop a low back injury over a period of 1 to 6 years after the time of hiring compared to high performers [11]. In the paramedic sector, the Ottawa Paramedic Physical Ability Test (OPPAT™) has been developed as a physical employment standard to identify if candidates can meet the physical demands of paramedic work that are identified as BFOR. The test requires candidates to complete simulations of physically demanding aspects of paramedic work embedded within three circuits that mimic common emergency calls scenarios. Candidates must complete the circuits within 600 and 1020 seconds without dropping any equipment to successfully demonstrate the requisite physical ability.
OPPAT™ development continues to follow the best practice approach to establish a legally defensible PES in Canada [9]. First, a project management team was formed including representation from union and management within the Ottawa Paramedic Service. Second, the job requirements and associated physical demands of paramedic work were quantified [1, 12]. Third, the physical demands data were listed for front-line paramedics, where those paramedics rank ordered the list in terms of physical demand [12]. Based on the physical demand ranking of essential tasks, the OPPAT™ was designed as a simulation-based physical employment standard encompassing many of the most physically demanding tasks of paramedic work. Consistent with the best practice approach of developing a legally defensible PES, and to address adverse impact, there is a duty to develop appropriate accommodation for candidates who are unsuccessful on the test. Targeted strength and conditioning has been proposed as an accommodation to improve PES performance [13], and has been shown to be effective in wildland firefighters and correctional officers[14, 15].
The benefits and improvements afforded by a strength and conditioning program are dependent on the design and structure of the program. In paramedic work, there are muscular and cardiovascular demands that include lifting, carrying, pushing and pulling equipment, often loaded with the weight of a patient. By considering previous research, aspects of fitness that are associated with successful performance in essential paramedic tasks can be identified. Von Restorff [16] showed grip strength was the best predictor to determine capacity to carry a 90 kg patient. Individuals with greater grip strength have also been shown to maintain high quality chest compression in cardio pulmonary resuscitation (CPR) [17]. With respect to fatigability in a prolonged stretcher carrying task, maximum aerobic capacity (
The purpose of this project was to develop and evaluate the effectiveness of a strength and conditioning program that can be implemented as an accommodation for candidates who do not initially perform well (e.g., are not successful) on the OPPAT™. To address that purpose, three specific research questions were investigated: Are strength (measured by dominant hand grip strength), cardiovascular fitness (measured by Is a 4-week strength and conditioning program effective in improving OPPAT™ performance and relevant fitness measures among those who initially perform poorly on the OPPAT™?; and, How do fitness measures differ between high and low OPPAT™ performers before and after the exercise intervention?
Methods
Overview
Two phases of research were required to address the research questions. The first phase required a baseline fitness assessment and an evaluation of OPPAT™ performance among a sample of students enrolled in a paramedic program. The second phase included a non-randomized control trial where phase 1 participants were divided into two groups based on their OPPAT™ performance (high performers and low performers). The low performer group completed a supervised 4-week strength and conditioning program and the high performer group served as a control group. Both groups re-completed the fitness assessment and OPPAT™ following the intervention period (Fig. 1).
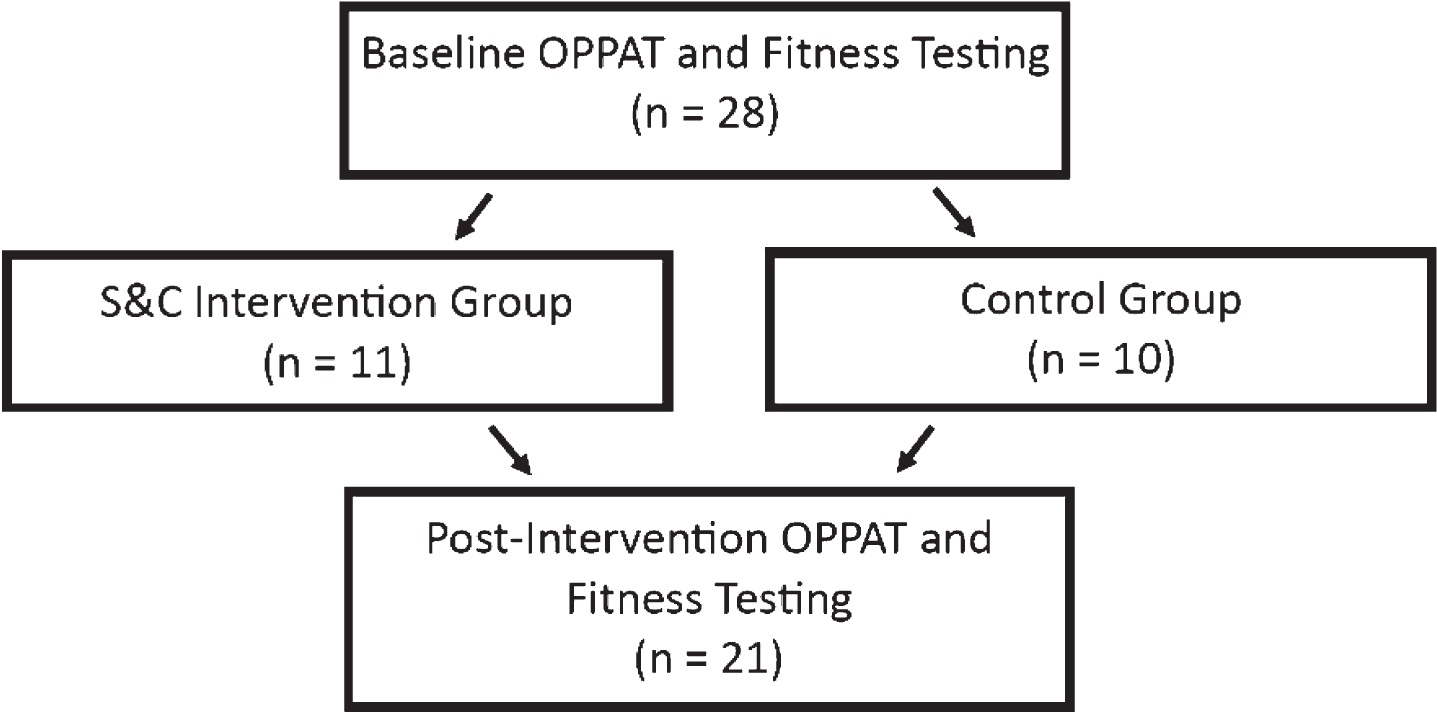
Overview of experimental protocol with number of participants indicated.
For phase 1, 28 students (14 female, 14 male; 25.0±4.7 y; 1.72±0.10 m; 80.1±15.9 kg) enrolled in a paramedic program at an Ontario college were recruited. Students enrolled in a paramedic program were selected as a participant pool as they directly represent the population that will have to successfully complete the OPPAT™ prior to being hired by a paramedic service. As part of their education, students received some background information on principles of strength and conditioning, but none of the participants received training or coaching in strength and conditioning within their formal educational training. Of those 28 participants, 10 (1 female, 9 male; 26.6±6.7 y; 1.77±0.07 m; 79.3±12.9 kg) were retained as the control group (high performers on their initial OPPAT™), and 11 (10 female, 1 male; 23.8±2.5 y; 1.65±0.06 m; 74.9±15.4 kg) formed the intervention group (low performers on their initial OPPAT™) for phase 2. Group assignment was based on OPPAT™ performance as detailed below in section 2.4.1.
Phase 1 – baseline testing
Baseline OPPAT™ testing
In participants’ first OPPAT™ session they were oriented to the OPPAT™ circuit, which included introduction to the lifting partner who assisted with lifts and carries throughout the circuit. The OPPAT™ is comprised of three sub-circuits completed in succession and loosely representing different types of paramedic call responses. OPPAT™ completion time was recorded as the performance measure. Consistent with the OPPAT™ performance standard, the test administrator could terminate the test if a participant dropped a piece of equipment or if a participant stopped in the middle of a task (i.e., during a cycle of CPR). If a test was terminated prior to completion, a time of 1050 seconds was recorded, which is greater than the standard performance cut-score of 1020 seconds. In all OPPAT™ trials participants were required to wear Canadian Standards Association approved steel toe shoes, uniform pants and belt.
Baseline fitness assessment
Participants also completed a fitness assessment battery including tests for dominant hand grip strength, peak lower body power and estimated
The modified Canadian Aerobic Fitness Test (mCAFT) step test was used as a predictive test of
Phase 2 – Strength and conditioning intervention
Strength and conditioning program
Participants from phase 1 who were willing to continue into phase 2 were dichotomized into one of two groups, a group that received supervised strength and conditioning training for 4 weeks or a control group who were asked to not make any lifestyle changes over the 4 weeks. A non-randomized approach was used to allocate participants into groups. Those with the 10 fastest OPPAT™ completion times were allocated into the control group and those with the 11 slowest OPPAT™ completion times were allocated into the intervention group. The mean OPPAT™ completion time across all participants pre-intervention was 812 seconds. The goal of the strength and conditioning program was to help improve the performance of those who initially completed the OPPAT™ in a slower time by increasing their physical ability.
Participants in the intervention group received a 4-week supervised, periodized exercise program designed to improve general fitness levels with a focus on strength and power development specific to the demands of paramedicine. The strength and conditioning program was informed by the results to research question 1, the Task Performance and Health Improvement Recommendations for Emergency Medical Service Practitioners [23] in accordance with general guidelines for exercise prescription [24], and periodization [25]. A focus on movement competency via key features of movement was also included as a high-level training objective consistent with the movement-guided strength and conditioning training employed by Frost et al. [26].
Participants attended 3, 1-hour sessions per week under the guidance, supervision and coaching of a Registered Kinesiologist. Participants began each session with a dynamic warmup followed by the completion of a full body workout including a combination of squat, hip-hinge, lunge, push, pull and carry movement patterns (Table 1). In each session participants were encouraged to select a resistance (operationalized as the weight lifted) which would require maximal effort to complete the prescribed number of repetitions. Exercises aimed to mimic primary movement patterns associated with the performance of physically demanding aspects of the OPPAT™, which in turn simulate live paramedic tasks. One example was the inclusion of the front squat instead of the back squat. Consistent with squatting down to lift a backboard or stretcher, the weight is typically anterior to the body (consistent with the position of the weight when performing a front squat) not posterior to the body (similar to a back squat).
Overview of training program. Training loads were selected so the desired number of repetitions could be achieved with a maximal effort. Exercises labeled with the same number (i.e. A1, A2) were performed in succession before completing a second set
Overview of training program. Training loads were selected so the desired number of repetitions could be achieved with a maximal effort. Exercises labeled with the same number (i.e. A1, A2) were performed in succession before completing a second set
Technique and movement competency was a program focus from week 1 to minimize unfavorable movement patterns such as spinal flexion and axial twist [26]. An emphasis on movement competency was maintained throughout the 4-week program as previous work has demonstrated that movement focused training can lead to improvements in low back and frontal plane knee motion in simulated work tasks within a firefighter population [26]. As participants progressed into weeks 2-3 the program focus was adapted to increase the resistance and movement explosiveness while continuing to maintain key movement features associated with good movement competency [26]. By the final week of the program training volume and intensity were adjusted to maximize strength development.
Following the 4-week training period participants in both groups completed the OPPAT™ and fitness assessment battery by following the same protocol as used pre- intervention.
Statistical analysis
A forward stepwise multiple regression was used to determine if dominant hand grip strength,
A two-way mixed analysis of variance (ANOVA) with a between factor of group (intervention or control) and a within factor of time (pre- vs. post- intervention) was used to detect for differences in OPPAT™ completion times and fitness measures. For the two-way ANOVA effect size was calculated as Cohen’s f where an f≥0.40 represented a large effect, 0.25≤f < 0.40 represented a medium effect, and 0.10≤f < 0.25 represented a small effect [28]. For significant effects, simple mean pairwise comparisons were used to evaluate differences in a single group pre- vs. post- intervention or between groups either pre- or post- intervention. In the simple means pairwise comparisons effect size was calculated as Cohen’s d where d≥0.80 represented a large effect, 0.50≤d < 0.80 represented a medium effect, and 0.20≤d < 0.5 represented a small effect [28]. An alpha value of α≤0.05 was used to detect for main effects. The alpha value was Bonferroni corrected for post hoc testing. All statistical analyses were conducted in SPSS (SPSS Version 22.0 for Windows, SPSS Inc., USA).
Results
Peak lower body power (β= – 0.62, p < 0.001) was the only significant predictor included in the forward stepwise multiple regression model and explained 38% of the variance of initial OPPAT™ performance (r2 = 0.38, F(1, 26) = 16.37, p < 0.001) (Fig. 2). However, a VIF of 2.48 was calculated between peak lower body power and dominant hand grip strength, indicating collinearity. A simple correlation between dominant grip strength and OPPAT™ completion time confirmed a significant association (r2 = 0.32, F(1, 26) = 12.21, p = 0.002). These results collectively suggest that the variance in OPPAT™ completion time explained by grip strength was also explained by peak lower body power.
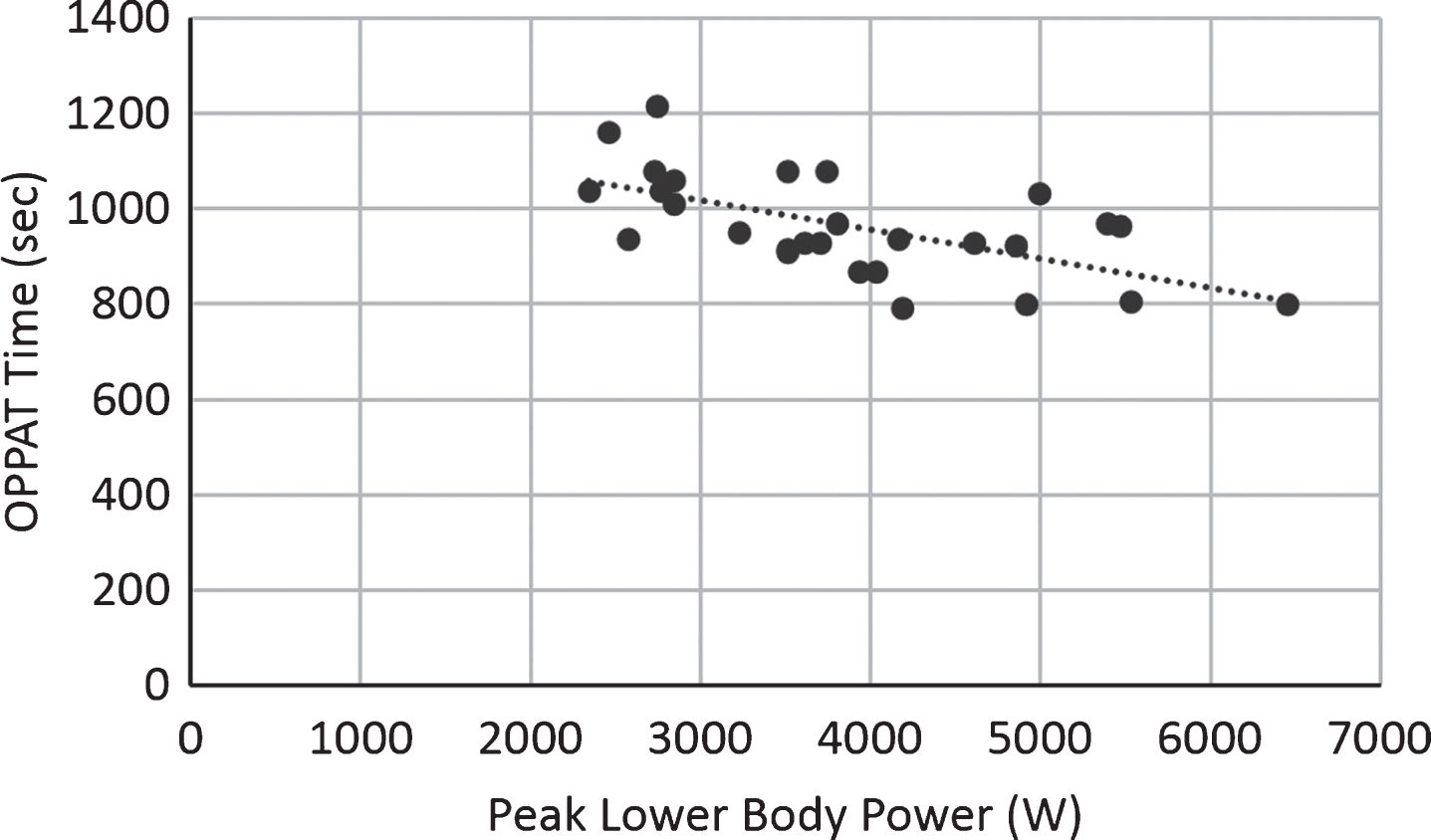
Completion time of first OPPAT™ trial as a function of peak lower body power.
There were significant main effects of time and group, as well a significant interaction effect on OPPAT™ completion time (Table 2). Simple mean pairwise comparison revealed the intervention group was significantly slower than the control group both before (p < 0.001, d = 1.65) and after the intervention (p = 0.026, d = 1.16) by 19.0% and 11.1% respectively. However, within the intervention group, OPPAT™ completion times were significantly faster post-intervention (p = 0.013, d = 0.94) (Fig. 3) which corresponded to a 9.8% reduction in completion time.
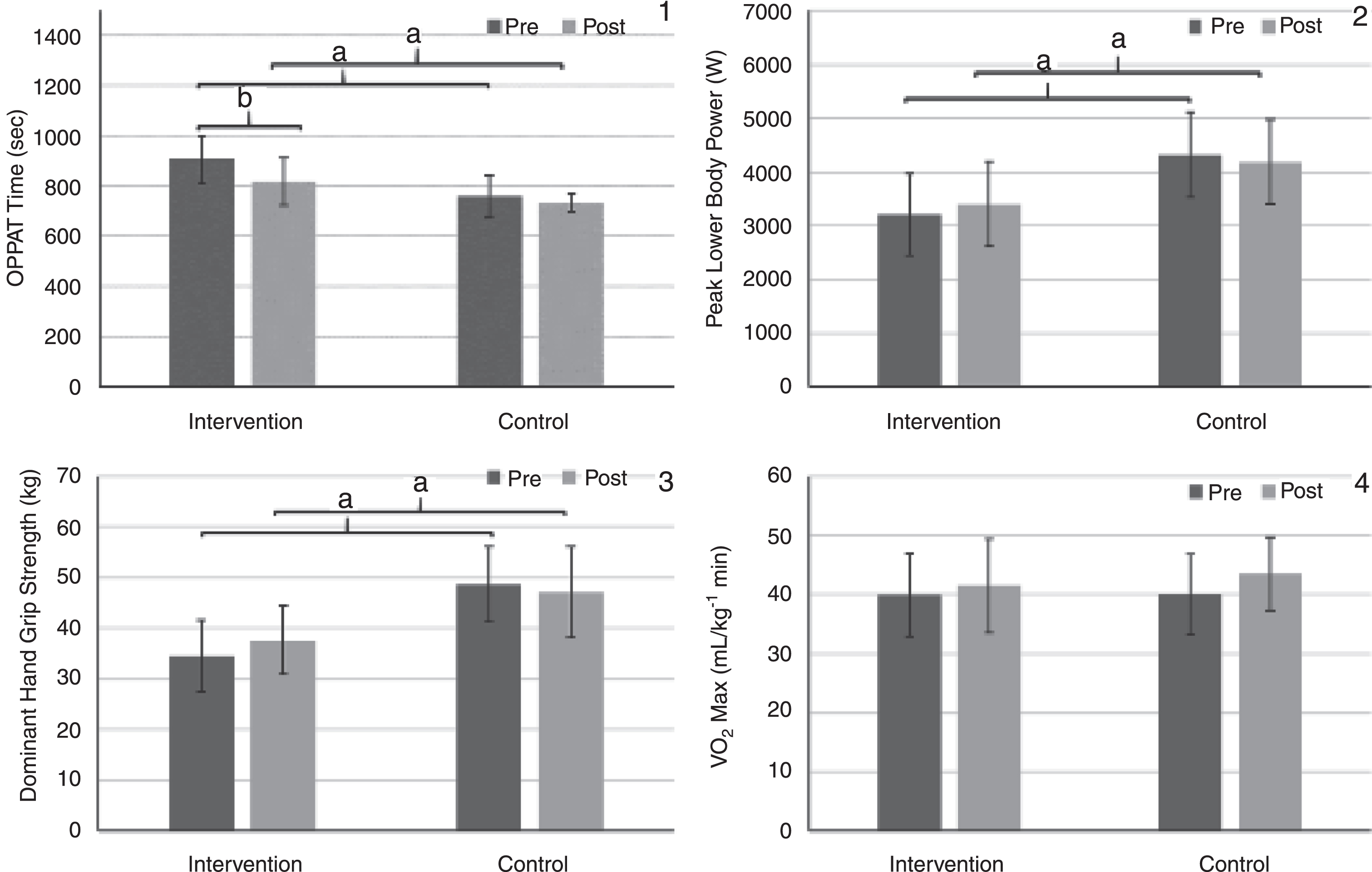
Simple mean comparisons of 1) OPPAT™ Completion time, 2) Peak Lower Body, 3) Dominant Hand Grip Strength, and 4) VO2 Max between groups and across time. ‘a’ represents a significant difference over time and ‘b’ represents a significant difference between groups.
Main effects of time, group and interaction effect for OPPAT™ times, peak leg power,
The within and between group comparison in fitness-related dependent measures revealed significant group and interaction effects for both peak lower body power and dominant hand grip strength, and a within effect for
Dominant hand grip strength and peak lower body power were related to pre-intervention OPPAT™ completion time. This informed the design of a 4-week strength and conditioning program that was developed to improve participant’s job-specific fitness by focusing on improving power and strength capacity. After completing the job-specific strength and conditioning program, the intervention group’s performance on the OPPAT™ improved. However, over 4 weeks participants in the intervention group did not demonstrate significant improvements in peak lower body power or dominant hand grip strength.
Peak lower body power was collinearly related with dominant hand grip strength, and was a significant predictor of OPPAT™ completion time. The importance of lower body power for the successful performance of paramedic work is a novel finding and likely serves to help explain emerging findings about the role of technique during scoop board lifting. Makhoul et al. [19] reported that those able to move a scoop board using a technique that minimized the loading on their spine did so by producing a greater proportion of work from the lower body relative to the upper body. Since work is the time integral of power, it is likely that paramedics who are better able to generate lower body power are in turn better able to produce more work through the lower body, thus able to lift more effectively from a biomechanical perspective. Identifying the relationship of peak lower body power and OPPAT™ performance, and understanding the mechanistic role of peak lower body power to lifting performance [19], reinforces the importance of training lower body power as a key physical attribute to support performance as a paramedic.
In the multivariate regression model, grip strength was not identified independently as a predictor of OPPAT™ performance because of the collinearity with peak lower body power. Although grip strength was not independently a predictor of performance, it remains an important consideration for OPPAT™ performance. The noted importance of grip strength is consistent with past findings identifying grip strength as the best predictor of one’s ability to carry a 90 kg patient [16]. Because of the links between lower body power and grip strength to OPPAT™ performance, the strength and conditioning program was developed with an underlying focus on improving these constructs of fitness.
Interestingly, cardiovascular fitness was not related to OPPAT™ performance. The lack of association is likely because participants were not allowed to run in the circuit and therefore complete it in a best effort time, limiting the cardiovascular demand of the test and likely weakening the relationship between
Since strength and power were significantly predictive of pre-intervention OPPAT™ completion time, the strength and conditioning program was targeted to improving these fitness measures. To achieve this training objective, repetition ranges were constrained to 6–8 by the end of the program. The selection of this repetition range was determined to balance the development of strength and power. To train strength, it has been suggested that repetitions should range from 5–10 in a set [31]. When focusing on explosive movement, sets of 6–8 repetitions have been shown to improve peak leg power [32]. Higher repetition ranges were prescribed in the first week of the program to focus on movement competency [26] and then progressed towards the 6–8 repetition range while concurrently increasing the resistance and emphasizing the maximal effort in every repetition to elicit strength and power improvements.
Following the strength and conditioning program participants in the intervention group showed significant improvements in OPPAT™ completion times. Although OPPAT™ performance time’s decreased post-intervention within the intervention group there was no concomitant improvement in either strength or power measures contrary to our hypotheses. The lack of significant improvements in strength or power is likely a result of the size of the improvements and the power of the study to detect small effects. As noted, the ANOVA model did detect significant interaction effects in peak lower body power and dominant hand grip strength but the improvements were small (d = 0.25 and d = 0.45, respectively). We hypothesized that the strength improvements would be more pronounced, suggesting our study design was not adequately powered. Despite the magnitude of change from a statistical standpoint, from a practical standpoint the modest improvement in grip strength and peak lower body power sufficed to significantly improve OPPAT™ performance. This reaffirms strength and condition as a suitable accommodation to improve an individual’s OPPAT™ performance.
The modest improvements in fitness may related to the duration of the program. In previous research, a one-year exercise intervention was introduced for the paramedic sector, where fatigue, as measured by blood lactate concentration, was significantly decreased when performing a stretcher carrying task [33] following the intervention. However, strength and conditioning programs likely do not need such a long duration to be successful as increases in maximum voluntary contractions during leg extension were observed after as little as 4 weeks of strength and conditioning training with 3 sessions a week [34], consistent with our approach. While improvements in strength in as little as 4 weeks have been documented in the literature [34] it is possible that participant training history reduced the magnitudes of the improvement. Training history was not assessed in this study design but all participants had some aspects of physical training incorporated into their college program where they participated in mandatory labs performing physical exertions with paramedic equipment. This level of pre-training may have limited the ability to substantially improve power and strength within 12 training sessions.
Accommodation and familiarization could also explanation improvements in OPPAT™ completion time. However, improvements were not detected in the control group. We believe this rules out an accommodation or familiarization explanation for the pre-post improvement in OPPAT™ performance among the intervention. As a result, the 4-week strength and conditioning program, while not eliciting statistically significant increases in grip strength or peak lower body power, was successful in improving OPPAT™ performance.
A 4-week strength and conditioning protocol did improve OPPAT™ performance, but did not restore performance to a level equivalent to the original high performance group. The differences pre- intervention were expected due to the group dichotomization process, but it was hypothesized that there would be no difference between groups following intervention. However, it seems that the difference between the intervention and control groups were too great initially to overcome with only 4-weeks of training. Following the intervention, the control group had an average OPPAT™ completion time of 734 (36) seconds (range of 667 to 783 seconds), well within the acceptable completion time window of 600 to 1020 seconds, and interestingly, faster than employed paramedics who complete the circuit in an average of 891 (93) seconds [35]. With the exemplary completion times demonstrated by the control group, the training intervention was not sufficient to eliminate differences between groups, as the initial gap was too large to overcome.
The strength and conditioning program was successful for its intended purpose of improving performance on the OPPAT™ for participants with slower performance on their initial attempts. In Canadian law, when considering PES as a BFOR there is duty to accommodate, or a requirement to have a process or program to address potential adverse impact through accommodation [9]. The results of this research demonstrate that evaluated job-specific strength and conditioning program can provide such an accommodation as it aided participants in significantly improving OPPAT™ performance. In fact, mean OPPAT™ completion time among the intervention group post- intervention was 816 (93) seconds, more than two standard deviations faster than the performance standard of 1020. This is consistent with the findings of Gumieniak et al. [14], demonstrating that strength and conditioning can improve performance in PES to address adverse impact.
In addition to the strength and conditioning program being successful as an accommodation to improve OPPAT™ performance, it may also serve to support injury prevention. Research demonstrates that paramedics with low fitness levels are more likely to suffer low back injury [36]. In contrast, evidence indicates that higher fitness, as gained through resistance training, is highly effective in reducing MSD symptoms [37]. By increasing paramedic fitness levels via a strength and conditioning training approach, not only will the potential adverse impact be addressed, but also may aid in reducing MSDs. While future research is required to evaluate the protective effects of a tailored strength and conditioning on paramedic long-term occupational health and well-being, these results underscore the importance of strength and conditioning to prepare candidates for completion of the OPPAT™ as a PES.
Familiarization was a potential confounding effect in this study. However, potential effect of familiarization was controlled for by ensuring that all participants had a minimum number of OPPAT™ attempts prior to their initial “live” performance in phase 1. Previous work shows that in a circuit based PES designed for the firefighting sector, performance stabilized by a participant’s fourth attempt as measured by a coefficient of variation of 2.6% for repetitions 4, 5 and 6 [38]. As a result, phase 1 OPPAT™ performance time were not recorded until each participants’ fourth attempt to account for a potential learning effect. Dominant hand grip strength and peak lower body power were used as surrogate measures for whole body strength and power, respectively. Although these measures only consider a portion of the body they continue to be used as time and cost effective surrogate measures for the estimation of whole body strength and power capacity [20]. Additionally, they may be safer to measure compared to one-repetition maximum testing and do not require complex equipment such as a dynamometer to measure. None-the-less, these data are based on surrogate, not joint-by-joint specific measures of power. Finally, the grouping of participants was done solely on initial OPPAT™ performance and did not consider personal characteristics such as sex, height and weight. This resulted in a control group composed of mostly males and greater stature, compared to an intervention group of mostly females and lower stature. With the majority of the control group being male the differences in peak lower body power and dominant hand grip strength between groups post- intervention may attributed in part to strength differences between sexes where females are estimated to have 2/3 the strength of males [39].
Future work should consider the effect of personal characteristics on OPPAT™ performance, use more robust fitness measures to assess strength and power improvements and apply the strength and conditioning program to incumbents that are unsuccessful on the OPPAT™. The purpose of this study was to evaluate the effectiveness of a strength and conditioning party to improve OPPAT™ performance by increasing the fitness of participants. However, other personal factors such as sex, height, weight and training history could influence OPPAT™ performance and were not considered in this study design. Second, the ability of this strength and conditioning program to improve fitness measures should be further investigated using more robust measures of power and strength such as one-repetition maximum testing. Finally, the effectiveness of this strength and conditioning program on improving OPPAT™ performance in candidates who are unsuccessful on the OPPAT™ should be evaluated. This study showed that the strength and conditioning programs was able to improve performance in low performers, but the majority of the sample was successful on the OPPAT™ on their pre- intervention trial. To confirm the efficacy of this strength and conditioning program as an accommodation its ability to improve performance should be assessed in candidates who were unsuccessful in their first OPPAT™ attempt.
Conclusion
Improvements in OPPAT™ completion time following a strength and conditioning intervention demonstrate that a job-specific strength and conditioning can provide a defacto accommodation for adversely affected candidates. By validating the developed strength and conditioning program as an accommodation to overcome this adversity, a key element (Step 10), in the best practice template for developing a physical employment standard [9], has been met.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We would like to acknowledge the support of Neil Freckleton and Craig MacCalman, the paramedic program coordinators at the participating colleges at the time of the study, for their efforts in facilitating this research. We would also like to acknowledge the support of Jessica Park, Jordan Taylor, Robert Wagner, and Danielle MacFarlane, all active duty paramedics that, in their off-duty time, were willing to support this research effort by serving as OPPAT™ lifting partners throughout the study.