
Abstract
BACKGROUND:
Several risk factors among packing lines workers can lead to Work-related Musculoskeletal Disorders (WRMSD) occurrence. Foreseeing WRMSD prevention and productivity increase, some furniture manufacturing industries have been investing in the adoption of robotic solutions. In this field, ergonomics plays an important role to verify if automation implementation has been successful.
OBJECTIVE:
This study aims to address the general impact and effectiveness from an ergonomics point of view of the implementation of a robotic aid in a packing workstation.
METHODS:
The Nordic Musculoskeletal Questionnaire (NMQ) was applied to 14 workers of semi-automated packing lines. Some additional questions about occupational conditions were included. In order to assess the ergonomic impact of the robotic aid, Rapid Upper Limb Assessment (RULA) was also applied by trained ergonomists, by analyzing the considered packing workstations before and after the adoption of the robotic aid proposed solution.
RESULTS:
The results showed that trunk torsion was the most highlighted WRMSD risk factor by all workers, associating it with the lumbar pain. The obtained RULA scores demonstrated that the adoption of a robotic aid eliminated this risk factor and, consequently, reduced the corresponding WRMSD risk.
CONCLUSIONS:
The adoption of robotic aids can be instrumental in reducing WRMSD risk in furniture manufacturing industries. Ergonomic studies with workers’ participatory approaches seem to be an appropriate strategy to enable the validation and development of industrial robotic solutions.
Keywords
Introduction
In the furniture industries with an important manufacturing component, there is a predominance of repetitive and manual tasks involving frequent lifting, pushing and pulling heavy loads and the adoption of awkward postures, such as trunk flexion and twisting [1, 2]. These occupational risk factors are often associated with Work-related Musculoskeletal Disorders (WRMSD) incidence [3]. The WRMSD occurrence constitutes one of the main occupational health problems, being a major cause of occupational absenteeism and decreased productivity [4]. Therefore, the WRMSD risk factors are responsible for a lot of damage to workers and are financially damaging the economy in general, being urgent its mitigation and prevention [5, 6]. For this purpose, the scientific literature shows that ergonomic intervention is the best prevention strategy to reduce the WRMSD risk [7, 8], meaning that the occupational risk factors must be assessed and, consequently, ergonomics improvements/redesigns must be implemented to improve health, safety and productivity at workstations [9, 10]. Different methods and tools have been developed to assess exposure to WRMSD risk factors, which can be divided into three groups according to the measurement technique, namely: self-report, direct measurement and observational methods [11].
In this field, aiming to reduce the human workload and diminish the WRMSD risk, automated solutions have been implemented, where robots play a major role mainly to perform repetitive tasks, non-critical, such as handling, welding and joining tasks [12, 13]. Recently, the Industry 4.0 paradigm aims at achieving efficiency, cost reduction and increased productivity, leading industries to implement several robotics solutions and integrated automation [14]. Industrial robots can lead today’s manufacturing industry to be competitive, replacing some of the cognitive and physical human-work [15]. These robots can perform continuously the tasks for which they are programmed with levels of speed, repeatability and precision impossible to achieve by human-workers [14]. However, the worker is the most flexible component of this robot-human binomial and also the most fragile. With this change in the manufacturing industry, comes the need to assess the risk that workers are exposed, due to the inertia, structure and process forces posed hazards by industrial robot systems [16]. Additionally, ergonomic criteria must be taken into account to enable and validate the design and deployment of human-robot tasks sharing. In this field, planning tools and methods are required regarding the effective allocation of work tasks between humans and robots and the design of work-cell layout, evaluating the ergonomic impact of the different task assignments [10, 18]. Concerning the furniture manufacturing, many companies are looking for automation solutions, but this industrial sector still is one of the least automated sector due to the lack of scientific and technical knowledge in this field [19]. According to statistical data [20], only 0.2% of all industrial robots operating worldwide are installed in the wood product sector (which includes the furniture industry).
The current study resulted from cooperation between a university and a large Portuguese site of furniture manufacturing, with the goal of studying a semi-automated packing workstation, where most of the workers were continuously exposed to WRMSD risk factors and reporting some kind of musculoskeletal complaints. Accordingly, the aim of this study is to assess the general impact and effectiveness from an ergonomics point of view of the adoption of a robotic aid in an industrial packing workstation.
Materials and method
Workstations studied
The current study was centered on an ergonomic intervention at three packing lines in a furniture manufacturing company. The selection of these lines was based on the significant rate of musculoskeletal complaints reported by the workers. The mentioned lines are composed by different workstations with robots and human-workers, accordingly to the following activity sequence: (i) robot packing box-maker; (ii) workstations with human-workers, who place the furniture pieces into a packing box; (iii) robots box-closer and labeling; (iv) robots for automatic palletizing and filming/strapping (Fig. 1). For each workstation with robots, there was a human-worker responsible for the supply of consumables, machines control/programming and problem-solving. These robots’ workstations were installed at the beginning and final of packing lines, separated from human-workers by safety fences. In the workstations where the manual packing takes place, the pieces to be handled are piled in a pallet, positioned behind the workers in a stacker. The packing box (previously made in the robot box-maker) is transferred to the workers’ area by a conveyor belt. In these workstations, the main handling sub-tasks are: (i) reach pieces from the stacker; and (ii) placing the pieces into the box packing. During these, the workers adopt a standing posture and, frequently, they twist the trunk. It should be noted that this is a task with a high repetitiveness, existing several musculoskeletal complaints reported by the workers. Based on these evidences, the company supervisors and safety practitioners, as well as the university analysts selected this type of workstation for the ergonomic intervention.

Examples of packing line workstations, namely: automation for packing box-maker; workstations with human-workers placing the furniture pieces into a packing box; robots for automatic palletizing and filming/strapping.
This study involved 14 workers, all of them belonging to three final packing lines, hereinafter designated by Lines 1 (n = 2 workers), 2 (n = 6) and 3 (n = 6). The lines’ selection was based on internal registrations of work accidents and WRMSD occurrence. Across these lines, the workers’ tasks are similar, varying only the dimensions and weight of the furniture pieces handled, according to the references produced. However, these furniture pieces are always of the same shape, i.e. rectangular and flattened.
The ergonomic intervention began with a first visit to understand the selected workstations, where some risk factors were identified. After that, six visits were carried out to collect individual data from each workstation, information about work organization, physical and mental requirements, workers’ complaints, working conditions, tasks performed, dangerous conditions and occupational risk factors. Photographs and videos of the workers performing their tasks were also registered.
In order to register workers’ perceptions, a preliminary questionnaire was applied. This questionnaire was structured based on the Ergonomic Workplace Analysis (EWA) [21] and adapted according to the study objectives. It was answered by the workers in teamwork for each packing line. This questionnaire allows the assessment of workers’ perceptions regarding several factors that influence the environment in which workers are inserted and that influence their exposure to occupational hazards. Topics covered include the following factors: workspace; physical activity in general; handling loads; postures and movements; risk of accident; repetitiveness of work; decision-making; lighting; thermal environment; and noise. For each topic, the workers expressed their evaluation through a qualitative scale composed by the following options: “- -” (the most negative evaluation); “-”; “+”; and “++” (the most positive evaluation).
In addition, the Portuguese version of the Nordic Musculoskeletal Questionnaire (NMQ) [22] was applied individually to the 14 workers of the considered packing lines. The NMQ is a standardized questionnaire used to evaluate and to characterize musculoskeletal symptomatology perceived by workers, considering their entire body. Additionally, for each body region, the musculoskeletal pain/discomfort intensity perceived was evaluated using a numerical scale (Visual Analogical Scale –VAS), ranging from 0 (without pain) to 10 points (maximum pain). Summarily, the application of this questionnaire was important to confirm workers’ complaints and to know the prevalence of WRMSD (as applied by Grzywinski et al. [23] and Asadia et al. [24]).
WRMSD risk assessment of the packing’ workstations
In ergonomics, workers’ posture and movements are important information for determining the WRMSD development risks in the workstations [25]. Considering the different tools and methods available to this risk assessment, in the current ergonomic intervention the Rapid Upper Limb Assessment (RULA) [26] was selected in order to assess the WRMSD risk related to existing packing tasks. This method has been widely used during ergonomic interventions in several workstations involving repetitive tasks/movements and awkward postures [10, 29]. Globally, these previous studies applied the RULA to evaluate existing workstations and, based on its results, to redesign workstations for ergonomic improvement. The RULA application combined with the self-reported musculoskeletal symptomatology questionnaires has also demonstrated an important contribution to the WRMSD risk assessment in workstations with manufacturing and repetitive tasks [30, 31]. Therefore, in the current study, the RULA assessment will support the ergonomic intervention, in this case, the implementation of the robotic aid, through the assessment before and after the intervention.
RULA is classified as an observational method for assessing WRMSD risk for the upper limbs, considering also the neck, trunk and lower extremities position during work activity [9, 11]. In this study, during the real-time and video-records observations of the 3 lines packing workers, the most frequent postures were identified in order to apply the RULA. Therefore, a total of 24 postures were considered (6 postures×2 packing tasks×2 occupational conditions, i.e. without and with robotic aid). For each posture, different joint angles were associated with a joint score according to a predefined range of angles. Joint angles were determined from digital images imported to LiteCAD®, version 2.0.0.48. These joint scores lead to a final RULA score, which is used to assign the observed posture into an action level indicating the required intervention. This method defines four action levels, namely: (i) level A (for final scores between 1 and 2), meaning that the posture is acceptable if not maintained or too much repeated; (ii) level B (final scores between 3 to 4), indicating that further investigation is needed; (iii) level C (scores between 5 to 6), further investigation and ergonomic intervention are needed soon; (iv) level D (scores equal and greater than 7), indicating that investigation and ergonomic intervention are required immediately. It should be noted that the RULA assessment was done by teamwork involving different researchers with expertise in applying the method, in order to increase the reliability of the results (as defended by Dockrell et al. [32]).
Results
Workers’ perceptions and musculoskeletal symptomatology self-reported
As mentioned above, a preliminary questionnaire was applied in order to collect the workers’ perceptions about the occupational conditions in their workplaces. The results (Table 1) show that the packing line with the most negative assessment across the different factors was the Line 1, where the workers pointed out the restricted working space between the stacker and conveyor belt and the high working rate as two of the negative factors. The factor with a negative score across the three packing lines was the “Movements and postures”. All the workers highlighted the trunk torsion as the worst posture adopted when they have to reach the materials and put in the packing-box. These results support the need for ergonomic intervention in these packing lines, highlighting the problem associated with the postures.
Summary of workers’ perceptions about their workplaces conditions
Summary of workers’ perceptions about their workplaces conditions
As mentioned above, the NMQ was applied in order to collect the reported complaints and musculoskeletal pain of the 14 workers of the studied packing lines. The respondents were all female, with a mean age of 36.1 (±11.3) years old and a mean work experience in the actual workstation of 4.7 (±4.3) years. The results (Figs. 2 and 3) show that the majority of workers reported musculoskeletal pain in two or more body regions, being the lumbar region (n = 14) the most affected one (considering the last 12 months and the last 7 days).
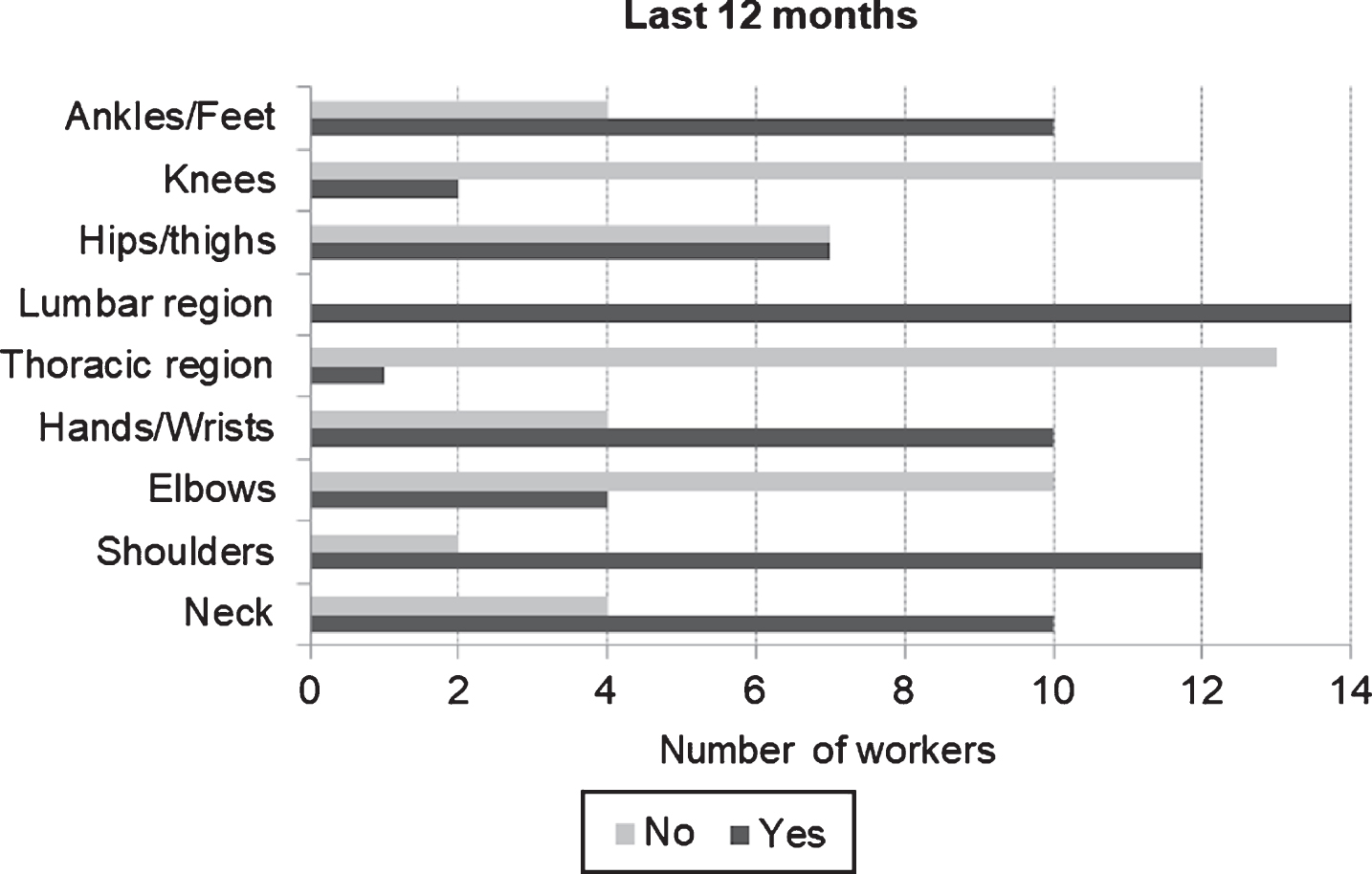
Relative frequencies of musculoskeletal symptomology for each body region perceived in the last 12 months (n = 14).
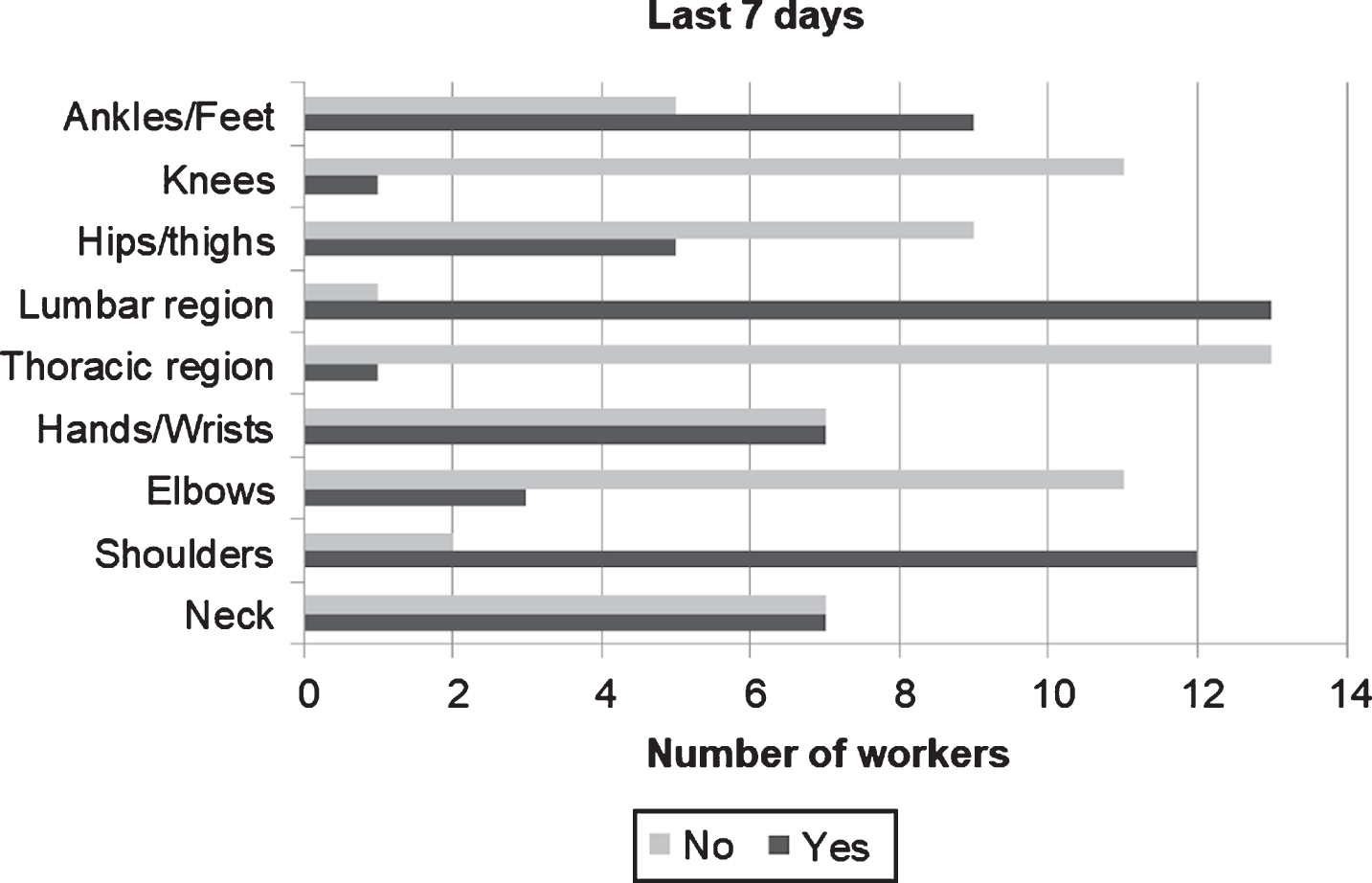
Relative frequencies of musculoskeletal symptomology for each body region perceived in the last 7 days (n = 14).
For each body region, as previously mentioned, the pain intensity perceived was assessed using a VAS scale. Consequently, in order to understand which regions are the most affected by musculoskeletal pain/discomfort, Table 2 presents the medians, maximum and minimum values for the scores (measured on an ordinal scale) of self-reported pain across the different body regions. Through this descriptive analysis of the scores, it can be observed that the lumbar region was the body region with higher pain intensity.
Medians, maximum and minimum values of pain scores reported for each body region
The results from the QNM show that, for 10 workers, the musculoskeletal symptoms are related to negative impact/limitations in their daily activities (e.g. housework or hobbies). In addition, nine workers reported having/had a WRMSD (one of these workers reported two types of these disorders). The WRMSD diagnosed were the following: (i) shoulders tendinitis (n = 4); (ii) (ii) wrists tendinitis (n = 2); (iii) herniation on the back (n = 2); (iv) acute low back pain (n = 1); and (v) carpal tunnel syndrome (n = 1).
From real-time and video-records observation, for each sub-task performed (reach and place pieces), it was selected 6 postures more frequently adopted by the workers (totalizing 12 postures for the condition without robotic aid) (Fig. 4). A RULA mean score was assigned to each task (Table 3). The results demonstrated that the upper limb, wrist and lumbar are the body regions with worst postures and that most negatively affect the RULA final scores.

Reaching and placing pieces into the packing box in the traditional workstations.
Summary of the RULA Assessment (mean scores±SD) for the traditional workstation (12 postures analysed)
In this preliminary study, the new robotic aid was installed only in Line 1, because this line is the one with fewer furniture pieces’ variability and also less work positions, making it technically easier to implement the changes. It should be noted that, according to the workers’ perceptions, this line obtained the most negative assessment across the different factors presented in Table 1, highlighting the importance of the robotic aid. This robotic aid is composed of a robotic arm with suction cups that individually transfers the pieces to a conveyor belt, which carries the pieces to the workers’ area (dispensing them frontally as observed in Fig. 5). In this case, the workers have to reach the pieces and to put into the packing box; this task started to be made in the workers’ sagittal plane, without the need to reach the pieces from the stacker, eliminating the trunk twisting. The RULA results presented in Table 4 show that the introduction of robotic aid was positive in the postural correction problem reaching and placing subtasks. In this case, the trunk twisting was eliminated, as well as arms flexion and abduction were reduced. However, the final score indicated that further investigation is recommended. In fact, there are still some remaining risk factors, such as inadequate posture of the hand-wrist system and repetitiveness.

Reaching and placing of pieces into the packing box in the workstation with the new robotic aid.
Summary of the RULA Assessment (mean scores±SD) for the workstation with robotic aid (12 postures analysed)
The NMQ results (Figs. 2 and 3) pointed out to the high prevalence of self-reported musculoskeletal symptoms in two or more body regions, being shoulders and lumbar the body regions with an increased number of musculoskeletal complaints, concerning the pain incidence and severity (Table 2). These results demonstrated the important WRMSD risk among these packing workers and are in accordance with previous studies developed in industrial manufacturing contexts with manual assembly and packing tasks [23, 33], justifying the need for ergonomic intervention in this type of workstations. Simultaneously, the NMQ results showed that different workers have WRMSD diagnosed, which can interfere both in their daily activities, as well as in their work performance (as defended by Schneider et al. [4]). In addition, regarding the workers’ perceptions preliminarily collected (Table 1) the postures and movements adoption and repetition constitutes the work factor more negatively highlighted across the packing lines. As mentioned above, the repetitive trunk torsion was the posture more referred by the workers, associating it with the lumbar pain perceived by them. Globally, these results support the need for the ergonomic intervention based on RULA postural assessment and help to define objectives of this intervention. Besides that, the workers’ involvement is an important factor for problem identification and for successful workstations interventions/modifications. In this field, Guimarães et al. [2] also developed a study based on participatory ergonomics intervention in a Brazilian furniture company, concluding that the workers’ participation was crucial for the success of the ergonomic modifications. In this case, the workers demonstrated an increased motivation and satisfaction with the new work design, which was explained by improvements inserted as well as by the teamwork done. Petit et al. [8] defended that the risk assessment is a major step in any preventive intervention to eliminate or reduce the WRMSD, using different ergonomic tools and methods, such as self-reporting tools (e.g. QNM), and observational methods and tools (e.g. RULA). In accordance with the methodology applied in the current study, the referred authors also defended that such assessments require the participation of workers and the technical expertise team.
Relatively to the RULA assessment of the traditional packing workstations (Table 3), the results were in accordance with the workers’ perceptions and musculoskeletal symptoms. The final RULA score indicated that further investigation and ergonomic intervention are needed soon for both subtasks evaluated (reaching the furniture pieces and placing them into the packing box). The flattened shape of the furniture pieces, without handles, compromised the hand-wrist position, often occurring wrist torsion, flexion, and extension, with the aggravating of the hand having to support the load (between 2 to 4 kg). In this work situation, the materials were located behind the workers, leading to arms flexion and abduction, as well as trunk twisting to reach them. Another important risk factor assessed is the work repetitiveness, all these postures and movements were repeated more than four times per minute.
Therefore, the RULA assessment, the workers’ perceptions, and NMQ results support the introduction of a new robotic aid at the packing line, in order to avoid the trunk twisting. As mentioned before, this aid allows dispensing frontally the furniture pieces to the worker, so that the handling tasks will always be carried out according to workers’ sagittal plane (Fig. 5). In this field, it is evident that this type of robotic aid can decrease the workload related to the manufacturing tasks [34]. Thereafter, intending the ergonomic assessment of this workstation intervention, the RULA was applied, demonstrating that in this new packing workstation the WRMSD risk was reduced (Table 4). However, this assessment indicated that further investigation is needed, mainly, due to the work repetitiveness and wrist position during the handling of the pieces. These two risk factors are still present in the redesigned workstation. Therefore, several preventive measures, already implemented in the industry under study, should continue to exist even with the robotic aid introduction, namely: (i) workers’ training and recommendations to use safe working postures and handling techniques (as defended by Grzywinski et al. [23]); (ii) labor gymnastics; (iii) correct organization of the workday to include recovery times [27]; (iv) job rotation for alternating workers between tasks with different exposure levels and occupational demands [35, 36]. It should be noted that the mentioned measures have been frequently associated with WRMSD prevention, but also with the enhancing of workers’ job satisfaction and productivity [35]. Consequently, this ergonomic intervention showed that the robotic aids are important in these workstations to prevent awkward postures and WRMSD risk, as well as this type of intervention, should be conducted with a multidisciplinary team, including ergonomic expertise, workers and industrial engineers (among others practitioners). It is believed that an integrated and participatory approach to workstations’ design/redesign in order to prevent WRMSD is highly important [37, 38], being the methodology applied in the current study, to assess the existing and the redesigned workstations, appropriate for these ergonomic interventions.
As future work, it is intended to deploy this ergonomic intervention with the implementation of a robotic aid in the remaining packing lines. However, other solutions for lines in which there is a higher variability of piece for packing, and a higher number of pieces/elements to be inserted in each packing box, have to be studied in more detail. In these situations, collaborative manufacturing with physical human-robot interaction may be recommended, enhancing the versatility and adaptation to dynamic working environments or sudden changes in production [14].
Conclusions
Manufacturing furniture is an industrial context with several WRMSD risk factors. Ergonomic assessment of workstations with and without robotic aids would give an important contribution to the WRMSD prevention. In the current study, a new robotic aid was introduced in a packing workstation and its ergonomic impact was assessed through the RULA method, verifying that this intervention leads to the improvement of workers’ postures, reducing the risk of WRMD. Additionally, the workers were involved across the study and their perceptions are in line with the ergonomic assessment, highlighting the importance of participatory ergonomics during workstation interventions.
However, future work is required in order to deploy this ergonomic intervention in the remaining packing lines, as well as to investigate other solutions for lines in which there is a higher variability of pieces for packing and tasks. Hopefully, the practices and recommendations presented in the current study would be helpful to other assessments at the company involved in this case study but also for other industries with similar problems.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This work has been supported by FCT –Fundação para a Ciência e Tecnologia within the R&D Units Project Scope: UIDB/00319/2020.