
Abstract
BACKGROUND:
Increasingly, occupational and physical therapists are using safe patient handling and mobility (SPHM) equipment, such as mechanical lifts, in rehabilitation. However, there is little guidance in the literature on how SPHM equipment can be used to assist patients to reach rehabilitation goals. The purpose of this projectwas to document and categorize common and innovative ways rehabilitation therapists use SPHM equipment in their clinical practice.
OBJECTIVE:
This article investigates common and innovative uses of SPHM equipment in rehabilitation practice.
METHODS:
Occupational, physical and kinesio therapist employed at the Veterans Health Administration wrote narratives and took photos describing rehabilitation therapy activities where they used SPHM equipment in their clinical practice. The authors used a systematic process to review and categorize the narratives and subsequent photos by using the World Health Organization’s International Classification of Functioning, Disability and Health (ICF).
RESULTS:
Thirty narratives (13 innovative and 17 common) were coded into four categories on the ICF section of mobility. The most common category was “changing and maintaining basic body position”(21) followed by “walking and moving” (5). The category “carrying, moving and handling objects” garnered two narratives and there were no narratives for “using transportation.”
CONCLUSIONS:
Project findings may serve as a guide for therapists who would like to enhance their use of SPHM equipment in rehabilitation. Additional research is needed to expand the use of SPHM in rehabilitation practice and evaluate the impact on patient rehabilitation outcomes and therapist safety outcomes.
Keywords
Introduction
Caregiver safety and patient safety are integrally linked by organizational culture, principles, methods and tools for creating safety. Yet, many health care organizations continue to “silo” worker from patient safety [1]. Over the past decade, an evidence-based, ergonomics approach to patient handling is replacing manual patient handling, resulting in decreased patient handling-related injuries among caregivers [2] and improved patient outcomes [3]. Increasing evidence suggests that Safe Patient Handling and Mobility (SPHM) in-patient programs also positively affect patients’ health. In hospitals with SPHM programs, patients are moved more frequently, are more engaged in activities, have a higher level of functioning at discharge, are less combative, and experience less depression [4–7]. They also experience fewer complications of immobility such as pressure ulcers, falls, and urinary dysfunction [7].
Although many occupational (OT) and physical therapists (PT) see the value in using equipment to promote safe patient mobility and function, some therapists believe that the use of SPHM equipment can interfere with rehabilitation goals of improved mobility and increased independence [8, 9]. Part of the dilemma is that there are no guidelines for therapist in the use of SPHM equipment in therapy. Also, there is scant research showing improved patient outcomes as a result of using SPHM equipment. As far back as 2005 there have been calls for the development of guidance for use of SPHM equipment in therapy [3, 9–11]. However, no such guidance has been forthcoming.
Recent studies have examined the effects of SPHM equipment in rehabilitation on patient outcomes [3]. Arnold and colleagues [7], conducted a retrospective study using Functional Independence Measure (FIM) ratings with patients following a stroke in a 20-bed acute inpatient rehabilitation facility before and after SPHM implementation. The group exposed to SPHM had higher discharge FIM scores than the group without exposure. In a larger project, Campo et al. [12] and Darragh et al. [13] compared the mobility and self-care outcomes of 507 patients admitted to rehabilitation prior to SPHM program to 784 patients admitted after SPHM implementation. They found no statistically significant differences between the groups in mobility and self-care discharge FIM scores, indicating that the SPHM program did not create patient reliance on equipment and promote physical dependency. In addition, two studies have found a decreased risk of pressure ulcers in extended care and long term care institutions with a SPHM program [4, 14].
In general, SPHM technology has improved and expanded the equipment options for use in rehabilitation [10, 13]. In a qualitative study with OTs, PTs and assistants, Darragh et al. [15] explored how therapists integrated SPHM equipment in rehabilitation and its effect on practice. They found that therapists reported greater options in patient care activities when using SPHM equipment especially those who were dependent or obese. In selecting equipment, they found that therapists underwent a complex decision-making process that considered multiple types of equipment, potential effects on the patient, patient limitations and the safety of the patient and the therapist. Hence, further exploration of the use of SPHM equipment and guidance on their use may mitigate the complexity of the decision-making process.
This project is a first step in describing and categorizing current SPHM practices in rehabilitation within the Veterans Health Administration (VHA). By describing and categorizing common and innovative uses of SPHM equipment in rehabilitation, it is hoped that all therapists will have a better understanding of SPHM practicesthat support patient rehabilitation goals while protecting therapists and therapy assistants from injury. In addition, it is hoped this work will inspire others to explore creative uses of SPHM equipment in rehabilitation.
Method
This project was approved as quality improvement project by two VHA Medical Centers (Tampa and Milwaukee) and three universities (George Washington University, Mercy College, and Nova Southeastern University). The Ohio State University Office of Responsible Research Practices approved the project as a research study; therefore, potential participants signed an online consent document that indicated if they would allow their data to be used for research purposes. All participants signed the document approving use of their data for the study.
The project used a photo-narrative methodology and an expert panel to assess and categorize common and innovative uses of SPHM equipment in rehabilitation. Photo-narrative is one of many available participant-generated image research methods [16]. Common uses were defined as typical or routine use of SPHM equipment during occupational or physical therapy sessions. Innovative uses were defined as the use of new SPHM equipment, new applications of existing SPHM equipment, and an atypical or creative use of equipment to allow performance of patient activities that enhance rehabilitation goals. The participants were instructed to not photograph patients, but rather have their colleagues or themselves demonstrate the activity.
Sampling and recruitment
Therapists were recruited from the VHA through an email distribution lists and by word of mouth. The therapists met the following criteria: (1) clinical focus in rehabilitation defined as acute or transitional rehabilitation, subacute care or nursing home; (2) employed as an OT, PT or Kinesio therapist (KT) by the VHA; (3) minimum of five years of clinical work with at least one year of SPHM equipment use; (4) agree to obtain permission of their hospital to take pictures of the therapy equipment (for group two this was the same facility); and (5) agree to obtain permission from any persons they take pictures of using the therapy equipment.
There were two groups of participants. In group one, therapists took pictures and described therapeutic activities at their respective VHA facilities following an online or self-paced training session. Therapists from group two attended a training at the VHA SimLearn labin Orlando, Florida, where they took pictures and described the therapeutic activities performed in the lab.
Procedures
Training in project procedures was provided to all participants. The first group was offered a one-hour, online training. Slides were emailed to participants prior to training and to participants that could not attend the session. For the second group, two co-authors gave a face-to-face presentation at the SimLearn facility using the same slides from the online training. The following topics were covered in the training: authors introductions, project purpose and objectives, tips for taking photos, examples of photo-narratives, accessing the Research Electronic Data Capture (REDCap) survey and how to upload photos and permission forms.
For the first group, an email invitation was sent to all individuals who expressed interest in participating. The invitation contained a unique identifier generated by REDCap. REDCap is a secure web application for building and managing online surveys and databases administered through the VHA. For both groups, follow-up reminders were sent at one, two, and three weeks after the initial invitation. For group one, at the request of some participants, the survey was active for six months. Email invitations were sent to the second group and photo-narratives were collected over seven weeks.
Each participant had to complete one REDCAP survey. Within the survey, each participant was required to complete one demographic form and a photo narrative forms for each (up to six) common or innovative use of SPHM equipment. Photos were taken with mobile phones, tablets or cameras and participants were encouraged to take up to three photos per therapeutic activity. Due to privacy issues, participants were required to use themselves and colleagues to demonstrate the therapeutic activities rather than patients. Participants were encouraged to create a folder on their personal VHA drive to store all narratives and photos prior to uploading into REDCap. In addition, a photo narrative “cheat sheet” was sent to each participant prior to data collection that included all the demographic and photo narrative questions that were on the REDCap survey.
Participants obtained permission from their facilities to take the photographs (using a standard memo of concurrence) and all individuals in the photographs signed a standard photo release (Department of Veteran’s Affairs form 10-3203). All signed forms were uploaded to REDCap.
Survey
The survey began with questions about the participant personal information covering; profession (OT, PT or KT), number of years they have worked with SPHM equipment, primary practice setting, the number of patients they saw per day, and what SPHM equipment they use in clinical practice. Participants were asked to submit up to three common and three innovative activities using SPHM equipment in rehabilitation. The participants determined if they considered the activity common or innovative. Each activity was described in a separate narrative with up to three photos to visualize what was described in the narrative. For each narrative, participants were asked four additional questions: the appropriate types of patients, precautions to consider, limitations of this technology and if other SPHM equipment could be used to facilitate this activity. Once completed, the photos and narratives were captured and stored securely behind the VHA firewall in the VHA Informatics and Computing Infrastructure (VINCI). The survey could only be accessed through a VHA account. Skip logic was used throughout the survey, so that if at any point the participant responded no, for example, “would you like to add another activity,” they would jump to the last page thanking them for their participation.
Analyses
To classify the photo-narratives into function-based units, the expert panel discussed and agreed to use the International Classification of Functioning, Disability and Health (ICF) as the coding taxonomy [17]. The purpose of the ICF is to provide a standardized language and framework for the description of health and health related states [17]. The ICF coding system provides four domains of classification (body structures, body functions, activities and participation, and environmental factors). The researchers used the codes for activities and participation domain as it best represented the activities described in the photo-narratives.
To code the photo-narratives, four expert panelists (one occupational therapist and three physical therapists) worked in two-person teams. Using the narratives and photos, each panelist independently developed short descriptors to label each therapeutic activity. They then conferred with the other person to check agreement. There were no inconsistencies. The ICF provides varying levels of detail by describing an activity using first (called chapters), second, third and fourth level codes. The researchers used the short descriptors along with the narrative to assign each narrative a code. For example, a photo narrative that used a portable floor-based lift device to partially assist a patient in gait training on a level surface but did not designate distance was assigned a second level code d450 (walking). A photo-narrative that depicted a person using a ceiling lift to assist in training a person with walking upstairs was assigned a third level code d4551 (climbing). Second and third level codes were used from Chapter 4 on mobility.
Results
Sample
The total number of participants was 17; 10 OTs, 6 PTs and 1 KT. The participants were from 12 out of a possible 18 Veterans Service Integrated Networks, a regional designation for the VA. Participants were from 13 states and oneUS territory. They worked in a variety of settings; five in rehabilitation, three in outpatient, three in acute care, threein home health, twoin long term care and onein another not specified setting. The number of patients seen in one day by the therapist ranged from threeto 12 with an average of seven. This was not necessarily the number of patients where they used SPHM equipment in their rehabilitation practices. Participants reported using a variety of equipment in their clinical practices: all used powered beds, most used ceiling lifts [14] and floor-based lifts [13]. Only one participant used an air assisted transfer device. Two participants listed other equipment that they use in their practice: vector variable body weight support system, power lift toilets and car lifts. The average number of years that the participants had been working with SPHM equipment was 4.6 (range 2.5 to 18).
Photo-narratives
Participants submitted 40 narratives (Table 1). Eighty-six (86) photos were submitted to portray the narratives. Ten (10) narratives were eliminated because: the practice was deemed unsafe (2), the equipment in the photos was not considered SPHM equipment (2), duplicates narratives that were uploaded twice (4), and the activity could not be determined (2). Therefore, 30 narratives and the corresponding photos were coded into ICF categories on mobility.
Summary of chapter 4 second and third level codes
Summary of chapter 4 second and third level codes
The participants submitted 17 common and 13 innovative narratives. Common narratives included the use of SPHM to enhance transfers and bed mobility, increase a patient’s performance of activities of daily living (ADL) and instrumental activities of daily living (IADL). Innovative practices included advancing pre-gait and gait training, facilitating strength training, and improving balance and coordination to prevent falls.
Table 1 shows the distribution for ICF second and third level codes. Two narratives were not assigned a level three category, because they did not include that level of detail and three narratives had two level two categories. The most common narrative was “changing and maintaining basic body position” followed by “walking and moving.” There were two narratives for “carrying, moving and handling objects. There were no examples of “moving around using transportation.” After coding, the expert panelist chose activities using SPHM that they would endorse. Three activities, one each for the secondary heading were chosen for “changing and maintaining basic body position”and one was chosen for“walking and moving.” The panelist thought the two examples of carrying, moving and handling objects were not good examples for that category.
Changing and maintaining basic body positions
Maintaining a Body Position (Fig. 1)
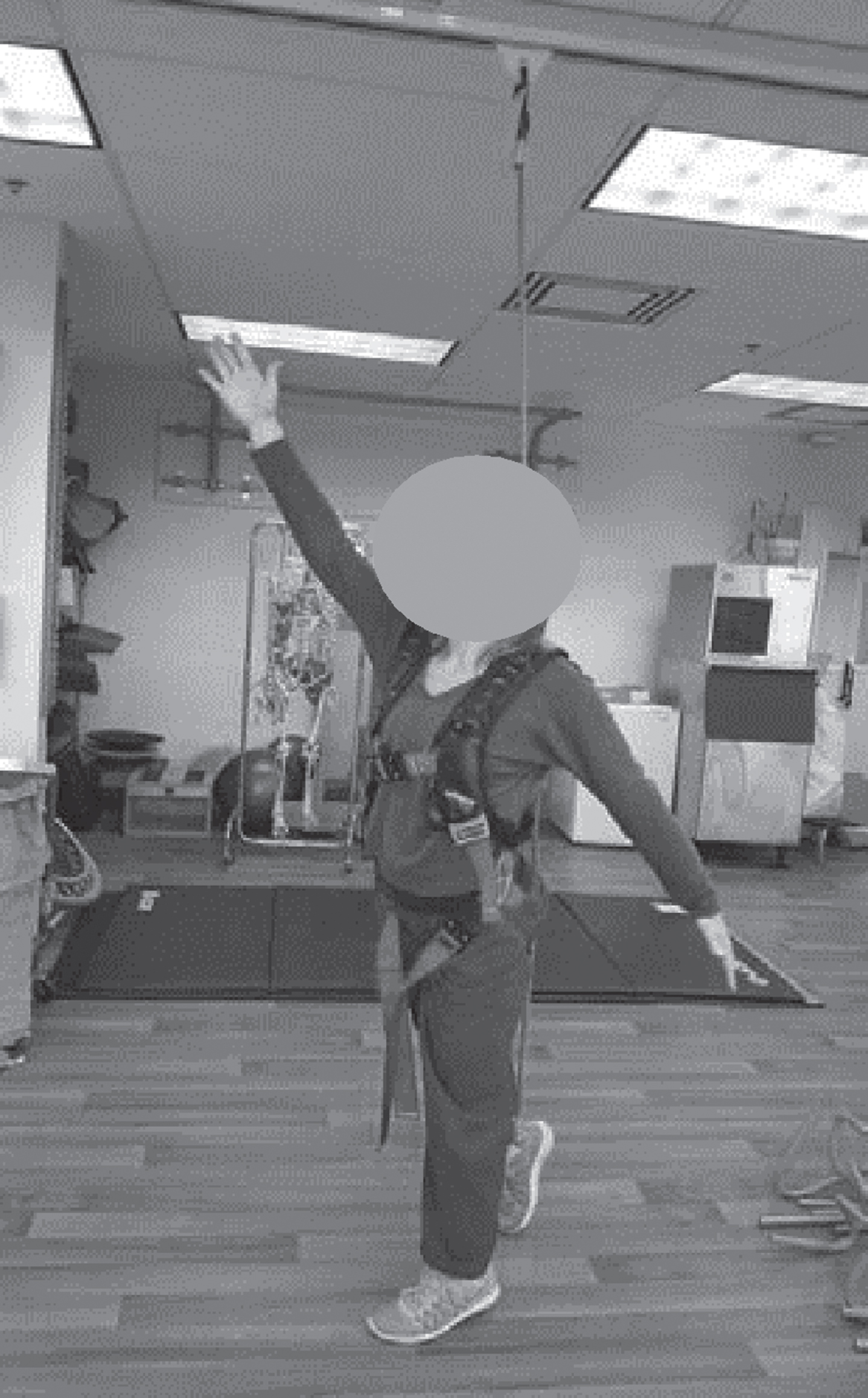
Changing basic body positions.
This is an example of a Large-Scale Voluntary Transfer (LSVT) BIG© exercise while using a ceiling lift and harness. This would be used with patients who have Parkinson’s disease. It requires knowledge of LSVT BIG exercises, and enough open space to do the exercises (not conducive to a small clinic or very busy time of day in a large clinic). –Outpatient PT
Changing and Maintaining Basic Body Positions Unspecified (Fig. 2)
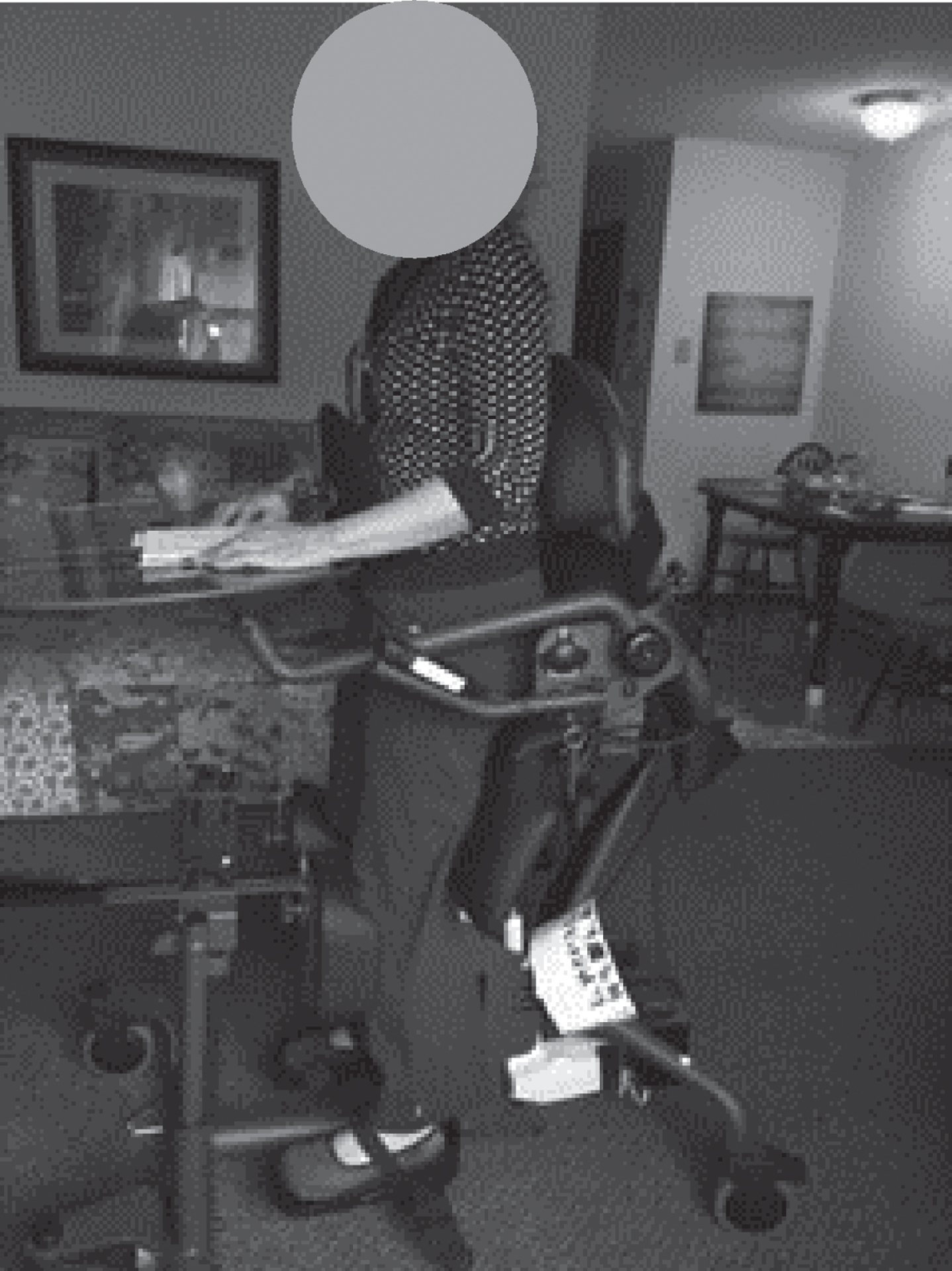
Maintaining a body position.
This is an easy stand lift. This SPHM tool is a lift for exercise purposes. It helps patients who cannot stand on their own to exercise and increases the amount of time they are standing. They can read a magazine or eat something and stand at the same time. Some patients find it boring to stand for so long with nothing to do, but this equipment allows patients to do something they enjoy while they are standing. It is important that the lift has a table because it increases the amount of standing time that patients can endure. I have a bilateral amputee patient who is dependent on a lift for his ADLs and all transfers. He stays there between forty minutes to an hour. It would be extremely unusual for him to stand for that long without this machine. We have about three hundred patients in Home-Based Primary Care and only two of our patients have these machines because you have to medically justify why the patient needs it. The VHA is on the right track for providing these to patients. –Home-Based PrimaryCare OT
Transferring Oneself (Fig. 3)
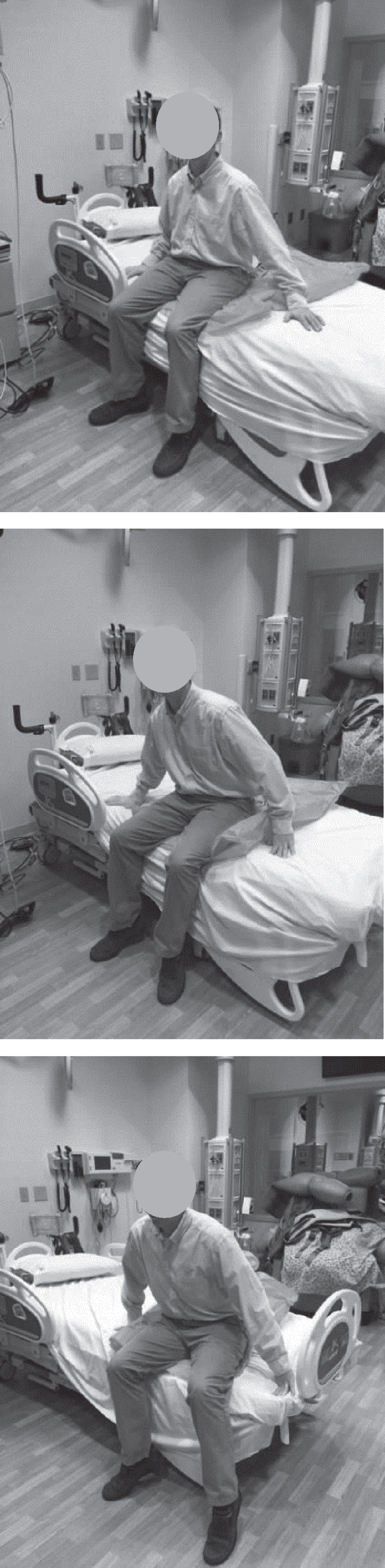
Transferring oneself.
Scooting up and down when sitting on edge of bed (EOB) and/or scooting forwards and backwards when sitting EOB. Use of friction reducing sliding sheet to facilitate scooting up or down at EOB. The sheet reduces friction, allowing a person to slide easier on the mattress and sheets. It promotes a smoother weight shifting for lateral sliding, like a ‘conveyor belt’ mechanism. With an easier gliding motion, the sheet can reduce skin shear during lateral transfers. Alternately, use the sheet to facilitate scooting forwards and backwards to sit at EOB. Use the sliding sheet with patient populations of post-Cerebral Vascular Accident (hemiparesis/hemiplegia), bariatric, amputee, and debility. - Rehabilitation OT
Moving Around Using Equipment (Fig. 4)

Walking.
Obstacle course gait in parallel bars using solo step on track. Progressing from inside parallel bars to outside of the bars. Does not have a motor, patient is dragging the cord with them. To be used with high fall risk, amputee, post CVA, and Parkinson’s patients. –Outpatient PT
For each narrativethe participant was asked; “For what types of patients would this activity and technology be appropriate?” There were 68 comments, two were excluded because they did not refer to type of patient or technology. Five themes emerged; patient strength, disability, unit type, patient’s ability to perform the activity and type of mobility activity. Patient strength garnered the most comments (29 comments), patients who were deconditioned, needed to be weight bearing, paralyzed or partially paralyzed are all examples of strength needs of the patient to perform the therapeutic activity. The second most common comment (20 comments) was to list the patient disability or type of hospital unit the patient would most likely be admitted. Examples of patient types were; geriatric, stroke, orthopedic, vestibular, bariatric, amputee or those with pressure ulcers. The hospital unit included post-operation, intensive care unit and surgical. There were four types of patient abilities (9 comments) to perform the activity mentioned, such as; able to follow instructions, motivated and able to assist. The last category related to types of mobility task undertaken, such as; repositioning and ambulation had 5 comments.
Precautions
For each narrative, the participant was asked; “Are there any precautions to consider when using this technology for this activity?” There were 46 comments. Comments were grouped under four themes; patient abilities, equipment, patient health conditions and general safety. Examples of the comments indicating patient ability (17 comments) included “able to bear weight,” “goodendurance” and “good trunk control.” Examples of equipment precautions (17 comments) were;“appropriate and fitted sling,” “ensure brakes are locked” and “do not leave sliders under patients on gurneys with no rails.” Seven comments addressed patient abilities, such as; “taking consideration of feeding tubes, lines, catheters, incisions and blood pressure changes.” There were five comments about general safety, such as; “observe patient to avoid harm,” “have a second per assist to take care of lines.”
Limitations
The third question for each narrative was: “What are the main limitations of this technology for this activity?”Of the 60 comments representing four themes. The themes were; logistics, equipment, patient abilities, and setting. The most common comment was about logistics (20 comments), such as; “time to set up,” ease of operation for family caregiver, space needed and if the activity needed two therapists. Equipment issues included comments (18 comments) such as; fit of sling, comfort and if it was appropriate for bariatric patients. There were 15 comments about the patient’s ability, such as; patients with memory issues or patients of size. Finally, specific strength characteristics were mentioned four times and refereed to upper or lower body strength. There were three comments about the setting; size of room and appropriate for home or outpatient settings.
Other technology
The final question for each narrative asked: “Please indicate if any other SPHM equipment could be used to facilitate this activity?” In all there were 37 comments. Seventeen comments mentioned specific brands of equipment. After brands there were generic mentions of; ceiling lifts, sit to stand lifts, floor based lift, ceiling lift with harness, and no equipment (using multiple therapists).
Discussion
We found that therapists used SPHM equipment for a variety of tasks with a variety of patients. The most frequent uses were categorized under the ICF code “changing and maintaining body positions” [18, p. 5]. This highlights the use of equipment for patients who are unable to stand or begin to ambulate without assistance. This is consistent with Darragh et al. [15], who studied perceptions of therapy staff in three facilities that had comprehensive, mature SPHM programs. The authors found that SPHM equipment was useful to mobilize more debilitated or dependent patients. Therapists in that study referred to increased therapeutic potential. They could mobilize and work with patients that they could not assist safely without equipment. In acute care, where patients tend to be more dependent, similar findings are found in the literature. Olkowski and Steffi [19], surveyed therapists and found that in acute care, therapists used the equipment to improve provider safety and the quality of therapeutic interventions. In the current project, therapists described similar types of mobility tasks and noted the importance of the equipment in promoting patient and therapist safety during these tasks.
In addition to the use of SPHM equipment for common rehabilitation activities such as standing and ambulation training, the project purpose projectwas to determine how equipment is used creatively. Out of 30 coded narratives, 13 were considered to be innovative by the participants. These innovative approaches included activities with multiple tasks (such as standing while grooming) or presenting higher level challenges to patients (such as ambulating through an obstacle course). This contrasts with Darragh, Campo and Olsen who studied therapists after a no-lift program was implemented in a rehabilitation hospital [8]. Therapists in that study felt that only the most dependent or the heaviest patients required equipment and that patients needed to move beyond equipment quickly. The perceptions of participants in the current project were more consistent with the therapists in the study by Darragh et al. [15] who also discussed combining tasks and making therapy more challenging. These results would support the notion that equipment could be used more creatively and more often in rehabilitation, especially for higher level functional activities. In the current project, there were few narratives that addressed ADL, such as grooming, dressing, bathing and toileting, indicating an area needing further exploration. Because only two narratives depicted self-care, perhaps therapists could be challenged to develop innovations to use SPHM equipment for self-care including but not limited to dressing, eating and drinking. Other self-care categories, i.e., washing oneself, caring for body parts and toileting, may have been better represented with reports from nurses who focus more on these areas than do therapists. An opportunity for innovation in the use of SPHM equipment in self-care is in “ensuring one’s physical comfort.” As clinicians look for ways to manage pain with fewer narcotics, perhaps researchers should examine the use of SPHM equipment in conjunction with integrative health strategies to reposition for comfort while decreasing the need for pain medications.
Because we asked the therapists in the current sample about specific rehabilitation tasks, we did not have the opportunity to explore the use of SPHM equipment for non-rehabilitation uses. One surprising finding by Darragh et al. was the frequency and utility of SPHM equipment for passive mobility [15]. Therapists in that sample frequently noted that many situations in rehabilitation required passive mobility. Examples included moving a patient from the wheelchair to the mat table prior to the therapy session, or getting the patient out of bed and into the rehabilitation gym. Even in rehabilitation, where active mobility is stressed, the ability to move patients passively, safely, and quickly is important. These findings should not be overlooked despite the current studies emphasis on active tasks.
While participants recognized the benefits of SPHM equipment, they also reported limitations in terms of logistics (e.g., time and space requirements), equipment issues and patient characteristics, all of which have been reported as barriers (19). However, literature exists that may provide insight to these perceived barriers. Regarding time limitations, researchers have documented that it takes significantly less time to use SPHM technology to move patients than manual team lifting approach (10.3 minutes vs. 14.86) [20]. When nurses weigh the cost of time against the benefit for themselves and for patients they are willing to sacrifice the time required for using SPHM equipment [20, 21]. Regarding space limitations, the availability of easily accessible space for storage has been cited by others as a barrier for equipment use [19]. Patient rooms and bathrooms may be too small to accommodate SPHM equipment such as floor-based lifts. Therapy rooms, while larger, are often at capacity with other equipment and may not accommodate portable lifts. Ceiling-mounted lifts overcome space barriers; they that require no footprint, are always accessible and are easily used in therapeutic activities. [14, 22].
Another barrier in the successful implementation of SPHM programs is the lack of interprofessional SPHM practice among therapists, nurses and others healthcare staff who use SPHM equipment. Greater communication and collaboration among these stakeholders would facilitate learning on all current uses of SPHM equipment (therapeutic and non-therapeutic) and encourage innovative problem solving to explore new uses that promote functional goals while enhancing worker and patient safety.
Finally, regarding patient characteristics, nurses have found that carefully matching patient function and type of movement desired with type of equipment will facilitate mobility [24–26]. In the same way that patient assessment guides the prescription of assistive devices, such as canes, walkers and wheelchairs, in rehabilitation, physical and cognitive assessment also guide the use of SPHM equipment. Some SPHM equipment such as full body slings are best for patients with low levels of cognition and mobility whereas sit to stand devices are only appropriate for patients who can bear weight and follow simple instructions.
Limitations and precautions
While results of this descriptive project are useful in better understanding the uses of SPHM equipment in rehabilitation, limitations should be noted, and findings may not be directly useful for recommending changes for therapy practice. The project was limited to VHA therapists who comprised a convenience sample, thereby limiting external validity. Photo narrative is rather new methodology and despite training with participants there was still variation in the narratives. Another limitation was that in a few photos the activity could not be determined.
Research implications
Project findings may serve as a guide for therapists who would like to enhance the use of SPHM equipment in rehabilitation. Additional studies, however, are needed to support SPHM in rehabilitation. Studies have demonstrated equivalent or improved outcomes with SPHM in rehabilitation [7, 12], but many, if not most rehabilitation therapist on units with SPHM do not use the equipment. Patients in rehabilitation can often stand or ambulate with contact guard or minimal assistance and therapists need to use clinical decision making skills when manual handling in these high functioning cases [8]. Future studies should focus specifically on therapy tasks that that should use equipment because of the worker safety concerns to examine the effect of SPHM on patient outcomes. To demonstrate the efficacy of SPHM in rehabilitation, we recommend a pragmatic, cluster randomized trial where facilities with SPHM rehabilitation programs are compared to facilities without SPHM rehabilitation programs.
Current findings build on existing, albeit scant, research to date that focuses on processes and outcomes related to the use of SPHM equipment in rehabilitation. Leaders in the field have noted that while the evidence is clear that SPHM reduces musculoskeletal injuries among nurses and other direct care staff [27], more research is needed to document the association between SPHM programs and patient outcomes and therapist safety outcomes [3].
Conflict of interest
The authors declare that they have no conflicts of interest.
Disclaimer
Contents do not represent the views of the Department of VHA or the United States Government.
Source of funding
Funding was provided by VA, VISN 8 Patient Safety Center of Inquiry, James A Haley Veterans’ Hospital and Clinics.
Footnotes
Acknowledgments
We are thankful for the work of the 17 participants, whose ingenuity and persistence made this project possible. There were many more therapists who participated in this project by staging equipment, taking pictures, posing in pictures and discussing narratives. We are grateful to these VHA therapists. We also wish to recognize and thank Tatjana Bulat, MD, Director of the VISN 8 Patient Safety Center of Inquiry for her support and continued interest in this project. Thank-you to our colleagues, Margeaux Chavez, MA, MPH for setting up the coding documents and Anita Ramrattan, DPT for helping with therapy language.