
Abstract
BACKGROUND:
Work-related health problems result in an economic loss of 4–6% in GDP (Gross domestic Product) of the most countries. In the industrialized countries, 1/3rd of the health-related absence to duty are due to musculoskeletal disorders. Professional driving is one such occupation which looks like sedentary occupation, but involves many risk factors that contribute to work-related musculoskeletal disorders (WMSD) due to its nature of working and work environment. This research describes the various risk factors associated with WMSDs and their effects on drivers health.
OBJECTIVE:
To assess the prevalence of WMSD and its associated risk factors among the bus drivers of Karnataka State Road Transport Corporation (KSRTC), Karnataka.
METHODS:
Subjects considered in this study are 301 full-time bus drivers from the central division KSRTC which consists of 6 depots in Bengaluru. Information regarding reported WMSD symptoms during immediate past 7 days to 12 months, the intervention of WMSD in their day-to-day life and the overall comfort of the body are determined through Standardized Nordic Questionnaire and also by direct observation. The survey questionnaire is conducted by face to face interview.
FINDINGS:
From the statistical analysis, it is found that around 55.8% of the study population has experienced WMSD. The prevalence of WMSD is most common in the age group of 29–39 years (53.5%) followed by the age group of >40 years.
CONCLUSION:
In this study, some of the work-related and lifestyle/health-related factors show significant association with WMSD in bus drivers of Karnataka. Musculoskeletal disorders can be prevented by designing the driver’s workspace ergonomically so that the design suits to all sorts of drivers and the drivers should also be trained on basics of vehicle ergonomics (posture, seat adjustments, in-vehicle controls adjustments).
INTERPRETATION:
KSRTC should educate drivers on the basics of vehicle ergonomics, harmful use of tobacco/alcohol, unhealthy food habits and also to involve in physical exercise at least 75–150 mins weekly. If not, the trend of drivers suffering from WMSD belonging to mid-age will increase exponentially.
SCOPE FOR FUTURE WORK:
Statistical result and direct observation insist on undertaking further studies on ergonomic interventions at driver’s cabin, lifestyle/occupational health factors which mitigate WMSD in different parts of the body during driving.
Introduction
Musculoskeletal disorders denote the health problems of locomotor apparatus [1]. The functional capacity of musculoskeletal systems depends on the proper activation of muscles [2]. MSDs may be due to a strain in muscles, a rupture in tendons/ligaments/muscles or a fracture in bones or due to degenerative changes [3]. Professional drivers are vulnerable to MSDs. Work-related MSDs among professional drivers is one of the major reasons for the early retirements [4]. Compared to other sedentary tasks driving is considered as the most stressful and unhealthy occupation [5]. This is because a driver has to perform defensive driving task considering the safety of occupants in the bus, safety of the vehicle, safety of other road users and also needs to follow the traffic rules and guidelines of the organization for which the driver is working [6]. Driver seat is located near the front suspension and bolted to the floor panels of the vehicle. The driver becomes an integral part of the vehicle at the seated position during driving. The main interface between the driver and the vehicle is the seat, steering wheel, and other in-vehicle controls. The driver experiences vibrations from various transfer paths like seat bolt attachments to floor panels, armrest, accelerator, brake pedal, clutch and also through the steering wheel.
Ergonomic considerations in vehicle design will directly influence the chances of getting WMSDs in professional drivers [7, 8]. Long time exposure of the human body to vehicle vibrations will cause severe WMSDs [9, 10]. Absenteeism, health issues, and less productivity in professional drivers are due to WMSDs, predominantly low back pain (LBP) [11, 12]. The risk of LBP increases with the increase of the risk factors in the working environment [13]. Several researchers have come across the prevalence of WMSDs and their associated risk factors among professional drivers. Major results drawn from the earlier researches are related to LBP followed by higher prevalence of MSD in lower extremities, and the least frequent body sites are arms and wrist regions [14]. Risk factors like age, BMI, total driving hours, shift timings will also contribute to WMSDs [15, 16]. Generally, professional drivers overcome the pain due to MSDs using easily available drugs like painkillers (diclofenac) without the doctor/physician consultation and prescription [17, 18]. QI spine clinic research suggests that the painkillers used by drivers will suppress the symptoms and will not cure the disorders in the body. Employees at Karnataka State Road Transport Corporation (KSRTC) suffering from illness mentioned in disability ACT-1995 (organizational constitution) with more than 40% disability due to WMSDs and accidents are accommodated by providing alternative job or light duty. The present work aims to identify the associated risk factors contributing to the prevalence of WMSD’s among the professional bus drivers of Karnataka, Southern part of INDIA. The association of sociodemographic, work-related, lifestyle and health factors which cause MSDs are identified by assessing the frequency of MSDs.
Subjects and methods
Selection of sampling size
Presently KSRTC has 10948 drivers. Questionnaire survey is done in Central Division of KSRTC which has 1295 drivers among which 85 drivers are aged above 55 years. Only 1210(N) drivers are considered as the total population for which sample size is 300.62 (n). Finally, n = 301 drivers are considered as the sample size. The sample size was calculated by using Yamane formula.
Where,
n-Sample size
N-Population Size
e-Sampling error (0.05)
Subjects selected in this study are directly recruited through KSRTC, and all are full-time bus drivers. These drivers perform 8–10 hours of driving job daily with six days on and one day off. Initially, the study targeted a total of 450 drivers. Later depending upon proper response to the questionnaire and active participation, 301 drivers in the age group between 24–55 years are considered for the study of WMSDs. Drivers with chronic disease and traumatic injuries in their muscular-skeletal systems, who have met with accidents several times and who have crossed >55 age limit have been discarded from the study.
Ethical consideration
The MNMQ (Modified Nordic Musculoskeletal Questionnaire) is checked and approved by the superintendent of administration, depot managers and divisional controller (DC) of KSRTC, central division, Shantinagar, Bengaluru.
Pilot survey
Initially 10% of the study samples are informed regarding the purpose of the study and are handed over with the questionnaire forms prepared in the local language. Drivers are individually asked whether all the questions framed fulfill the nature of the study to identify the prevalence of WMSD’s. Based on the feedback, the questionnaire is modified, and the study conducted.
Data collection
During the study, the data are collected from face to face interview with the help of questionnaires and also by direct observation. Questions framed are based on Modified Nordic Musculoskeletal Questionnaire (MNMQ) [19, 20]. Driver’s opinion, experience, and incidents happened earlier are taken into consideration while studying the associated risk factors of driving. The questionnaire consists of three sections a). Socio-demographic information b). Occupational/Behavior/Lifestyle Information c). Medical/Health (history) information. The first section includes information about gender, age, height, weight, marital status, work experience, shift timings. The second section covers the information on seat adaptability, ease of egress/ingress, micro breaks, body bending and repetitive tasks, the reachability of in-vehicle controls, stress at work, force exertion on vehicle controls, ORVM (Outside Rear View Mirrors) visibility, smoking/ tobacco consumption, and drinking habits. The third section has information regarding the overall discomfort of the body, prevalence of MSD’s from past 7 days to 12 months and their inference in the day to day activities. The first section of the questionnaire has multiple choices to record the response of the participants. The second section has ‘yes’ or‘no’ type of responses, and the third section has body charts to identify the regions, and to record the response related to WMSDs. It also has Likert scale method of following four choices: comfortable, very comfortable, uncomfortable and very uncomfortable to evaluate the overall discomfort of the body. Data collection and investigation of WMSDs are carried out for only male bus drivers (n = 301).
Data analysis
Response from the subject is entered in the questionnaire form, and these responses are coded suitably to analyze with suitable tools. The tool used for this study is SPSS version 20.0. Data analysis is performed using chi-square test which is commonly used to assess the relationship between independent and dependent variables. Independent variables considered in this study are socio-demographic, lifestyle/behaviors/occupational information’s, whereas reported musculoskeletal complaints are considered as a dependent variable. χ2 test results (with 95% confidence intervals) of p < 0.05 are considered statistically significant. Prevalence (%) of WMSDs during last 12 months and last 7 days are identified. The overall discomfort of the body and prevalence of WMSDs in different age group and also based on work experience are examined from various anatomical sites like the neck, shoulder, lower/upper back, and in lower extremities.
Results
General information
The sample for the study consisted of 301 male bus drivers. 8.31% belong to 24–28 age groups, 47.18% belong to 29–39 age group, and 44.5% belong to >40 age group. Mean height, weight, and age of the participants are 5.5”, 73.4 kg and 39 years (SD±7.3) respectively. The government of Karnataka (GoK) has mandated 24 yrs as the minimum age limit with intermediate/PU (pre-university) as the minimum education qualification for driving job. 66.11% have completed PU, 24.58% have completed diploma/degree, and rest have completed basic education up to class X. 93.40% of drivers in the sample study are married, and 6.60% are unmarried. 10.30% of drivers work in the first shift, 54.15% work in the second shift and 35.55% work in general shift. It is found that 9.63% of drivers have maintained good health with no WMSD history; rest has average health status and had a history of WMSDs. 56.15% of drivers involved in tobacco consumption/smoking and drinking habits and 16.28% of drivers involved in game activities during free time. Almost half of the study sample responded that they feel muscle fatigue during driving and lack of strength due to routine work. During the year 2017–18, 65 cases of drunken while on duty were detected and fined among 45,186 checks. In 2016–17, 57 drivers are treated for alcoholism spending Rupees 8,000/person ($110 approx.) for de-addiction. Anti-tobacco signature program and WAPPA (Workplace Alcoholic Prevention Program Activity) are conducted by KSRTC from 1997 to create awareness and educate drivers to maintain their health. KSRTC has setup preventive medicine and healthy lifestyle clinic at Mysuru, India in which 3933 drivers have undergone health checkup during 2016–17. It is found that 5.98% drivers are underweight, 53.16% are normal weight, 39.87% are overweight, and 1.00% are obese. From the survey, it is found that 7% of drivers have undergone piles operation, 4.5% have undergone various heart surgeries, and 3.5% have undergone treatment for minor and major injuries.
Work and workplace characteristics
KSRTC is a state government road transport organization. It is one of the best government organization in Asia, which has bagged more than 150 state, national and international awards for its best practices and service in the transport sector. KSRTC, named after MGRTD (Mysore Government Road Transport Department) was inaugurated with 120 buses on 12th September 1948. Presently there are approximately 10,948 drivers and 2912 conductors and also 12,851 drivers cum conductors (D/C) working in KSRTC. The organization has headquarters in Bengaluru, consists of a central division, which has six depots within the district (Bengaluru). KSRTC operates on 5899 daily routes covering more than 29, 07,752 kms.
Employment crunch draws more people to driving job to support their family financially. Recent job notification (December 5th, 2017) has 500 posts for drivers in KSRTC for which 33,191 aspirants have submitted their application to the organization. KSRTC offers rupees 10,000/per month ($147 approx.) for selected candidates with 2 years of training. KSRTC has introduced “Traffic Revenue Incentive Scheme “in which 3% of traffic revenue collection per day is shared equally among drivers and conductors for city and sub-urban services and 2% of traffic revenue for ordinary, express and luxury services. The central division operates more than 96 routes targeting to cover 50–51 thousand km daily among which shortest route covers 272 km (Mysore-Bengaluru) and longest covers 1384 km (Bengaluru-Srisailam). The daily workload for the drivers includes collecting the route sheet (Routes will be allotted based on the seniority and options available in the routes) and allotted bus for the prescribed route. The driver has to complete the scheduled route within prescribed time with 363 kms/50 litre of diesel.
It is observed that no driver is using seat belts while driving. Moreover, the belts are removed in almost all the buses. Many buses are fitted with ORVMs (outside rearview mirrors) which are smaller in size and require more tilt angle for the torso region to view those mirrors. Pollution control board of Karnataka has recorded the average sound pressure of 86 dB in busy streets of Bengaluru which is higher than the government norms. Honking and busy traffic noise along with vehicle (bus) sound (due to powertrain and road noise) induces stress in drivers. Inhaling the CO (carbon monoxide) in traffic signals causes less oxygen supply to the brain and causes headaches, dizziness, chest pain, and confusion. Sound pressure of greater than >65 dB causes release of hormones in the body that induce stress [21]. From the study, it is found that 55.15% drivers involved in prolong sitting, 51.50% have seat adaptability issue, 20.67% does not have job satisfaction, 63.79% have stress due to tight work schedule and traffic congestion, 89.04% have depended on outside food. 53.82% have no proper access to restrooms and drinking water facility at the workplace, 39.20% have exposed to vibration due to vehicle and road conditions, and 70.83% have faced egress/ingress issues.
Prevalence of WMSDs from past 7 days
Participants reported symptoms with intensity (high and very high), and frequency (often and very often) are considered as participants suffering from MSDs. During the last 7 days drivers have experienced symptoms in neck (2%), shoulder (6.6%), upper arm (2.6%), forearm (0.9%) upper back (11.6%), lower back (21.59%), hip/buttocks (8.6%), thighs (9.3%), knees (23.9%) and ankle/foot (9.3%). It was found that there are fewer symptoms experienced by subjects in hand/wrist (0%) and fingers (0%). The prevalence of WMSDs based on body region is detailed in Table 2.
Prevalence of WMSDs from past 12 months
During the past 12 months, subjects have experienced symptoms in neck (6%), shoulder (24.2%), upper arm (7.6%), forearm (12.6%), hand/wrist (2.6%), finger (1.9%), upper back (23.92%), lower back (11.2%), hip/buttocks (15.9%), thighs (17.9%), knees (37.2%) and ankle/foot (16.2%). It is observed that the symptoms experienced from subjects are more in lower extremities like knees, upper and lower back symptoms pre dominants in upper extremities. Table 1 summarizes overall results of the study which mainly focus on the factors affecting the prevalence of WMSDs. It is also observed that no significant difference has been found in independent variables such as marital status, height, education, posture training, work satisfaction, work interest, involvement in game activities. Table 3 gives the descriptive statistics on the prevalence of WMSDs for last 12 months. Factors like age, seat adaptability, prolong sitting, body bending, active breaks, BMI, current health status, risky driving job are found to be statistically significant.
Association of Socio-demographic, lifestyle/health and work related factors and reported musculoskeletal disorders (n = 301)
Association of Socio-demographic, lifestyle/health and work related factors and reported musculoskeletal disorders (n = 301)
n = number of samples. df = degrees of freedom. x2 = Chi-square value. pa = Significant/non-significant values.
Site wise distribution of participants on prevalence of WMSD’s from past 7 days
Site wise distribution of participants on prevalence of WMSD’s from past 12 months
Table 4 depicts the interference of WMSDs in daily activities. The response consists of 3 choices like “Not at all,” “slightly interfered” and “substantially interfered”. Slightly interfered MSDs will cause acute and painful injuries, which can be avoided by involving in physical activities, maintaining proper food diet and with little medical care. Substantially interfered MSDs will cause chronic and lingering injuries and this type needs intensive medical care. Highest discomfort/pain/fatigue interference are identified in a shoulder (13.2%), lower back (3.6%), knees (13.9%) and ankle/foot (10.6%). From the study, it is found that there is very less intervention of pain hand/wrist and fingers during daily activities.
Descriptive statistics on interference of discomfort in daily activities
Descriptive statistics on interference of discomfort in daily activities
The prevalence of WMSDs based on age group is shown in Fig. 1. It is determined that age contributes to MSDs in drivers. It can be concluded that WMSDs in the predominant age group 30–40 years when compared to other age groups. For the age group of 30–40 years, the highest prevalence is reported in shoulder (9.3%), lower back (14.6%), hip/buttocks (6.3%), knees (10.9%) and ankle/foot (2.6%). For the age group of >41 years highest prevalence is in lower back (15.2%), shoulder (6.6%) and knees (6.6%). For the age group 24–28 years, highest prevalence was reported in lower back (3.3%).

Prevalence of WMSD’s based on age group in past 12 months.
The prevalence of WRMSDs based work experience is detailed in Fig. 2. The highest occurrence is reported in drivers having 11–15 years’ experience. The regions identified are shoulder (0.6%), forearm (4%), upper back (11.2%), lower back (6.6%), thighs (2.6%), knees (8.6%). The second highest prevalence is reported in drivers having 6–10 years’ experience and the identified anatomical sites are knees (10.9%), lower back (5.3%), upper back (5.3%). Drivers having <5 years and >16 years work experience have reported less prevalence of MSD’s.

Prevalence of WMSD’s based on work experience in past 12 months.
The response from the subjects regarding the overall discomfort of the body is depicted in Fig. 3. Responses are based on the Likert scale which has four choices to select. Subjects were asked to respond by showing the graphical representation of the body. Based on the response it is seen that shoulder (36.5%), lower back (50.1%) and knees (40.1%) lies in the extremely uncomfortable category, whereas forearm (3.3%), hand/wrist (81.3%), upper arm (71%) lies in the extremely comfortable category.
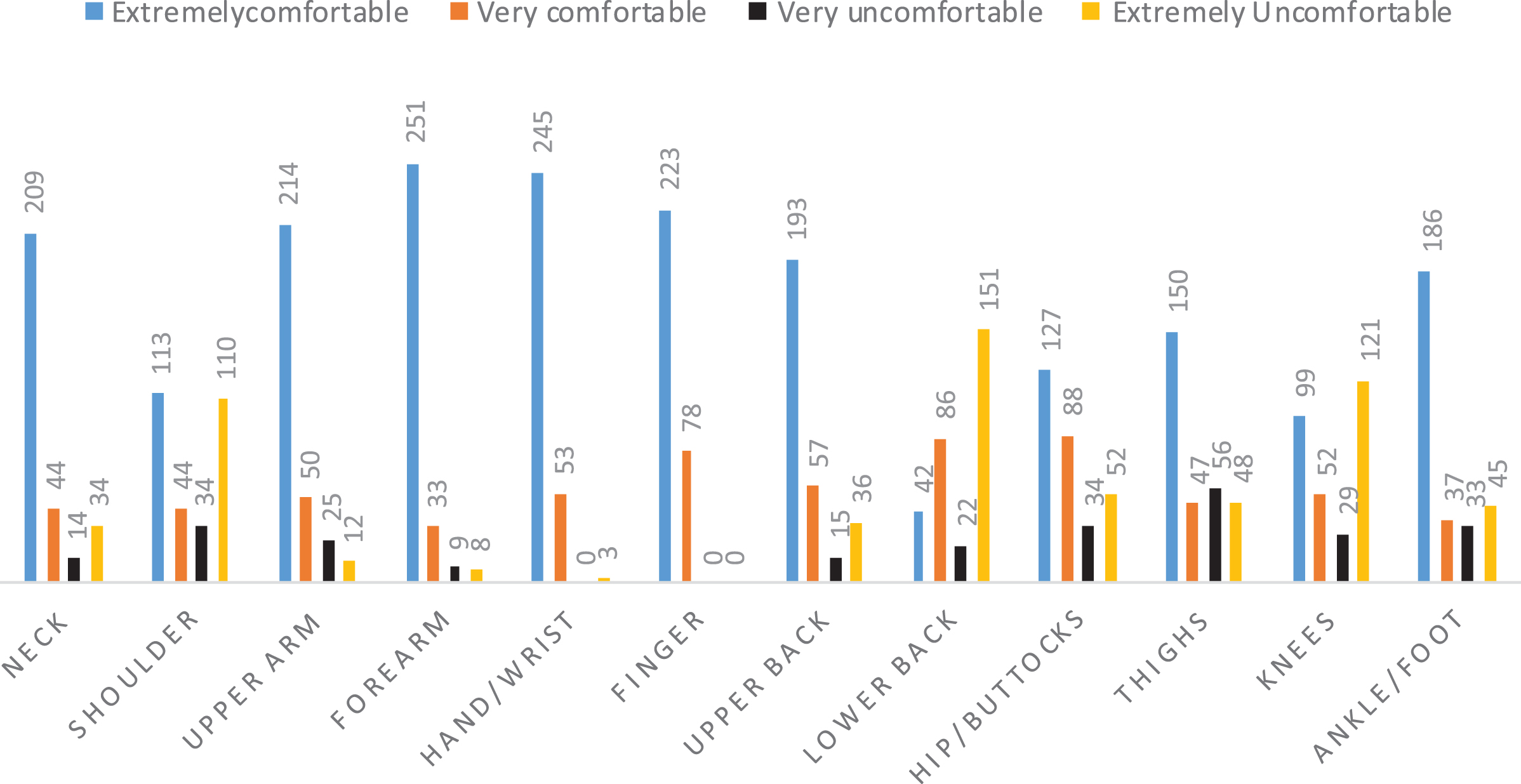
Overall discomfort of the body in past 12 months.
ILO (International Labor Organization) and previous researches have concluded that the prevalence of MSDs in occupational drivers is high when compared to other type of workers due to their working nature. Monotonous jobs of drivers make them vulnerable to WMSDs. The present study conducted and focuses on the associated risk factors of WMSDs and its effects on driver’s health and preventive measures to overcome MSDs in the day to day life. Data analysis in this study has derived some dependent variables of WMSDs like seat adaptability issues (51.50%), involved in prolong sitting (55.15%), involved in body bending task (39.53%), insufficient physical activity/exercise (47.51%), performing repetitive task (50.17%), exposed to vibration (39.205%), feels stress at work (63.79%), insufficient micro-breaks (54.15%), improper access to drinking water and restrooms (53.82%). Almost half of the study sample responded that they are facing seat adaptability issue due to the design of the seat. It is observed during the study that some of the drivers using additional stacking materials (i.e., pillows, blankets and bed covers) for back support, additional cushion effect and to compensate for the height. Seats in KSRTC buses (ordinary) are made up of steel frames knitted with nylon tubes in cushion and backrest area, and there is no headrest. Body parts that come in contact with the seat require cushioning for comfortable driving. Driver cabin should be designed ergonomically so that the seat area should have minimum exposure to heat, glare, noise, and vibration.
MSDs have a strong link with insufficient physical activity [22]. The present research shows that 47.51% of participants are not involved in any physical activity during leisure time. World health organization (WHO) recommends adults to involve in physical activity for at least 150 min/week of moderate intensity exercises or 75 min/week of vigorous intensity physical exercises [23]. Lack of physical activity in daily life of drivers leads to higher risk of hypertension, diabetes and cardiovascular diseases, etc. [24]. Seventy percent of the countries globally have an operational physical activity policy; but their implementation is not effective or nil. China, the most populous country, has effectively implemented, encouraged its people to involve in physical activity during leisure time [25, 26]. In the same way, India should implement national policy referring to the global action plan on physical activity 2018–2030 [27]. There should be a setup such as open spaces, parks in depots and terminals to support drivers to involve in recreation and sports during the leisure time actively [28, 29].
Drivers involving in prolong sitting (55.15%) are vulnerable to low back pain (LBP) and disk pressure [30]. Unfavorable sitting postures influence the LBP and causes overload on muscular skeletal elements [31]. Performing repetitive task in driving causes repeated activations of the same muscles without relaxation [32]. Combination of prolonged sitting, repetitive task and whole-body vibration will lead to irreversible changes in muscle structure [33]. Due to repetitive task lower extremities are under risk due to larger force transfer through spine and legs while applying brake, clutch, and accelerator [34]. From the data analysis, it was observed that 53.82% of the participants have responded that they feel stress at work. Work-related stress is considered as a psychosocial factor for MSDs [35]. Stress in drivers is due to tight route schedule, insufficient micro breaks, traffic congestion, lack of time to address food and toilet needs [36]. Data analysis depicts that stress is a dependent risk factor for MSDs. Very few studies have been conducted to prove that work-related stress is associated with MSDs [37, 38]. Proper health management and reduced work stress will decrease the work-related disorders among the drivers [39]. Excessive stress accumulation can increase the possibility to enhance cancer cells in the body.
Sleep debt in drivers mainly due to regular shift change, extended shift timings (54.15%). Sleep disorders among drivers causes cardiovascular diseases [40]. Drivers are extending shift timings and over time (OT) duty for the additional financial benefits from the organization during other driver’s absence, national holidays and festivals [41]. 64.45% of participants utilize organization rest houses at depots, and some use to sleep in the bus. KSRTC should provide proper accommodation for drivers at depots, bus terminals, and outstations. It was observed that recent trends of dependency on smartphone games and browsing for recreation in leisure time and after duty hours among mid-age drivers is also a reason for sleep debt. Drivers need at least 8 hours of sleep daily to keep up the good health [42]. Sleep debt in driver’s causes fatigue, drowsiness on duty which may lead to accidents, and stress accumulation which in turn reduces the task performance capacity [43].
Jhatkaa, an NGO based in Bengaluru, has conducted the study on air pollution and its effects on the human population. The study shows that Sri Jayadeva Institute of cardiovascular science and research, the largest single center for heart care destination in South East Asia has registered 1000 cases of heart attacks in under 40 age group in April 2017. This study also reveals that the professional drivers exposed to air pollution in urban areas have heart attacks commonly. In the present study also, the drivers belonging to the age group below 40 and having below 15 years of work experience are reported with the highest prevalence of MSDs. The results obtained from the present study can be compared to similar studies conducted on professional bus drivers in different states of India and other countries: Relevant study conducted by Gangopadhyay and Dev [44] on drivers of Kolkata shows (n = 160) that a maximum and their social and professional lives are highly affected due to WMSD’s. 22.9% (n = 667) of drivers in Pondicherry are suffering from low back pain [45]. Aslam et al. [46] conducted a similar study on WMSD’s in bus drivers (n = 273) of Lahore and the results shows that highest prevalence in previous 12 months is in shoulder (33.3%), upper back (16.5%), lower back (15.5%) and knees (12.5%). Szeto and Lam [47] conducted a study on WMSD’s in urban bus drivers on Hong Kong and the result shows that neck, lower and upper back, knees/thighs and shoulder have highest prevalence a rate ranging from 35% to 60% and 90% discomfort was related to bus driving. 45.4% (n = 164) of Israel drivers reported experience of low back pain in the previous 12 months [48]. In the study conducted at Belgaum (North West KSRTC), Karnataka, results shows that 43.3% (n = 365) drivers are overweight and 22.2% are obese [49]. In the present study also, association of BMI with WMSDs is statistically significant.
Conclusion and preventive measures
The present study assessed the prevalence of WMSDs and associated risk factors among the bus drivers of Karnataka State Road Transport Corporation (KSRTC), Karnataka. It was determined that 51.81% of occupational drivers were suffering from WMSDs. The highest prevalence was found in the age group of 30–40 years. Reported prevalence was less when compared to other states in India. Significant factors like age, BMI, prolonged sitting, stress at work, micro breaks contribute to WMSDs in drivers. Using several methods/habits/practices prevalence of WMSDs could be avoided in technical point of view by following the below steps. For hand comfort, drivers should hold the steering wheel at 9 and 3 o’clock position which also avoids vibration to hands. During egress/ingress driver should maintain 3-point support. (It was observed that during the study drivers used to jump from the driver cabin on egress and the reaction force from the ground induces a force on the legs which is 6–8 times greater than the body weight). The driver should adjust the seat to get adequate support to the body. (Mainly for upper back, lower back, thighs, and head). Drivers should avoid the self-medication, mainly painkillers as they only avoid pain signals reaching the brain but not initiate the healing process in the affected region. Drivers should involve in exercise/games/yoga activities before and after work. KSRTC management should conduct initial investigations on ergonomic guidelines adopted in new buses before purchase for the continuous improvement of the driver’s workplace.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We gratefully acknowledge the support and co-operation of the staff members of all six depots of central division KSRTC, Bengaluru.